You might also like
- Incidence of Emergence Agitation and Post-Operative... - Indian Journal of Anaesthesia 2012Document7 pagesIncidence of Emergence Agitation and Post-Operative... - Indian Journal of Anaesthesia 2012song minoNo ratings yet
- Emergency Delirium in PediatricDocument15 pagesEmergency Delirium in PediatricUzZySusFabregasNo ratings yet
- A Randomized Controlled Trial To Determine The.26Document6 pagesA Randomized Controlled Trial To Determine The.26blok etikakedokteranNo ratings yet
- Questionaire StudyDocument5 pagesQuestionaire Studygogih64190No ratings yet
- Ben SonDocument5 pagesBen SonDian NovitasariNo ratings yet
- Apnea After Awake Regional and General Anesthesia in InfantsDocument17 pagesApnea After Awake Regional and General Anesthesia in InfantsmluthfidunandNo ratings yet
- Pauta Enuresis N&ADocument3 pagesPauta Enuresis N&APedro Y. LuyoNo ratings yet
- Clinical Signs and Electroencephalographic.7Document11 pagesClinical Signs and Electroencephalographic.7Mora GalliNo ratings yet
- TMP FDE0Document5 pagesTMP FDE0FrontiersNo ratings yet
- Recovery Characteristics of Total Intravenous Anesthesia With Propofol Versus Sevoflurane Anesthesia: A Prospective Randomized Clinical TrialDocument7 pagesRecovery Characteristics of Total Intravenous Anesthesia With Propofol Versus Sevoflurane Anesthesia: A Prospective Randomized Clinical TrialdennyramdhanNo ratings yet
- Efficacy of Perampanel in Young ChildrenDocument5 pagesEfficacy of Perampanel in Young ChildrenFlavia Angelina SatopohNo ratings yet
- Special Report 2010.xDocument15 pagesSpecial Report 2010.xDianMuliasariNo ratings yet
- Test-Retest Reliability of The English Version of The Edinburgh Postnatal Depression ScaleDocument3 pagesTest-Retest Reliability of The English Version of The Edinburgh Postnatal Depression Scaleevania nitaNo ratings yet
- Sleep Habits and Disturbances in Malaysian Children With EpilepsyDocument5 pagesSleep Habits and Disturbances in Malaysian Children With EpilepsynoiNo ratings yet
- Ijcn 9 024Document8 pagesIjcn 9 024Rio Mulya RihartaNo ratings yet
- Brief Resolved Unexplained Event: Child Health UpdateDocument3 pagesBrief Resolved Unexplained Event: Child Health UpdateNATALIA LEMOS CALLENo ratings yet
- Staring Spells V Epilepsy PDFDocument4 pagesStaring Spells V Epilepsy PDFverdantlawNo ratings yet
- Ferhm Effectiveness of Adenotonsillectomy Vs Watchful Waiting in Young ChildrenDocument17 pagesFerhm Effectiveness of Adenotonsillectomy Vs Watchful Waiting in Young Childrendanielesantos.202019No ratings yet
- 1Document12 pages1Syane TitaleyNo ratings yet
- Predictors of Intractable Epilepsy in Childhood: Case-Control StudyDocument7 pagesPredictors of Intractable Epilepsy in Childhood: Case-Control StudyArdiya OktamaNo ratings yet
- Jurnal THTDocument4 pagesJurnal THTAnggi PrasetyoNo ratings yet
- Clinical Score Adenoid Hypertrophy PDFDocument7 pagesClinical Score Adenoid Hypertrophy PDFjoniindahsariNo ratings yet
- PAPER (ENG) - Swallowing Disturbance Questionnaire For Detecting DysphagiaDocument5 pagesPAPER (ENG) - Swallowing Disturbance Questionnaire For Detecting DysphagiaAldo Hip NaranjoNo ratings yet
- VOTE PSR AnakDocument9 pagesVOTE PSR AnakINGGRID 102015016No ratings yet
- Journal of Clinical AnesthesiaDocument7 pagesJournal of Clinical AnesthesiaNongnapat KettungmunNo ratings yet
- The New York University Pediatric Heart PDFDocument5 pagesThe New York University Pediatric Heart PDFDian IslamiatyNo ratings yet
- Aafp Acute AppaDocument10 pagesAafp Acute AppacarmeliaNo ratings yet
- Development of Refractive Accommodative Esotropia in Children Initially Diagnosed With PseudoesotropiaDocument3 pagesDevelopment of Refractive Accommodative Esotropia in Children Initially Diagnosed With Pseudoesotropialuz mila sanchezNo ratings yet
- Relationship of Dissociated Vertical Deviation and The Timing of Initial Surgery For Congenital EsotropiaDocument4 pagesRelationship of Dissociated Vertical Deviation and The Timing of Initial Surgery For Congenital EsotropiaMacarena AlvarezNo ratings yet
- Pi Is 0149291820302836Document15 pagesPi Is 0149291820302836John SMithNo ratings yet
- Treatment of Strabismic AblyopiaDocument5 pagesTreatment of Strabismic AblyopiaYuke PutriNo ratings yet
- CP Spastic, Diskinetik, AtaxicDocument4 pagesCP Spastic, Diskinetik, AtaxicNura Eky VNo ratings yet
- Anaet 2Document3 pagesAnaet 2hidrisdmnk_747467972No ratings yet
- Efficacy and Safety of Levetiracetam in Pediatric EpilepsyDocument4 pagesEfficacy and Safety of Levetiracetam in Pediatric EpilepsyDian ArdiansyahNo ratings yet
- Arch Dis Child Fetal Neonatal Ed-2005 5876Document6 pagesArch Dis Child Fetal Neonatal Ed-2005 5876Dian NovitasariNo ratings yet
- A.pediatrica para AdultosDocument7 pagesA.pediatrica para AdultosArturo GuilliemNo ratings yet
- Levetiracetam Monotherapy in JuvenileDocument5 pagesLevetiracetam Monotherapy in JuvenileDian ArdiansyahNo ratings yet
- Accommodative Lag Using Dynamic Retinoscopy Age.10Document5 pagesAccommodative Lag Using Dynamic Retinoscopy Age.10JosepMolinsReixachNo ratings yet
- Corticoid EsDocument7 pagesCorticoid EsMaria Gratzia OrdoñezNo ratings yet
- 2011 Efficacy and Augmentation During 6 Months of Double-Blind Pramipexole For Restless Legs SyndromeDocument10 pages2011 Efficacy and Augmentation During 6 Months of Double-Blind Pramipexole For Restless Legs SyndromeAga_tthaNo ratings yet
- Apnea Del PrematuroDocument8 pagesApnea Del PrematuroAndres ChasiNo ratings yet
- Journal Full Ayudita Silvia HasibuanDocument29 pagesJournal Full Ayudita Silvia Hasibuanayudita silvia hasibuanNo ratings yet
- Jurnal 1 Ayudita Silvia HasibuanDocument6 pagesJurnal 1 Ayudita Silvia HasibuanParutigapuluh NovemberNo ratings yet
- Neonatal Seizures Semfetneo2013press-1Document7 pagesNeonatal Seizures Semfetneo2013press-1Vianney Olvera SánchezNo ratings yet
- First-Line Medication Dosing in Pediatricrefractory Status Epilepticus 2020Document14 pagesFirst-Line Medication Dosing in Pediatricrefractory Status Epilepticus 2020Adriana MoroNo ratings yet
- Prednisona Vs ActhDocument7 pagesPrednisona Vs ActhElCanaldeSaadNo ratings yet
- Apnea After Awake Regional and General Anesthesia in InfantsDocument17 pagesApnea After Awake Regional and General Anesthesia in InfantsUtari Mudhia Arisa PutriNo ratings yet
- Problems of Rational Therapy For Epilepsy During Pregnancy: Mart2802@Document10 pagesProblems of Rational Therapy For Epilepsy During Pregnancy: Mart2802@retnowidi41No ratings yet
- Desvenlafaxine Versus Placebo in The TreatmentDocument12 pagesDesvenlafaxine Versus Placebo in The TreatmentNatalia OlmosNo ratings yet
- Clinical Features and Visual Outcomes of Optic Neuritis in Chinese ChildrenDocument7 pagesClinical Features and Visual Outcomes of Optic Neuritis in Chinese ChildrenklinkasikNo ratings yet
- Retinopathy Cryotherapy Retinopathy Study: Eyes PrematurityDocument5 pagesRetinopathy Cryotherapy Retinopathy Study: Eyes PrematuritySalma HamdyNo ratings yet
- Primer Paper Cambio Alte Por Brue AppDocument32 pagesPrimer Paper Cambio Alte Por Brue AppAndres ChasiNo ratings yet
- Sofer1994 Phediatris Pharmacology and TherapeuticsDocument6 pagesSofer1994 Phediatris Pharmacology and TherapeuticsLorena MendozaNo ratings yet
- Nested Case-Control Study of Children Presenting WDocument6 pagesNested Case-Control Study of Children Presenting Wbilal hadiNo ratings yet
- Electroencephalographic Characteristics in Preterm Infants Born With Intrauterine Growth Restriction 2014 The Journal of PediatricsDocument7 pagesElectroencephalographic Characteristics in Preterm Infants Born With Intrauterine Growth Restriction 2014 The Journal of PediatricsfujimeisterNo ratings yet
- P2 (1) - Kowski AB, Et Al. Epilepsy Behav - 2016 Jan 54150-7.Document8 pagesP2 (1) - Kowski AB, Et Al. Epilepsy Behav - 2016 Jan 54150-7.li chenNo ratings yet
- Tecer 2004 Audiovestibular Functioning in Patients With Panic DisorderDocument6 pagesTecer 2004 Audiovestibular Functioning in Patients With Panic DisorderJuan Hernández GarcíaNo ratings yet
- 2018 Article 1359Document5 pages2018 Article 1359SaskiahNo ratings yet
- 1 s2.0 S0894731723006223 MainDocument52 pages1 s2.0 S0894731723006223 Mainpaul00040No ratings yet
- Thursday / January 2019 Thursday / January 2019Document572 pagesThursday / January 2019 Thursday / January 2019Zie EikinNo ratings yet
- Books & PeriodicalsDocument1 pageBooks & PeriodicalsDebabrat MishraNo ratings yet
- Century Vemap PDFDocument5 pagesCentury Vemap PDFMaster MirrorNo ratings yet
- Executive Summary Report Julio13Document8 pagesExecutive Summary Report Julio13exxgineNo ratings yet
- PUP 200 Quizzes 6Document47 pagesPUP 200 Quizzes 6Nam TranNo ratings yet
- Motion in One Dimension QuestionDocument6 pagesMotion in One Dimension Questionabh_omega33% (3)
- Grade 8 - EnglishDocument2 pagesGrade 8 - EnglishTCHR KIMNo ratings yet
- Interjections NotesDocument2 pagesInterjections NotesKanna ImuiNo ratings yet
- NCR Supplier PPAP Training PresentationDocument166 pagesNCR Supplier PPAP Training PresentationRajeev ChadhaNo ratings yet
- INT PL 2020 Web 01-20 PDFDocument320 pagesINT PL 2020 Web 01-20 PDFAndriana Vilijencova100% (1)
- Unit 1Document90 pagesUnit 1Atul Jaysing PatilNo ratings yet
- Solution PDFDocument20 pagesSolution PDFVard FarrellNo ratings yet
- 01.introduction To Earth ScienceDocument29 pages01.introduction To Earth ScienceIshan Chua100% (1)
- Labour Law Assignment - Gross NegligenceDocument6 pagesLabour Law Assignment - Gross NegligenceOlaotse MoletsaneNo ratings yet
- Chapter 2 Ag - EconDocument7 pagesChapter 2 Ag - EconJay Kenneth Bajar Cernal100% (1)
- Is There Any Way To Download The Whole Package of Asphalt 8 Airborne So That I Can Install It On Any Android Device Without An Internet Connection - QuoraDocument4 pagesIs There Any Way To Download The Whole Package of Asphalt 8 Airborne So That I Can Install It On Any Android Device Without An Internet Connection - QuoraMounir2105No ratings yet
- Lab Report 1Document23 pagesLab Report 1hadri arif0% (1)
- Electromechanical Instruments: Permanent-Magnet Moving-Coil InstrumentsDocument13 pagesElectromechanical Instruments: Permanent-Magnet Moving-Coil InstrumentsTaimur ShahzadNo ratings yet
- An Introduction To EFTDocument24 pagesAn Introduction To EFTkunjammuNo ratings yet
- Relations Between Lean Management and Organizational StructuresDocument12 pagesRelations Between Lean Management and Organizational StructuresRENE JAVIER PACHECO SALASNo ratings yet
- Wish Upon A STAR: Presented By: Daulo, Eunice R. III - Block 3Document17 pagesWish Upon A STAR: Presented By: Daulo, Eunice R. III - Block 3nhyce18No ratings yet
- ENGG 3150 Engineering Biomechanics Lab Guide 2006: University of Guelph School of EngineeringDocument13 pagesENGG 3150 Engineering Biomechanics Lab Guide 2006: University of Guelph School of Engineeringالقداري القداريNo ratings yet
- Spying From Space - Constructing America's Satellite Command and Control Systems (PDFDrive)Document230 pagesSpying From Space - Constructing America's Satellite Command and Control Systems (PDFDrive)MohammadNo ratings yet
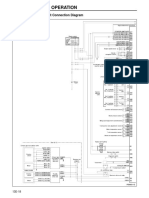
- Structure and Operation: 3. Electronic Control Unit Connection DiagramDocument16 pagesStructure and Operation: 3. Electronic Control Unit Connection DiagramAung Hlaing Min MyanmarNo ratings yet
- Animal Defenses TestDocument3 pagesAnimal Defenses TestNermine MouallemNo ratings yet
- Contractor Hse Management ProgramDocument12 pagesContractor Hse Management ProgramAhmed IbrahimNo ratings yet
- AS400 RPG400 BasicsDocument148 pagesAS400 RPG400 Basicscharaviz84100% (1)
- Chess AI: Competing Paradigms For Machine Intelligence: Shiva Maharaj Nick Polson Alex TurkDocument15 pagesChess AI: Competing Paradigms For Machine Intelligence: Shiva Maharaj Nick Polson Alex TurkDomingo IslasNo ratings yet
- Sect. 4 Tech Docum PC7 AutoLube - 1209 PDFDocument46 pagesSect. 4 Tech Docum PC7 AutoLube - 1209 PDFAlexis MikeNo ratings yet
- Ground Architecture (Mourad Medhat)Document146 pagesGround Architecture (Mourad Medhat)Aída SousaNo ratings yet