You might also like
- Background Verification FormDocument6 pagesBackground Verification FormjobanNo ratings yet
- My NK JoiningDocument24 pagesMy NK Joiningkshv46No ratings yet
- Application Form HCLFC407694Document3 pagesApplication Form HCLFC407694Meenu PalNo ratings yet
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 pagesEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationShankar KhuspeNo ratings yet
- Kotak Joining Kit PDFDocument18 pagesKotak Joining Kit PDFDhiraj SirsatNo ratings yet
- RRB TechnicianDocument2 pagesRRB Technicianak1334660No ratings yet
- Background Screening Form Updated (2) (2 Files Merged)Document8 pagesBackground Screening Form Updated (2) (2 Files Merged)ASHISH OJHANo ratings yet
- DFCCIL FormDocument5 pagesDFCCIL Formabhishekmani014No ratings yet
- Checklist Report V1Document22 pagesChecklist Report V1Anil kadamNo ratings yet
- B. K. Birla College: of Arts, Science and Commerce (Autonomous), KALYAN Affiliated To University of MumbaiDocument2 pagesB. K. Birla College: of Arts, Science and Commerce (Autonomous), KALYAN Affiliated To University of Mumbaimanoj phadtare0% (1)
- ApplicationForm 41268Document17 pagesApplicationForm 41268Sagar PitalaNo ratings yet
- Httpskotakstpxpress - My.salesforce Sites - Comrecordid 00QHG000001oqFO2AYDocument1 pageHttpskotakstpxpress - My.salesforce Sites - Comrecordid 00QHG000001oqFO2AYManjunath ShettyNo ratings yet
- Form ECIL PDFDocument3 pagesForm ECIL PDFFloydCorreaNo ratings yet
- LoanApplicationFormDocument4 pagesLoanApplicationFormpokeNo ratings yet
- Application Form CGMDocument4 pagesApplication Form CGMantoNo ratings yet
- DFCCIL FormDocument5 pagesDFCCIL Formvenkateshwarareddy siddavatamNo ratings yet
- CRPF Form 2023Document4 pagesCRPF Form 2023Krishna SinghNo ratings yet
- Miss Suman Rajnath Yadav: Prudent Corporate Advisory Services LTDDocument8 pagesMiss Suman Rajnath Yadav: Prudent Corporate Advisory Services LTDPramod YadavNo ratings yet
- Hindustan Copper Limited: Application Form No.: 06estt/1/2005/2018043372018Document2 pagesHindustan Copper Limited: Application Form No.: 06estt/1/2005/2018043372018Zainuddin AnsariNo ratings yet
- PDF ApplicationformDocument5 pagesPDF ApplicationformcscsrisakthiNo ratings yet
- Print PDFDocument5 pagesPrint PDFrohan mahadikNo ratings yet
- 3120051913Document1 page3120051913mehekpardeshi100% (1)
- RrbrahulDocument2 pagesRrbrahulauebajcuahdhNo ratings yet
- Services Selection Board - Jammu & KashmirDocument3 pagesServices Selection Board - Jammu & KashmirAshiq RazaviNo ratings yet
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument3 pagesEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationMayuresh DalviNo ratings yet
- USGI Application Form-2Document3 pagesUSGI Application Form-2paviliongmatNo ratings yet
- ApplicationForm - KA 017 218276 05137446Document5 pagesApplicationForm - KA 017 218276 05137446neelkantyrajkumar6No ratings yet
- Employees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of RegistrationDocument2 pagesEmployees' State Insurance Corporation E-Pehchan Card: Insured Person: Insurance No.: Date of Registrationआनंद चव्हाणNo ratings yet
- Rrbapply - Gov.in # Pscexamservice Candidate View Application Id 5b48e839 C9a4 4394 A276 d58b65b3181cDocument2 pagesRrbapply - Gov.in # Pscexamservice Candidate View Application Id 5b48e839 C9a4 4394 A276 d58b65b3181ckalimunda74No ratings yet
- ApplicationForm - WB 001 108617 00286102Document4 pagesApplicationForm - WB 001 108617 00286102anishmistri8333No ratings yet
- Rahuls If HaDocument3 pagesRahuls If HadkopaonopNo ratings yet
- National Pension System (NPS) Subscriber Registration FormDocument2 pagesNational Pension System (NPS) Subscriber Registration FormHarish SabalNo ratings yet
- Customer Application Form: Personal DetailsDocument14 pagesCustomer Application Form: Personal DetailsMalikMDNuraniNo ratings yet
- B. K. Birla College of Arts, Science & COMMERCE (Autonomous), KALYANDocument4 pagesB. K. Birla College of Arts, Science & COMMERCE (Autonomous), KALYANBussiness EmpireNo ratings yet
- Vishwakarma - GJ 017 161521 16799324Document4 pagesVishwakarma - GJ 017 161521 16799324digitaldy52No ratings yet
- SB - Financial Inclusion ACCOUNT OPENING FORM (BC POINT-System Generated)Document2 pagesSB - Financial Inclusion ACCOUNT OPENING FORM (BC POINT-System Generated)reena.msassociatesNo ratings yet
- Personal Details: 22001448 Sonu Antony Antony Joseph Gracy Antony Indian No Male 20/aug/1994Document5 pagesPersonal Details: 22001448 Sonu Antony Antony Joseph Gracy Antony Indian No Male 20/aug/1994Sonu AntonyNo ratings yet
- B. K. Birla College of Arts, Science & COMMERCE (Autonomous), KALYANDocument4 pagesB. K. Birla College of Arts, Science & COMMERCE (Autonomous), KALYANBussiness EmpireNo ratings yet
- RRB FormicatinDocument2 pagesRRB Formicatingyaniprasad49No ratings yet
- FSSAI Form 2021Document5 pagesFSSAI Form 2021ShivamNo ratings yet
- CRPF Form 2023Document4 pagesCRPF Form 2023Om prakash JatNo ratings yet
- Admission FormDocument4 pagesAdmission FormprathmeshNo ratings yet
- Government of Gujarat: Student Basic DetailsDocument2 pagesGovernment of Gujarat: Student Basic DetailsVAV PPPNo ratings yet
- CRPF Form 2023Document4 pagesCRPF Form 2023ravisharma.rs80216No ratings yet
- Personal Details: Customer Profile FormDocument3 pagesPersonal Details: Customer Profile FormAdarsh SinghNo ratings yet
- Applicant Details: Applicant Photo Applicationid:1920Vjb1000126794Document6 pagesApplicant Details: Applicant Photo Applicationid:1920Vjb1000126794Niraj PatilNo ratings yet
- Recruitmentrrb - in # Pscexamservice Candidate View Application Id Abddbdd7 0c2e 49ce A9f9 c00059f2035dDocument2 pagesRecruitmentrrb - in # Pscexamservice Candidate View Application Id Abddbdd7 0c2e 49ce A9f9 c00059f2035dsajjankumarraj0No ratings yet
- E-Employment Application Form - Updated 011122Document8 pagesE-Employment Application Form - Updated 011122ZHEN WEI WONGNo ratings yet
- Suresh Kumar RajendranDocument3 pagesSuresh Kumar RajendranSURESH KUMAR RNo ratings yet
- Interview Personal Detail Form: Source of Hire (Please Choose One of The Below and Add The Relevant Details)Document10 pagesInterview Personal Detail Form: Source of Hire (Please Choose One of The Below and Add The Relevant Details)dharshan rajNo ratings yet
- ApplicationForm - JK 017 007053 21246689Document4 pagesApplicationForm - JK 017 007053 21246689anshudevi91499No ratings yet
- Assistant District Attorney in Prosecution Department Haryana - Preview ApplicationDocument2 pagesAssistant District Attorney in Prosecution Department Haryana - Preview ApplicationMazid KhanNo ratings yet
- Background Verification FormDocument6 pagesBackground Verification FormpritamjaanNo ratings yet
- Applicant Details:: Online Account Opening / Applicant Information Form For Resident IndividualsDocument4 pagesApplicant Details:: Online Account Opening / Applicant Information Form For Resident IndividualsDinesh sakharam GawaliNo ratings yet
- Customer Application Form: Personal DetailsDocument16 pagesCustomer Application Form: Personal DetailsSantosh creationsNo ratings yet
- Personal Details: Customer Profile FormDocument3 pagesPersonal Details: Customer Profile FormJannat 9163No ratings yet
- Customer Application Form: Personal DetailsDocument19 pagesCustomer Application Form: Personal DetailsAKNo ratings yet
- Employees State Insurance Corporation Temporary Identity CertificateDocument1 pageEmployees State Insurance Corporation Temporary Identity CertificateGauravNo ratings yet
- Rrbapply - Gov.in # Pscexamservice Candidate View Application Id 73274021 f0c2 4f51 94ba 570c4c0ef02fDocument2 pagesRrbapply - Gov.in # Pscexamservice Candidate View Application Id 73274021 f0c2 4f51 94ba 570c4c0ef02fIT96 Sajal choubeyNo ratings yet
- Computerised Payroll Practice Set Using MYOB AccountRight: Australian EditionFrom EverandComputerised Payroll Practice Set Using MYOB AccountRight: Australian EditionNo ratings yet
- KMB CEC Pre Joining Learning AdvisoryDocument11 pagesKMB CEC Pre Joining Learning AdvisoryVineesha GurnaniNo ratings yet
- Chapter-4 Elasticity of DemandDocument38 pagesChapter-4 Elasticity of DemandVineesha GurnaniNo ratings yet
- Production Function, ISO-quants and Economies of ScaleDocument57 pagesProduction Function, ISO-quants and Economies of ScaleVineesha GurnaniNo ratings yet
- PDFDocument5 pagesPDFVineesha GurnaniNo ratings yet
- Following Annexure Has To Be Put On First Page of The PresentationDocument48 pagesFollowing Annexure Has To Be Put On First Page of The PresentationVineesha GurnaniNo ratings yet
- Cost Accounting MCQs End TermDocument7 pagesCost Accounting MCQs End TermVineesha GurnaniNo ratings yet
- Strategic MGMT MCQs - End TermDocument10 pagesStrategic MGMT MCQs - End TermVineesha GurnaniNo ratings yet
- Starbucks Business Ethics Case StudyDocument9 pagesStarbucks Business Ethics Case StudyLovely Sweety Ghosh100% (1)
- Daily ChecklistDocument1 pageDaily ChecklistPatel AspNo ratings yet
- Advanced Industrial and Labour Relations - Assignment 2Document4 pagesAdvanced Industrial and Labour Relations - Assignment 2Matthew MhlongoNo ratings yet
- January 20Document48 pagesJanuary 20fijitimescanadaNo ratings yet
- Expatriates Law in IndiaDocument26 pagesExpatriates Law in IndiaBabli JhaNo ratings yet
- Labour Law-Ii Important Questions:: Page 1 of 21Document21 pagesLabour Law-Ii Important Questions:: Page 1 of 21Shailan AliNo ratings yet
- Work - Life - Work Balance by Andrew Maynard - ArchDailyDocument25 pagesWork - Life - Work Balance by Andrew Maynard - ArchDailylovnishNo ratings yet
- Economic Instructor ManualDocument28 pagesEconomic Instructor Manualclbrack100% (9)
- Apprenticship PDFDocument102 pagesApprenticship PDFDr. Isha SharmaNo ratings yet
- EPHRM Course Details - PDF - IIMDocument4 pagesEPHRM Course Details - PDF - IIMSandeep Ghai0% (1)
- Module No 7 - Manufacturing Overhead AccountingDocument3 pagesModule No 7 - Manufacturing Overhead AccountingRafols AnnabelleNo ratings yet
- What Is A Cover Letter For A Job? Definition, Purpose, MeaningDocument4 pagesWhat Is A Cover Letter For A Job? Definition, Purpose, Meaningflying ostrichNo ratings yet
- Chapter 20, 21 & 22Document18 pagesChapter 20, 21 & 22sk001100% (1)
- MGT103 C5Document3 pagesMGT103 C5Bacquial, Phil Gio E. (Phil Gio)No ratings yet
- Performance Appraisal Methods - Traditional & Modern - Short NotesDocument4 pagesPerformance Appraisal Methods - Traditional & Modern - Short NotesHugh JackmanNo ratings yet
- Cases Legal EthicsDocument33 pagesCases Legal EthicsMark Genesis Alvarez RojasNo ratings yet
- HR Manual Dasra CompanyDocument31 pagesHR Manual Dasra CompanySidhesh TodarmalNo ratings yet
- Checklist - New Hire Onboarding ChecklistDocument8 pagesChecklist - New Hire Onboarding Checklistsaurabh mishraNo ratings yet
- Office Assistant Resume SkillsDocument4 pagesOffice Assistant Resume Skillse79svncm100% (1)
- Re-Hiring of EX-Employees PolicyDocument2 pagesRe-Hiring of EX-Employees PolicyBadal BhattacharyaNo ratings yet
- Case Studies Chapterwise SPCC PDFDocument15 pagesCase Studies Chapterwise SPCC PDFNavya100% (1)
- Paper - 4: Cost Accounting andDocument56 pagesPaper - 4: Cost Accounting andemmanuel JohnyNo ratings yet
- Chapter#3 SocializationDocument46 pagesChapter#3 SocializationSadakalo ShopnooNo ratings yet
- Social MobilityDocument11 pagesSocial MobilityAnonymous n8GJm7wRNo ratings yet
- Labor Standards and Labor RelationsDocument71 pagesLabor Standards and Labor RelationsCacaCamenforteNo ratings yet
- Apa ch20 PDFDocument21 pagesApa ch20 PDFNBNo ratings yet
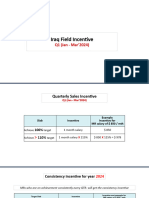
- Iraq Incentive Q1 (Jan - Mar) 2024Document6 pagesIraq Incentive Q1 (Jan - Mar) 2024حسن عباس حسن عباس الغانميNo ratings yet
- Organizational AgilityDocument26 pagesOrganizational AgilityHaitham Mohamed100% (1)
- Human Resource Planning and Employee Productivity in Nigeria Public OrganizationDocument13 pagesHuman Resource Planning and Employee Productivity in Nigeria Public OrganizationKassaf Chowdhury100% (1)
- BCOM 1 Entrepreneurship DevelopmentDocument20 pagesBCOM 1 Entrepreneurship DevelopmentsabirNo ratings yet