You might also like
- Gizmo (Meiosis)Document8 pagesGizmo (Meiosis)Elijah50% (6)
- Clin Chem CompiledDocument9 pagesClin Chem CompiledReg LagartejaNo ratings yet
- AACB 2013 Lab QCDocument9 pagesAACB 2013 Lab QCMW100% (1)
- Serum Protein Electrophoresis: Edited by RaniDocument66 pagesSerum Protein Electrophoresis: Edited by RaniMustakim DuharingNo ratings yet
- Newsletter10-1 SebiaDocument4 pagesNewsletter10-1 SebiaNidiam2100% (1)
- Virtual Laboratory Exercise 2Document4 pagesVirtual Laboratory Exercise 2Jung Somin100% (1)
- Validation Vs VerificationDocument46 pagesValidation Vs VerificationMW100% (1)
- Toksik 1Document5 pagesToksik 1wiwin nur halizaNo ratings yet
- Effects of Anticoagulants in BiochemistryDocument4 pagesEffects of Anticoagulants in BiochemistrySaniya KulkarniNo ratings yet
- MLT Boards - Chemistry (BOR)Document22 pagesMLT Boards - Chemistry (BOR)sherwinbuluranNo ratings yet
- Quantification of Pregabalin Using Hydrophilic Interaction HPLC-High-Resolution MS in Postmortem Human Samples: Eighteen Case ReportsDocument6 pagesQuantification of Pregabalin Using Hydrophilic Interaction HPLC-High-Resolution MS in Postmortem Human Samples: Eighteen Case ReportsLuisa Fernanda Velásquez QuijanoNo ratings yet
- Clinchem 1479Document4 pagesClinchem 1479ghfkhgfjhfgNo ratings yet
- My JournalDocument12 pagesMy JournalFelixNo ratings yet
- Effects of Total Plasma Protein ConcentrDocument4 pagesEffects of Total Plasma Protein ConcentrThuy NguyenNo ratings yet
- 2011 Schumann Alp-Reference-Method CCLMDocument8 pages2011 Schumann Alp-Reference-Method CCLMأم الجودNo ratings yet
- Zapadka, Et Al (2016) A PH Induced Switch in GLP 1 Aggregation KineticsDocument9 pagesZapadka, Et Al (2016) A PH Induced Switch in GLP 1 Aggregation Kineticstantry puspitasariNo ratings yet
- An Unique Encounter With ParaprotenemiaDocument3 pagesAn Unique Encounter With ParaprotenemiaramazankocabasNo ratings yet
- Practical Laboratory Medicine: Gilles Cauet, Aurélien Daynès, Nevzat TemurokDocument7 pagesPractical Laboratory Medicine: Gilles Cauet, Aurélien Daynès, Nevzat TemurokFrankenstein MelancholyNo ratings yet
- Jcem 2743Document4 pagesJcem 2743Yaser MNo ratings yet
- Haemoglobin Electrophoresis in Diagnosing A Case oDocument3 pagesHaemoglobin Electrophoresis in Diagnosing A Case oTawsif MusharofNo ratings yet
- Haemoglobin Electrophoresis in Diagnosing A Case oDocument3 pagesHaemoglobin Electrophoresis in Diagnosing A Case oYunonNo ratings yet
- A524 780TM1Document2 pagesA524 780TM1clinical_pathologyNo ratings yet
- Interferencia Indices SericosDocument8 pagesInterferencia Indices SericosALEJANDRO OLIVARES MARTÍNEZNo ratings yet
- Paraproteins A Review Article and MCQ'sDocument10 pagesParaproteins A Review Article and MCQ'slataseyaniNo ratings yet
- Shaker IDocument4 pagesShaker IyessiesektiNo ratings yet
- Clinical Characterization of Patients WithDocument4 pagesClinical Characterization of Patients WithPaulo Eduardo CampanaNo ratings yet
- A Modified Protein Precipitation Procedure For Efficient Removal of Albumin From SerumDocument11 pagesA Modified Protein Precipitation Procedure For Efficient Removal of Albumin From SerumDámaso A. Rubio VargasNo ratings yet
- Design of A Coupled Bioluminescent Assay For A Recombinant Pyruvate Kinase From A Thermophilic GeobacillusDocument8 pagesDesign of A Coupled Bioluminescent Assay For A Recombinant Pyruvate Kinase From A Thermophilic Geobacillusd2champNo ratings yet
- Evaluation of Effect of Some Corticosteroids On Glucose-6-Phosphate Dehydrogenase and Comparative Study of Antioxidant Enzyme ActivitiesDocument6 pagesEvaluation of Effect of Some Corticosteroids On Glucose-6-Phosphate Dehydrogenase and Comparative Study of Antioxidant Enzyme ActivitiesBrianna PowersNo ratings yet
- Monitoring of ATP Levels in Red Blood Cells and T Cells of Healthy and Ill Subjects and The Effects of Age On Mitochondrial PotentialDocument9 pagesMonitoring of ATP Levels in Red Blood Cells and T Cells of Healthy and Ill Subjects and The Effects of Age On Mitochondrial PotentialHossam ArafaNo ratings yet
- Angiolupus 2Document7 pagesAngiolupus 2AlisNo ratings yet
- Identification of Five Gelatins by UPLC Q-ToF-MS Using Principal Component AnalysisDocument5 pagesIdentification of Five Gelatins by UPLC Q-ToF-MS Using Principal Component AnalysisHasna RomadhoniNo ratings yet
- Bagus GlomerulosclerosisDocument10 pagesBagus GlomerulosclerosisJundiNo ratings yet
- A Laboratory Diagnostic Approach To Hepatobiliary Disease in Small AnimalsDocument17 pagesA Laboratory Diagnostic Approach To Hepatobiliary Disease in Small Animalsl.fernandagonzalez97No ratings yet
- Capillary Electrophoresis Method Change - 08 - 08Document2 pagesCapillary Electrophoresis Method Change - 08 - 08Samar SharafNo ratings yet
- Amperometric Biosensor System For Simultaneous Determination ofDocument9 pagesAmperometric Biosensor System For Simultaneous Determination ofOsValdo GarciaNo ratings yet
- Assay Interference A Need For Increased Understanding and TestingDocument9 pagesAssay Interference A Need For Increased Understanding and Testingchali90No ratings yet
- PSK062 01 01Document6 pagesPSK062 01 01q52rqhqsybNo ratings yet
- Inhibition of Rat PC12 Cell Calpain Activity by Glutathione, Oxidized Glutathione and Nitric OxideDocument4 pagesInhibition of Rat PC12 Cell Calpain Activity by Glutathione, Oxidized Glutathione and Nitric OxidePaoloNo ratings yet
- Assays of Matrix Metalloproteinases (MMPS) Activities: A ReviewDocument9 pagesAssays of Matrix Metalloproteinases (MMPS) Activities: A ReviewPaulo MattosNo ratings yet
- Detection of Human Urinary 5 Hydroxymethylcytosine by Stable Isotope Dilution HPLC-MS/MS AnalysisDocument7 pagesDetection of Human Urinary 5 Hydroxymethylcytosine by Stable Isotope Dilution HPLC-MS/MS Analysis承成蔡No ratings yet
- Lacture 5Document116 pagesLacture 5Ahmed Makky JafarNo ratings yet
- The Plasma Sugar, Free Fatty Acid, Cortisol, and Growth Hormone Response Insulin. I. in Control SubjectsDocument8 pagesThe Plasma Sugar, Free Fatty Acid, Cortisol, and Growth Hormone Response Insulin. I. in Control SubjectsYng TangNo ratings yet
- AMPK Phosphorylation Assay KitDocument3 pagesAMPK Phosphorylation Assay KitBioAssay 2015No ratings yet
- UprgenyDocument9 pagesUprgenyJose Rafael Villafan BernalNo ratings yet
- 223821lateral Circulate Immunoassays For Aflatoxins B and G and For Aflatoxin M1Document3 pages223821lateral Circulate Immunoassays For Aflatoxins B and G and For Aflatoxin M1ephardfdvkNo ratings yet
- Macroprolactinemia Associated With Anti-Prolactin Antibodies: A Case ReportDocument3 pagesMacroprolactinemia Associated With Anti-Prolactin Antibodies: A Case ReportYaser MNo ratings yet
- Natural History and Early Diagnosis of LAD-1 - Variant SyndromeDocument9 pagesNatural History and Early Diagnosis of LAD-1 - Variant SyndromeCosmin BarbosNo ratings yet
- J. Biol. Chem.-1994-Jaffe-13065-8Document4 pagesJ. Biol. Chem.-1994-Jaffe-13065-8Toeii ChatpolchaiNo ratings yet
- Instrumentation, Quantitative Meausrement of Platelet Makers and Quality ControlDocument63 pagesInstrumentation, Quantitative Meausrement of Platelet Makers and Quality ControlVince Louie VictoriosoNo ratings yet
- GliclazideDocument8 pagesGliclazideUpe VeerlapatiNo ratings yet
- Serum Protein Electrophoresis and ImmunofixationDocument112 pagesSerum Protein Electrophoresis and ImmunofixationMand Bady100% (1)
- Sds Methode LimitationsDocument8 pagesSds Methode LimitationsorinadeesfuerzoNo ratings yet
- 08 Rivers JPRDocument7 pages08 Rivers JPRVenkata Suryanarayana GorleNo ratings yet
- Engineering Journal::Methanolic Extract of Red Ginseng Marc Induces Apoptosis On Human Oral Squamous Cell Carcinoma HSC-3Document12 pagesEngineering Journal::Methanolic Extract of Red Ginseng Marc Induces Apoptosis On Human Oral Squamous Cell Carcinoma HSC-3Engineering JournalNo ratings yet
- Low Serum Bicarbonate in A Patient With Diabetes&#Document3 pagesLow Serum Bicarbonate in A Patient With Diabetes&#ayaz ahmadNo ratings yet
- Protein Precipitation As A Possible Important Pitfall in The Clinical Chemistry Analysis of Blood Samples Containing Monoclonal ImmunoglobulinsDocument11 pagesProtein Precipitation As A Possible Important Pitfall in The Clinical Chemistry Analysis of Blood Samples Containing Monoclonal ImmunoglobulinsramazankocabasNo ratings yet
- Arn de InterferenciaDocument8 pagesArn de InterferenciaRosita Aguirre FloresNo ratings yet
- Effects of Oxcarbazepine Use On Hemogram Liver ThyDocument6 pagesEffects of Oxcarbazepine Use On Hemogram Liver ThyehsanNo ratings yet
- Alpha-AMYLASE BLOSR6x82 ENDocument4 pagesAlpha-AMYLASE BLOSR6x82 ENMeethuanNo ratings yet
- Uapcr DiagnosticDocument8 pagesUapcr DiagnosticYA MAAPNo ratings yet
- 10 Amylase, Lipase, Gamma Glutamyl Transferase, Glucose-6-Phosphate Dehydrogenase, Cholinesterase and 5-NucleotidaseDocument29 pages10 Amylase, Lipase, Gamma Glutamyl Transferase, Glucose-6-Phosphate Dehydrogenase, Cholinesterase and 5-NucleotidaseFrances FranciscoNo ratings yet
- Thrombocytopathia and Light-Chain Proteinuria in A Dog Naturally Infected WithDocument3 pagesThrombocytopathia and Light-Chain Proteinuria in A Dog Naturally Infected WithDiana GranadaNo ratings yet
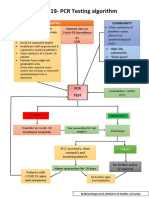
- CovidpcrtestingalgorithmDocument1 pageCovidpcrtestingalgorithmMWNo ratings yet
- Clinical Neuroanatomical TechniquesDocument6 pagesClinical Neuroanatomical TechniquesMWNo ratings yet
- Case ReportDocument3 pagesCase ReportMWNo ratings yet
- Case Report: Excessive Calcium Ingestion Leading To Milk-Alkali SyndromeDocument3 pagesCase Report: Excessive Calcium Ingestion Leading To Milk-Alkali SyndromeMWNo ratings yet
- Color Atlas of BrainDocument8 pagesColor Atlas of BrainMWNo ratings yet
- Short ReportDocument4 pagesShort ReportMWNo ratings yet
- National Guidelines For Analysis of Cerebrospinal Uid For Bilirubin in Suspected Subarachnoid HaemorrhageDocument8 pagesNational Guidelines For Analysis of Cerebrospinal Uid For Bilirubin in Suspected Subarachnoid HaemorrhageMWNo ratings yet
- WHO Practical GuideDocument113 pagesWHO Practical GuideMWNo ratings yet
- Reference Intervals - Direct Priori MethodDocument5 pagesReference Intervals - Direct Priori MethodMWNo ratings yet
- Prodcut of Recombinat DNA TechnologyDocument9 pagesProdcut of Recombinat DNA TechnologySHOAIB NAVEEDNo ratings yet
- NegOr Q4 GenBio2 SLKWeek5 v2Document14 pagesNegOr Q4 GenBio2 SLKWeek5 v2Maribel Ruedas RamosNo ratings yet
- Actual ItemsDocument7 pagesActual ItemsJessica OcheaNo ratings yet
- MCB 309 SyllabusDocument3 pagesMCB 309 SyllabusChaos HadesNo ratings yet
- Terms and Concepts in Plant PathologyDocument48 pagesTerms and Concepts in Plant PathologytripsNo ratings yet
- Sains Dalam Air Liur ManusiaDocument11 pagesSains Dalam Air Liur ManusiaacehhfzhNo ratings yet
- MCQ Biotechnology CRT QuestionsDocument20 pagesMCQ Biotechnology CRT QuestionsEkta MenghaniNo ratings yet
- Chapter 10 Guided ReadingDocument11 pagesChapter 10 Guided ReadingNadim HammoudNo ratings yet
- Aict General Knowledge 2 025a8954bced8Document4 pagesAict General Knowledge 2 025a8954bced8Ujjwal SinghalNo ratings yet
- January 2021 P2BR QPDocument24 pagesJanuary 2021 P2BR QPSareeha SadhviNo ratings yet
- 2016 FY11 Biology Detailed SolutionDocument31 pages2016 FY11 Biology Detailed SolutionPeter MayNo ratings yet
- 2017 H2 Biology Prelim SA2 Raffles InstitutionDocument77 pages2017 H2 Biology Prelim SA2 Raffles InstitutionSalman ShethNo ratings yet
- Shimshekgenesisi CRE2002Document9 pagesShimshekgenesisi CRE2002MihailNo ratings yet
- Biof325 Exam 1answersDocument7 pagesBiof325 Exam 1answersSmartunblurrNo ratings yet
- 1-CV Payeli 2023Document3 pages1-CV Payeli 2023shobhitbhargava39No ratings yet
- Small Mobilizable Multi-Purpose Cloning Vectors Derived From The The Chromosome of Corynebacterium GlutumicumDocument5 pagesSmall Mobilizable Multi-Purpose Cloning Vectors Derived From The The Chromosome of Corynebacterium GlutumicumMariaNo ratings yet
- MuscleDocument5 pagesMuscleAbdulrahman AqraNo ratings yet
- Molecular Biology of The Cell, Sixth Edition Chapter 5: Dna Replication, Repair, and RecombinationDocument25 pagesMolecular Biology of The Cell, Sixth Edition Chapter 5: Dna Replication, Repair, and RecombinationIsmael Torres-PizarroNo ratings yet
- Biochemical Energy ProductionDocument59 pagesBiochemical Energy ProductionShane G.No ratings yet
- Classification Study Guide AnswersDocument2 pagesClassification Study Guide Answersapi-325864985100% (1)
- Polymerase Chain Reaction (PCR), Immunoassay Dan Respon Imunitas Penderita Sars Ncov-2, Sebuah Narasi Review (Studi Literatur)Document8 pagesPolymerase Chain Reaction (PCR), Immunoassay Dan Respon Imunitas Penderita Sars Ncov-2, Sebuah Narasi Review (Studi Literatur)Medical EngineerNo ratings yet
- Biomolecules New BioHackDocument9 pagesBiomolecules New BioHackAdhithyan MNo ratings yet
- Claribel Ria MaeDocument19 pagesClaribel Ria MaeGLENN MENDOZANo ratings yet
- Sex DeterminationDocument14 pagesSex DeterminationAdri ChakraNo ratings yet
- The CellDocument8 pagesThe CellCasielle KyroffNo ratings yet
- 141 Research Studies Affirm Naturally Acquired Immunity To Covid-19 (Brownstone Institute 2021)Document40 pages141 Research Studies Affirm Naturally Acquired Immunity To Covid-19 (Brownstone Institute 2021)gd_hbarNo ratings yet
- Anthropology Final HadoutDocument65 pagesAnthropology Final HadoutDagim AbrehamNo ratings yet
- Path-SARS-CoV-2 Winterplex IFU Issue 11.02Document36 pagesPath-SARS-CoV-2 Winterplex IFU Issue 11.02nazmiNo ratings yet