You might also like
- Acid-Base and Electrolyte Handbook for Veterinary TechniciansFrom EverandAcid-Base and Electrolyte Handbook for Veterinary TechniciansAngela Randels-ThorpNo ratings yet
- Cases Acid BaseDocument3 pagesCases Acid BaseSa MoNo ratings yet
- 2017 Refeeding Syndrome A Case Report PDFDocument6 pages2017 Refeeding Syndrome A Case Report PDFManual de VacunaciónNo ratings yet
- Chemistry Case 1: Chem PanelDocument3 pagesChemistry Case 1: Chem PanelangelNo ratings yet
- Dietetic Internship - Major Case Study PresentationDocument61 pagesDietetic Internship - Major Case Study Presentationapi-535934790No ratings yet
- Lactation Ketoacidosis in A COVID - 19 Patient A Case ReportDocument3 pagesLactation Ketoacidosis in A COVID - 19 Patient A Case Reporteditorial.boardNo ratings yet
- 2021 - Elbokl - Severe Caffeine Intoxication Treated With HemodialysisDocument4 pages2021 - Elbokl - Severe Caffeine Intoxication Treated With Hemodialysisamanda lssNo ratings yet
- Guideline Title: Management of Diabetic KetoacidosisDocument9 pagesGuideline Title: Management of Diabetic KetoacidosisJorge Salazar GomezNo ratings yet
- Acid Base 7 2Document31 pagesAcid Base 7 2sarvathaqaryNo ratings yet
- Fluid BalanceDocument28 pagesFluid BalancePragadesh NatarajanNo ratings yet
- L6 Water and Electrolyte BalanceDocument16 pagesL6 Water and Electrolyte BalancecuteNo ratings yet
- HRF Resolved Refractory ItchDocument3 pagesHRF Resolved Refractory ItchLaboratorio de NefrologíaNo ratings yet
- 11.50 DR Stella George, Diabetic and Metabolic EmergenciesDocument49 pages11.50 DR Stella George, Diabetic and Metabolic Emergenciesamir ahmadNo ratings yet
- Data Lab Kasus 1Document3 pagesData Lab Kasus 1Luh Adi KusumaNo ratings yet
- PrintDocument7 pagesPrintJEREMIE FAYE UMALINo ratings yet
- Leino Koivula 2009 Stability of Chemical and Immunochemical Analytes in Uncentrifuged Plasma SamplesDocument3 pagesLeino Koivula 2009 Stability of Chemical and Immunochemical Analytes in Uncentrifuged Plasma SamplestestNo ratings yet
- National Competition Case: ASHP Clinical Skills CompetitionDocument16 pagesNational Competition Case: ASHP Clinical Skills CompetitionHelmiNo ratings yet
- كمستريDocument68 pagesكمستريYaRa HamarshehNo ratings yet
- ART'S DKA TXDocument6 pagesART'S DKA TXphat lippNo ratings yet
- Case Report: An Unconscious Man With Profound Drug-Induced HypoglycaemiaDocument6 pagesCase Report: An Unconscious Man With Profound Drug-Induced Hypoglycaemiagevowo3277No ratings yet
- Atherosclerotic Cardiovascular Disease - Critical CareDocument39 pagesAtherosclerotic Cardiovascular Disease - Critical CareAdolf Benedick Dacanay MalalaNo ratings yet
- Arterial Blood Gas Analysis: Diagnostic ExaminationsDocument5 pagesArterial Blood Gas Analysis: Diagnostic ExaminationsstrawberryNo ratings yet
- By Melese A (Mi) Kalkidan A (Mi)Document38 pagesBy Melese A (Mi) Kalkidan A (Mi)Tegegn LegesseNo ratings yet
- Studi KasusDocument9 pagesStudi KasusWina YustisiaNo ratings yet
- Final Exam Case StudyDocument6 pagesFinal Exam Case StudyLoucil Ursula AranasNo ratings yet
- Diabetic Ketoacidosis (1) SMHGDocument57 pagesDiabetic Ketoacidosis (1) SMHGfmocoyombyNo ratings yet
- Surgery Case History: Ref. Range Result ChemistryDocument2 pagesSurgery Case History: Ref. Range Result ChemistryH MNo ratings yet
- Diagnostic Tests GosayeDocument188 pagesDiagnostic Tests GosayeAbdii TolasaNo ratings yet
- Diabetes Mellitus Case StudyDocument16 pagesDiabetes Mellitus Case Studyapi-351187552No ratings yet
- Physician Con May Abhinav 2022Document28 pagesPhysician Con May Abhinav 2022Abhinav ReddyNo ratings yet
- Case 056: Common Bile Duct Stones (Choledocholithiasis)Document5 pagesCase 056: Common Bile Duct Stones (Choledocholithiasis)ZauzaNo ratings yet
- Case 8 ОкDocument4 pagesCase 8 ОкАбдул Насер МохаммадізмаелNo ratings yet
- Acute Care Case StudyDocument16 pagesAcute Care Case Studyapi-654020776No ratings yet
- Management of Acute Metabolic Acidosis in The ICU Sodium BicarbonateDocument6 pagesManagement of Acute Metabolic Acidosis in The ICU Sodium Bicarbonatecastillojess100% (1)
- Acute Severe Chromium Poisoning After Dermal Exposure To Hexavalent ChromiumDocument3 pagesAcute Severe Chromium Poisoning After Dermal Exposure To Hexavalent ChromiumAlexandra DolhăscuNo ratings yet
- Mycobacteria Cocos PDFDocument6 pagesMycobacteria Cocos PDFMila Fer D. PridonttNo ratings yet
- Lactate Monitoring For Severe Infection and Septic Shock Edit 4Document46 pagesLactate Monitoring For Severe Infection and Septic Shock Edit 4Kusumastuti TutikNo ratings yet
- CH Pre Lecture PN Calculations ComplicationsDocument4 pagesCH Pre Lecture PN Calculations Complicationsyairegtz2No ratings yet
- 000 Nursing School Necessities Cheat SheetDocument3 pages000 Nursing School Necessities Cheat SheetRevNo ratings yet
- Homeostasis - Case StudyDocument2 pagesHomeostasis - Case StudyAlena JosephNo ratings yet
- Its Just HoaxDocument10 pagesIts Just HoaxArkhan HanafiNo ratings yet
- Texas A and M ResultsDocument6 pagesTexas A and M ResultsraisingaddieNo ratings yet
- Bmjcred00509 0023aDocument1 pageBmjcred00509 0023aBilly SandyNo ratings yet
- Friday Seminar 9-23Document28 pagesFriday Seminar 9-23api-609125382No ratings yet
- CC1 11Document2 pagesCC1 11Joshua TrinidadNo ratings yet
- Case Study 5feb14Document6 pagesCase Study 5feb14helenthongNo ratings yet
- Computer-Based Scenario Biochemistry: How To Read Bloods?Document66 pagesComputer-Based Scenario Biochemistry: How To Read Bloods?Haytham KhalifaNo ratings yet
- Case Report: Ni Ketut Puspa Sari DR - IDA Putri Wirawati, SP - PK (K)Document12 pagesCase Report: Ni Ketut Puspa Sari DR - IDA Putri Wirawati, SP - PK (K)ekaNo ratings yet
- Rhabdomyolysis Case Study WeeblyDocument18 pagesRhabdomyolysis Case Study Weeblyapi-241865788No ratings yet
- Calcium-Phosphate Metabolism: Medical Benchmarking ReportDocument9 pagesCalcium-Phosphate Metabolism: Medical Benchmarking ReportLuis Hernan Guerrero LoaizaNo ratings yet
- MMC Case StudyDocument23 pagesMMC Case Studyapi-547007896No ratings yet
- NUT 116AL Obesity Case StudyDocument10 pagesNUT 116AL Obesity Case StudyAkarin MittongtareNo ratings yet
- Case Report: Anesthetic Management of Acute Fatty Liver of Pregnancy in The Postpartum PeriodDocument6 pagesCase Report: Anesthetic Management of Acute Fatty Liver of Pregnancy in The Postpartum PeriodBrando PanjaitanNo ratings yet
- Aspiration PneumoniaDocument46 pagesAspiration Pneumoniayasmine abdelkarimNo ratings yet
- Chemistry (Cobas) - Cornell University College of Veterinary MedicineDocument3 pagesChemistry (Cobas) - Cornell University College of Veterinary MedicineVu NguyenNo ratings yet
- Disjag Baru CKDDocument17 pagesDisjag Baru CKDNorma Juwita MNo ratings yet
- CC Case-Analysis-CompilationDocument5 pagesCC Case-Analysis-CompilationJiyahnBayNo ratings yet
- Pathophysiology and Treatm - Ent of Metabolic Acidosis in The Diarrhoeic CalfDocument5 pagesPathophysiology and Treatm - Ent of Metabolic Acidosis in The Diarrhoeic CalfesyeehoNo ratings yet
- 555-Article Text-4693-2-10-20201212Document7 pages555-Article Text-4693-2-10-20201212bboyhelyNo ratings yet
- Disseminated Intravascular Coagulation 2016Document11 pagesDisseminated Intravascular Coagulation 2016Cris TobalNo ratings yet
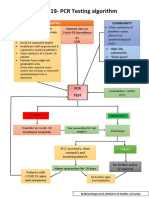
- CovidpcrtestingalgorithmDocument1 pageCovidpcrtestingalgorithmMWNo ratings yet
- Color Atlas of BrainDocument8 pagesColor Atlas of BrainMWNo ratings yet
- Effects of Contamination of Blood Specimens With Liquid potassium-EDTA AnticoagulantDocument8 pagesEffects of Contamination of Blood Specimens With Liquid potassium-EDTA AnticoagulantMWNo ratings yet
- Case ReportDocument3 pagesCase ReportMWNo ratings yet
- Clinical Neuroanatomical TechniquesDocument6 pagesClinical Neuroanatomical TechniquesMWNo ratings yet
- Short ReportDocument4 pagesShort ReportMWNo ratings yet
- Original Article: Macroenzyme Detection by Polyethylene Glycol PrecipitationDocument7 pagesOriginal Article: Macroenzyme Detection by Polyethylene Glycol PrecipitationMWNo ratings yet
- National Guidelines For Analysis of Cerebrospinal Uid For Bilirubin in Suspected Subarachnoid HaemorrhageDocument8 pagesNational Guidelines For Analysis of Cerebrospinal Uid For Bilirubin in Suspected Subarachnoid HaemorrhageMWNo ratings yet
- Validation Vs VerificationDocument46 pagesValidation Vs VerificationMW100% (1)
- AACB 2013 Lab QCDocument9 pagesAACB 2013 Lab QCMW100% (1)
- WHO Practical GuideDocument113 pagesWHO Practical GuideMWNo ratings yet
- Clinical UncertaintyDocument24 pagesClinical Uncertaintyzilangamba_s4535No ratings yet
- Reference Intervals - Direct Priori MethodDocument5 pagesReference Intervals - Direct Priori MethodMWNo ratings yet
- 14 - Interferences in Immunoassay PDFDocument16 pages14 - Interferences in Immunoassay PDFLyannYisellNo ratings yet
- Retirement Planning Mistakes Undermining The Post Retirement Adjustment and Well BeingDocument17 pagesRetirement Planning Mistakes Undermining The Post Retirement Adjustment and Well BeingMehedi HasanNo ratings yet
- Report of Mr. AUDARYA MANEDocument1 pageReport of Mr. AUDARYA MANENeutral GodNo ratings yet
- Septico Tank TreatmentDocument3 pagesSeptico Tank TreatmentfernandaNo ratings yet
- Phychology Cbcs Draft Syllabus PDFDocument50 pagesPhychology Cbcs Draft Syllabus PDFTithi PaulNo ratings yet
- AdfgDocument9 pagesAdfgicha shafiraNo ratings yet
- GMP and Preparation in Hospital Pharmacies - Bouwman and Andersen 19 (5) - 469 - European Journal of Hospital Pharmacy - Science and PracticeDocument4 pagesGMP and Preparation in Hospital Pharmacies - Bouwman and Andersen 19 (5) - 469 - European Journal of Hospital Pharmacy - Science and Practicecarbou0% (1)
- Cast CareDocument4 pagesCast CareRogelyn PatriarcaNo ratings yet
- HIV Infection / AIDS (Z21, B20-B24)Document37 pagesHIV Infection / AIDS (Z21, B20-B24)Shreya ThackerNo ratings yet
- PodStick ManualDocument40 pagesPodStick ManualMusafir QolbuNo ratings yet
- Hospital Designing and PlanningDocument55 pagesHospital Designing and PlanningSiddharthh Nutan Gokani81% (27)
- Approved Harmonized National RD Agenda 2017-2022 PDFDocument90 pagesApproved Harmonized National RD Agenda 2017-2022 PDFJoemel Bautista100% (1)
- Track and Field Constitution 2021-2022 1Document7 pagesTrack and Field Constitution 2021-2022 1api-610935042No ratings yet
- Counselling and PsychoterapyDocument52 pagesCounselling and PsychoterapyelnicaNo ratings yet
- The Awakening From ChildhoodDocument3 pagesThe Awakening From ChildhoodDafer M. EnrijoNo ratings yet
- Business Plan For Juan A Drink PDFDocument17 pagesBusiness Plan For Juan A Drink PDFMaria Jane MoyanoNo ratings yet
- IV ScriptDocument3 pagesIV ScriptRica AcuninNo ratings yet
- AFIU Post Op Managment of Renal Transplant - Prof Saeed AkhtarDocument55 pagesAFIU Post Op Managment of Renal Transplant - Prof Saeed AkhtarUmar FarooqNo ratings yet
- Telemetry Recognition WorkbookDocument29 pagesTelemetry Recognition WorkbookQueenNo ratings yet
- Banking - Diksha Book On Effective Study Techniques PDFDocument66 pagesBanking - Diksha Book On Effective Study Techniques PDFHemrajSainiNo ratings yet
- DSEQ Manual 0 PDFDocument29 pagesDSEQ Manual 0 PDFRiki KikiNo ratings yet
- Symptomatic Treatment of Cough Among Adult Patients With Lung Cancer CHEST Guideline and Expert Panel ReportDocument14 pagesSymptomatic Treatment of Cough Among Adult Patients With Lung Cancer CHEST Guideline and Expert Panel ReportThaísa NogueiraNo ratings yet
- Practical Exercise 3 Pareto Diagram: DR Yousef Amer - School of Engineering University of South Australia Page 1 of 3Document6 pagesPractical Exercise 3 Pareto Diagram: DR Yousef Amer - School of Engineering University of South Australia Page 1 of 3HarisNo ratings yet
- MHPSSDocument11 pagesMHPSSVan TotNo ratings yet
- Jamaica Society For The Blind (JSB)Document4 pagesJamaica Society For The Blind (JSB)eyecarecaribbeanNo ratings yet
- Analgesic Efficacy of Ketoprofen in Postpartum, General Surgery, and Chronic Cancer PainDocument8 pagesAnalgesic Efficacy of Ketoprofen in Postpartum, General Surgery, and Chronic Cancer PainYohanna Lawanda da CostaNo ratings yet
- Textbook of Paediatric Emergency Medicine, 2ndDocument628 pagesTextbook of Paediatric Emergency Medicine, 2ndPhruek Hinhumpetch100% (1)
- In Memoriam David R. Hawkins 27.4Document2 pagesIn Memoriam David R. Hawkins 27.4Aditya VarunNo ratings yet
- Ngoa, Jose Troy - Sas3Document7 pagesNgoa, Jose Troy - Sas3Ella AroNo ratings yet
- Sample Letters To EditorDocument10 pagesSample Letters To EditorPriyanshi KarNo ratings yet
- Graduate Student Research Proposal ExampleDocument3 pagesGraduate Student Research Proposal ExampleHeatherNo ratings yet
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- The Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyFrom EverandThe Body Book: The Law of Hunger, the Science of Strength, and Other Ways to Love Your Amazing BodyNo ratings yet
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)From EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Rating: 4 out of 5 stars4/5 (378)
- The Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingFrom EverandThe Food Lover's Cleanse: 140 Delicious, Nourishing Recipes That Will Tempt You Back into Healthful EatingRating: 4 out of 5 stars4/5 (3)
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- Intermittent Fasting Basics for Women: The Complete Guide to Safe and Effective Weight Loss with Intermittent FastingFrom EverandIntermittent Fasting Basics for Women: The Complete Guide to Safe and Effective Weight Loss with Intermittent FastingRating: 5 out of 5 stars5/5 (12)
- Sugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthFrom EverandSugar Crush: How to Reduce Inflammation, Reverse Nerve Damage, and Reclaim Good HealthRating: 4 out of 5 stars4/5 (6)
- The Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonFrom EverandThe Beck Diet Solution Weight Loss Workbook: The 6-Week Plan to Train Your Brain to Think Like a Thin PersonRating: 3.5 out of 5 stars3.5/5 (33)
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 4.5 out of 5 stars4.5/5 (2)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- The Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodFrom EverandThe Diet Trap Solution: Train Your Brain to Lose Weight and Keep It Off for GoodNo ratings yet
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- Secrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainFrom EverandSecrets From the Eating Lab: The Science of Weight Loss, the Myth of Willpower, and Why You Should Never Diet AgainRating: 3.5 out of 5 stars3.5/5 (38)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- Find Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeFrom EverandFind Your Path: Honor Your Body, Fuel Your Soul, and Get Strong with the Fit52 LifeRating: 4 out of 5 stars4/5 (3)
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 3.5 out of 5 stars3.5/5 (2)
- How Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseFrom EverandHow Not to Die by Michael Greger MD, Gene Stone - Book Summary: Discover the Foods Scientifically Proven to Prevent and Reverse DiseaseRating: 4.5 out of 5 stars4.5/5 (83)
- The End of Craving: Recovering the Lost Wisdom of Eating WellFrom EverandThe End of Craving: Recovering the Lost Wisdom of Eating WellRating: 4.5 out of 5 stars4.5/5 (80)
- Rapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsFrom EverandRapid Weight Loss Hypnosis: Deep Sleep Your Way to Rapid Weight Loss, Healing Your Body and Self Esteem with Guided Meditations and Positive AffirmationsRating: 5 out of 5 stars5/5 (7)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainFrom EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainRating: 3.5 out of 5 stars3.5/5 (6)
- Proteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItFrom EverandProteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItRating: 4.5 out of 5 stars4.5/5 (19)
- Foods That Cause You to Lose Weight: The Negative Calorie EffectFrom EverandFoods That Cause You to Lose Weight: The Negative Calorie EffectRating: 3 out of 5 stars3/5 (5)