You might also like
- Concrete Epoxy HV PDFDocument2 pagesConcrete Epoxy HV PDFGeovanni Mabiscay0% (1)
- TMJ Splints SaherDocument94 pagesTMJ Splints SaherAnkita AgarwallNo ratings yet
- Hepatitis Learning GuideDocument71 pagesHepatitis Learning Guidequimico clinico 27100% (10)
- Intro To GymnasticsDocument69 pagesIntro To GymnasticsMichaela Celerio50% (2)
- ALVEOLAR DISTRACTION OSTEOGENESIS AND IMPLANTOLOGYDocument4 pagesALVEOLAR DISTRACTION OSTEOGENESIS AND IMPLANTOLOGYIJAR JOURNALNo ratings yet
- Biomechanics and orthodontic treatment in maxillofacial distractionDocument9 pagesBiomechanics and orthodontic treatment in maxillofacial distractionHARITHA H.PNo ratings yet
- Distraction Osteogenesis SeminarDocument126 pagesDistraction Osteogenesis SeminarkeerthanNo ratings yet
- Journal of Orthopaedic Science: Hidenori Matsubara, Hiroyuki TsuchiyaDocument8 pagesJournal of Orthopaedic Science: Hidenori Matsubara, Hiroyuki TsuchiyaNeta Aza MaineztNo ratings yet
- Open and Closed Fractures - 2018 EnglishDocument49 pagesOpen and Closed Fractures - 2018 EnglishЕлена КовбасаNo ratings yet
- Treating Bone Deformities With Circular External Skeletal FixationDocument10 pagesTreating Bone Deformities With Circular External Skeletal Fixationtaner_soysurenNo ratings yet
- Bone Transport Distraction Osteogenesis 1Document31 pagesBone Transport Distraction Osteogenesis 1Euginia YosephineNo ratings yet
- 4 Fracture MandibleDocument33 pages4 Fracture MandibleYoussef ElbeharyNo ratings yet
- s-Malunion and nonunionDocument75 pagess-Malunion and nonunionshahnazroeentanmailNo ratings yet
- Manson1974 PDFDocument5 pagesManson1974 PDFharithrra vNo ratings yet
- Dental ArticulatorsDocument10 pagesDental ArticulatorsOmar Al-FatyanNo ratings yet
- Liza RovDocument29 pagesLiza RovCarlos Taito TakahashiNo ratings yet
- Bone FractureDocument23 pagesBone FractureClifford GulfanNo ratings yet
- Distraction Osteogenesis EbookDocument27 pagesDistraction Osteogenesis EbookSundeep SharmaNo ratings yet
- Distraction Osteogenesis of The Maxillofacial Skeleton: Clinical and Radiological EvaluationDocument27 pagesDistraction Osteogenesis of The Maxillofacial Skeleton: Clinical and Radiological EvaluationDevata RaviNo ratings yet
- Ijpi 2 (4) 136-140Document5 pagesIjpi 2 (4) 136-140salman khawarNo ratings yet
- Resective Osseous SurgeryDocument5 pagesResective Osseous SurgeryTania HenriquezNo ratings yet
- Biology of Bone Formation, Fracture Healing, and Distraction OsteogenesisDocument10 pagesBiology of Bone Formation, Fracture Healing, and Distraction OsteogenesisenviNo ratings yet
- Modified distolingual splitting technique for removal of impacted mandibular third molarsDocument7 pagesModified distolingual splitting technique for removal of impacted mandibular third molarsArchanaShenoyNo ratings yet
- Periodontal SurgeriesDocument46 pagesPeriodontal SurgeriesnutacosmynNo ratings yet
- 179-Article Text-302-1-10-20171121 PDFDocument5 pages179-Article Text-302-1-10-20171121 PDFMichael XuNo ratings yet
- Roles of Osteoclasts in Alveolar Bone RemodelingDocument18 pagesRoles of Osteoclasts in Alveolar Bone RemodelingYogi Ajik YNo ratings yet
- Aaid Joi D 14 00023Document6 pagesAaid Joi D 14 00023MohamedAtefNo ratings yet
- Ilizarov TechonlogyDocument41 pagesIlizarov TechonlogyNatalia GonzalezNo ratings yet
- 2.04A Orthopaedic SurgeryDocument11 pages2.04A Orthopaedic SurgeryAnna Mae MarantanNo ratings yet
- Jaw Surgery: Robert M. Menard, Nikhil K. DesaiDocument10 pagesJaw Surgery: Robert M. Menard, Nikhil K. DesaiAlain AguirreNo ratings yet
- 04 - 001 Trauma From OcclusionDocument4 pages04 - 001 Trauma From Occlusiondeepak sharmaNo ratings yet
- Osteogenesis InglesDocument4 pagesOsteogenesis InglesJulio TorresNo ratings yet
- "Distraction Osteogenesis in Orthodontics: A Comprehensive ReviewDocument8 pages"Distraction Osteogenesis in Orthodontics: A Comprehensive ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- 14985-Article Text-29120-1-10-20210409Document6 pages14985-Article Text-29120-1-10-20210409Rakan KhtoomNo ratings yet
- Onodera 2006Document8 pagesOnodera 2006Israel MuñozNo ratings yet
- Periodontal Accelerated Osteogenic OrthodonticsDocument6 pagesPeriodontal Accelerated Osteogenic Orthodonticsyui cherryNo ratings yet
- Musculo Semis MS2Document55 pagesMusculo Semis MS2Miden AlbanoNo ratings yet
- Bone Grafts in Periodontal Surgery - A Review: July 2014Document4 pagesBone Grafts in Periodontal Surgery - A Review: July 2014Fajri AliNo ratings yet
- Artigo ClamshellDocument15 pagesArtigo ClamshellbritocirurgiadamaoNo ratings yet
- Li LBM 4 Blok 18 AnggunDocument8 pagesLi LBM 4 Blok 18 AnggunAnggun Amanda SaveriiaNo ratings yet
- OsteogensisDocument10 pagesOsteogensisDaniela OliverosNo ratings yet
- Distraction OsteogenesisDocument85 pagesDistraction OsteogenesisEdwing Daniel Arias PerezNo ratings yet
- Interocclusal Record (Bite Registration Record)Document10 pagesInterocclusal Record (Bite Registration Record)abdelazizNo ratings yet
- Fundamentals of Occlusion Article PDFDocument6 pagesFundamentals of Occlusion Article PDFIacob Anca MihaelaNo ratings yet
- Implanto Chapter 74-78Document104 pagesImplanto Chapter 74-78whatever200020100% (1)
- 骨科部實習生核心課程 (20160909)Document32 pages骨科部實習生核心課程 (20160909)ChenNo ratings yet
- Bony Exostoses: Case Series and Review of Literature: Acta Scientific Dental Sciences (Issn: 2581-4893)Document4 pagesBony Exostoses: Case Series and Review of Literature: Acta Scientific Dental Sciences (Issn: 2581-4893)Fransiski HoNo ratings yet
- Diskusi Hemifacial Microsomia ItaDocument34 pagesDiskusi Hemifacial Microsomia ItaitaNo ratings yet
- Growth and Development of Temporomandibular JointDocument40 pagesGrowth and Development of Temporomandibular JointSadhu AbhijeetNo ratings yet
- TMD & Its Role in Orthodontics "TMD An Entity Affecting Every Aspect of Life" A ReviewDocument6 pagesTMD & Its Role in Orthodontics "TMD An Entity Affecting Every Aspect of Life" A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Full Mouth Rehabilitation-Part 2: Presentor: Dr.G.ManasaDocument118 pagesFull Mouth Rehabilitation-Part 2: Presentor: Dr.G.Manasabharathi krishnaNo ratings yet
- Occlusal Splints in TMJ RXDocument14 pagesOcclusal Splints in TMJ RXspu123No ratings yet
- Artrodesis RodillaDocument5 pagesArtrodesis RodillaMom of twoNo ratings yet
- المستندDocument12 pagesالمستند22368717No ratings yet
- Oral Pathology: Bone Diseases and CherubismDocument218 pagesOral Pathology: Bone Diseases and CherubismJuhiJahan AmanullahNo ratings yet
- Chapterpdf Download635476105037 4Document20 pagesChapterpdf Download635476105037 4Abhishek JhaNo ratings yet
- The Use of A BruxChecker in The Evaluation of Different Grinding Patterns During Sleep BruxismDocument9 pagesThe Use of A BruxChecker in The Evaluation of Different Grinding Patterns During Sleep BruxismJonathan GIraldo MartinezNo ratings yet
- Biology of Orthodontic Tooth MovementsDocument17 pagesBiology of Orthodontic Tooth MovementsDler RaufNo ratings yet
- Wil CK Odon TicsDocument5 pagesWil CK Odon TicsRambabu SatipedakalaNo ratings yet
- Histologic Comparison of Biologic Width Around Teeth Versus Implants: The Effect On Bone PreservationDocument5 pagesHistologic Comparison of Biologic Width Around Teeth Versus Implants: The Effect On Bone PreservationPaul CerdaNo ratings yet
- Fibro-Osseous Lesions A ReviewDocument4 pagesFibro-Osseous Lesions A ReviewInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Ankle Syndesmosis Injuries Diagnosis and TreatmentDocument11 pagesAnkle Syndesmosis Injuries Diagnosis and TreatmentRoger WatersNo ratings yet
- Orthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFrom EverandOrthodontically Driven Corticotomy: Tissue Engineering to Enhance Orthodontic and Multidisciplinary TreatmentFederico BrugnamiNo ratings yet
- Role of Drugs That Affect Renin Angiotensin SystemDocument22 pagesRole of Drugs That Affect Renin Angiotensin Systemash ashNo ratings yet
- Thai Occupational Safety, Health and Environment Act B.E. 2554 (A.d. 2011)Document32 pagesThai Occupational Safety, Health and Environment Act B.E. 2554 (A.d. 2011)DibbaSotaNanaNo ratings yet
- Waleed Alomari CVDocument2 pagesWaleed Alomari CValomari_waleedNo ratings yet
- OTC Drug ListDocument7 pagesOTC Drug ListHong Diem100% (1)
- Understanding the Relationship Between Place and HealthDocument14 pagesUnderstanding the Relationship Between Place and HealtheNo ratings yet
- Corticosteroid: Saut Samuel Simamora Department Ophthalmology Diponegoro University-Kariadi HospitalDocument21 pagesCorticosteroid: Saut Samuel Simamora Department Ophthalmology Diponegoro University-Kariadi HospitalSania NadianisaNo ratings yet
- Guided Noteboo Kin GED10 2 (Mathe Matics in The Modern World)Document5 pagesGuided Noteboo Kin GED10 2 (Mathe Matics in The Modern World)Chenie BatacNo ratings yet
- Fujitsu GeneralDocument51 pagesFujitsu GeneralZubair DarNo ratings yet
- SanCoP7 AgendaDocument2 pagesSanCoP7 AgendaNicolaGreeneNo ratings yet
- Fingertip Injuries Diagnosis, Management and ReconstructionDocument197 pagesFingertip Injuries Diagnosis, Management and Reconstructionokida192No ratings yet
- Water Hammer PDFDocument30 pagesWater Hammer PDFbhavesh shuklaNo ratings yet
- Accessibility POC: October 26, 2017Document7 pagesAccessibility POC: October 26, 2017Ramesh BodukaniNo ratings yet
- NAVAL Hot Tapping Tool User GuideDocument19 pagesNAVAL Hot Tapping Tool User GuidemarconelucenapereiraNo ratings yet
- CHAPTER 3: Toxic Effects of Drugs: Pharmacology Page 1Document1 pageCHAPTER 3: Toxic Effects of Drugs: Pharmacology Page 1Gabriel GonzagaNo ratings yet
- UM16000 Flame Detector Installation Guide EnglishDocument12 pagesUM16000 Flame Detector Installation Guide Englishmohamed.rescoNo ratings yet
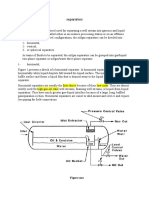
- Separators: Figure OneDocument8 pagesSeparators: Figure OneMohamed Moder100% (1)
- Berca Engineering SUBMITTEDDocument20 pagesBerca Engineering SUBMITTEDJohandika FerbiantokoNo ratings yet
- Notes Form 2 Chapter 4Document4 pagesNotes Form 2 Chapter 4lembu_sihat7783% (6)
- EWC661 TITLE: Dietary Habits During Term Time Among University Students. Background of StudyDocument4 pagesEWC661 TITLE: Dietary Habits During Term Time Among University Students. Background of StudyfarinaazmiNo ratings yet
- Cereal Based Functional BeveragesDocument7 pagesCereal Based Functional BeveragesCorina ParicanazaNo ratings yet
- What Are OPPE and FPPE?Document1 pageWhat Are OPPE and FPPE?adyNo ratings yet
- IED Recognition GuideDocument28 pagesIED Recognition GuideLeafs61100% (5)
- Polythionic Acid Stress Corrosion CrackingDocument2 pagesPolythionic Acid Stress Corrosion CrackingVajid MadathilNo ratings yet
- Color Me VeganDocument272 pagesColor Me VeganBela Luísa Novo100% (1)
- 2 - FNCPDocument5 pages2 - FNCPIlda Lekka RequizaNo ratings yet
- Sprocket Asa 180Document1 pageSprocket Asa 180jhampolrosalesNo ratings yet
- Sydney M PRPDocument23 pagesSydney M PRPapi-465406877No ratings yet