You might also like
- Metrobank Home Loan Application FormDocument2 pagesMetrobank Home Loan Application Formrauden40% (5)
- CV Format For PRC ActivityDocument2 pagesCV Format For PRC ActivityFitz Jaminit100% (1)
- KIA India Dealer Application FormDocument14 pagesKIA India Dealer Application Formpalanisamy86% (22)
- Resume of Resource Person: Professional Regulation CommissionDocument3 pagesResume of Resource Person: Professional Regulation CommissionMa. Jennyrose Solis100% (1)
- Policy Amendment Form FILLABLEDocument2 pagesPolicy Amendment Form FILLABLEcristina tamonteNo ratings yet
- Kia India Dealership Application FormDocument9 pagesKia India Dealership Application FormfalconsnordNo ratings yet
- Denr EmbDocument2 pagesDenr EmbELben RescoberNo ratings yet
- 2015 September 16 Group Application Form (Sept 2015)Document1 page2015 September 16 Group Application Form (Sept 2015)Evangeline AcunaNo ratings yet
- E-Commerce Partnership Registration Form: Company InformationDocument1 pageE-Commerce Partnership Registration Form: Company InformationA.N.M. neyaz MorshedNo ratings yet
- UCPB Client Information Update Sheet CIUSDocument2 pagesUCPB Client Information Update Sheet CIUSLeogen TomultoNo ratings yet
- Kia India Dealer Application FormDocument13 pagesKia India Dealer Application FormAlok KumarNo ratings yet
- Employment Application Form: (Information Contained in This Application Will Be Treated As Confidential)Document4 pagesEmployment Application Form: (Information Contained in This Application Will Be Treated As Confidential)Rehan khan NCSNo ratings yet
- Standard Application Form 6 Pager FATCA Change 31052016Document6 pagesStandard Application Form 6 Pager FATCA Change 31052016आज़ाद पटेलNo ratings yet
- Optima Secure PDFDocument13 pagesOptima Secure PDFandro4shivNo ratings yet
- Bdo 1ST Dep Form For Cy 2021Document1 pageBdo 1ST Dep Form For Cy 2021Arriane Jane Espora MataganasNo ratings yet
- Recruiter Name: Infinite Dragon Life Insurance AgencyDocument17 pagesRecruiter Name: Infinite Dragon Life Insurance Agencybob huli ngalanNo ratings yet
- The Rawalpindi Chamber of Commerce & IndustryDocument4 pagesThe Rawalpindi Chamber of Commerce & IndustryNasir BashirNo ratings yet
- Consolidated Enrollment Form - SFI (FINAL-2018)Document2 pagesConsolidated Enrollment Form - SFI (FINAL-2018)Anh TranNo ratings yet
- Onboarding FormDocument3 pagesOnboarding FormVishnu VardhanNo ratings yet
- Ulip Proposal PDFDocument8 pagesUlip Proposal PDFrajkumarNo ratings yet
- Appendix C Resume of Resource Persons 1Document2 pagesAppendix C Resume of Resource Persons 1Divine O. OcumenNo ratings yet
- Renewal of Your Easy Health Floater Standard Insurance PolicyDocument4 pagesRenewal of Your Easy Health Floater Standard Insurance PolicyAhesan Ali MominNo ratings yet
- Prestige Clairemont Kokapet 1Document4 pagesPrestige Clairemont Kokapet 1luke_skywarediffmailNo ratings yet
- Loan FormDocument3 pagesLoan FormJustine Mae CipresNo ratings yet
- Accreditation Form & PisDocument3 pagesAccreditation Form & Pisamiel pugatNo ratings yet
- Claims Statement 2018Document17 pagesClaims Statement 2018sNo ratings yet
- Fellowship Mutual Recognition App Form 2022Document4 pagesFellowship Mutual Recognition App Form 2022siddhesh karnikNo ratings yet
- SEIS Form For Test EnvironmentDocument3 pagesSEIS Form For Test EnvironmentPrincess SalvadorNo ratings yet
- Cash Card Updating Form Legal Fillable 5 PagesDocument5 pagesCash Card Updating Form Legal Fillable 5 PagesAidonNo ratings yet
- Candidate Application FormDocument2 pagesCandidate Application FormMårk MèrçådøNo ratings yet
- Family Discount Program Enrollment FormDocument1 pageFamily Discount Program Enrollment FormJeffrey LiNo ratings yet
- Brokers Manager & Agent Accreditation FormsDocument2 pagesBrokers Manager & Agent Accreditation FormsJ SalesNo ratings yet
- Membership Application: "Bridging The Gap Between Concrete Knowledge & Practice"Document1 pageMembership Application: "Bridging The Gap Between Concrete Knowledge & Practice"MarkNo ratings yet
- Prrivate Car Proposal Form July 2015Document2 pagesPrrivate Car Proposal Form July 2015Md RashidNo ratings yet
- Salary Certificate Request FormDocument1 pageSalary Certificate Request FormAhmad Abou HadiNo ratings yet
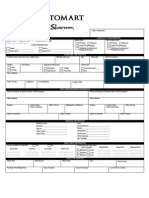
- Application FormDocument1 pageApplication FormpinoyautomartNo ratings yet
- RP Questionnaire - Individual BorrowerDocument2 pagesRP Questionnaire - Individual BorrowerTin-tin Reyes Jr.No ratings yet
- Application Form For Minor Policy Alterations: (Contact Details To Be Filled Mandatory)Document2 pagesApplication Form For Minor Policy Alterations: (Contact Details To Be Filled Mandatory)Sonu SinghNo ratings yet
- Minor Alteration Form - Client PDFDocument2 pagesMinor Alteration Form - Client PDFSonu SinghNo ratings yet
- KIA India Dealer Application FormDocument8 pagesKIA India Dealer Application FormAMIT BAFNANo ratings yet
- APP - MET - Enhanced Medical Benefit Plan-3 (NEXtCARE) - July 2021Document8 pagesAPP - MET - Enhanced Medical Benefit Plan-3 (NEXtCARE) - July 2021FebilaNo ratings yet
- Application - Engineer, Project (75297) - Vishnuvarthan SDocument3 pagesApplication - Engineer, Project (75297) - Vishnuvarthan Svishnu RasaaliNo ratings yet
- Barrick Enrollment Form Apr 2022Document3 pagesBarrick Enrollment Form Apr 2022jorge ordinolaNo ratings yet
- NEAP Curriculum-VitaeDocument2 pagesNEAP Curriculum-VitaeJean EspinosaNo ratings yet
- Account Opening Form: Maldives Islamic BankDocument2 pagesAccount Opening Form: Maldives Islamic BankmikeNo ratings yet
- Employment Application Form: Human Resource DepartmentDocument3 pagesEmployment Application Form: Human Resource DepartmentMudassar PatelNo ratings yet
- KIA India Dealer Application FormDocument13 pagesKIA India Dealer Application FormSalim MiyaNo ratings yet
- Insurance Policy Receipt TemplateDocument1 pageInsurance Policy Receipt TemplateRahul JiwaneNo ratings yet
- Life Insurance Policy Surrender Request Form FIllableDocument1 pageLife Insurance Policy Surrender Request Form FIllableDanny Glean LabordoNo ratings yet
- FDC Demat Tender FormDocument2 pagesFDC Demat Tender FormManoranjan AnmolNo ratings yet
- NEW LOAN-APPLICATION-FORM November 2021 v2 PDFDocument4 pagesNEW LOAN-APPLICATION-FORM November 2021 v2 PDFjohnson mwauraNo ratings yet
- HR-REC-02 Application Form Rev - 2Document2 pagesHR-REC-02 Application Form Rev - 2Gaming PalonNo ratings yet
- Dok Alternatibo Brotherhood With Inventors Guild CooperativeDocument2 pagesDok Alternatibo Brotherhood With Inventors Guild CooperativeStaff Coo Dok AlternatiboNo ratings yet
- Policy Name Policy No. Date of Expiry: My:health Koti Suraksha Section 2 Personal Accident - Schedule of CoverageDocument2 pagesPolicy Name Policy No. Date of Expiry: My:health Koti Suraksha Section 2 Personal Accident - Schedule of CoverageRaju GbNo ratings yet
- Research Paper InformationDocument4 pagesResearch Paper InformationJerico NaypaNo ratings yet
- MSME Loan Application FinalDocument12 pagesMSME Loan Application Finalnambi2rajanNo ratings yet
- Credit Card Application: For Principal CardholderDocument1 pageCredit Card Application: For Principal CardholderDe Gala ChrisNo ratings yet
- The Seriously Lighthearted Guide to BBBEE Benefits for Small Black Owned Businesses!: The Seriously Lighthearted Guide Series, #3From EverandThe Seriously Lighthearted Guide to BBBEE Benefits for Small Black Owned Businesses!: The Seriously Lighthearted Guide Series, #3No ratings yet
- 5 Rules to Achieve Financial Agility Without Killing Your Dream LifestyleFrom Everand5 Rules to Achieve Financial Agility Without Killing Your Dream LifestyleRating: 5 out of 5 stars5/5 (1)
- Electronic Ticket Receipt 28JUL For FRANCISCO JR AQUINODocument3 pagesElectronic Ticket Receipt 28JUL For FRANCISCO JR AQUINOTribal PrincezsNo ratings yet
- Electronic Ticket Receipt 28JUL For VIRGILIO LUCQUIAODocument3 pagesElectronic Ticket Receipt 28JUL For VIRGILIO LUCQUIAOTribal PrincezsNo ratings yet
- Electronic Ticket Receipt 28JUL For AILEEN LIBANDocument3 pagesElectronic Ticket Receipt 28JUL For AILEEN LIBANTribal PrincezsNo ratings yet
- To Puerto Princesa: Original Flight Details Changed To PassengersDocument1 pageTo Puerto Princesa: Original Flight Details Changed To PassengersTribal PrincezsNo ratings yet
- Singtel Annual Report 2023 Higher ResDocument275 pagesSingtel Annual Report 2023 Higher ResJL ChuaNo ratings yet
- Kuliah 02 - Pengolahan Citra Digital Sampling Quantization 2Document18 pagesKuliah 02 - Pengolahan Citra Digital Sampling Quantization 2Zulkifli Nagh BalitanNo ratings yet
- Module 5 Advanced MechanicsDocument60 pagesModule 5 Advanced Mechanicsiknowvictoriassecret49No ratings yet
- Development LetterDocument3 pagesDevelopment Lettertan balanNo ratings yet
- Energy and Buildings: F. AsdrubaliDocument9 pagesEnergy and Buildings: F. AsdrubaliBogdan BrieNo ratings yet
- Critical Thinking and EBPDocument31 pagesCritical Thinking and EBPEni SukmawatiNo ratings yet
- Methods of Teaching 1 and 6Document68 pagesMethods of Teaching 1 and 6BUEN, RENZZELLE JOY B.No ratings yet
- Process Pump ControlDocument4 pagesProcess Pump ControlBramJanssen76No ratings yet
- GIS and Regional Economic Development Planning: Chen Fei Du Daosheng Jiang JingtongDocument8 pagesGIS and Regional Economic Development Planning: Chen Fei Du Daosheng Jiang JingtongJuragan MudaNo ratings yet
- Ellena's Book of Birds in SingaporeDocument38 pagesEllena's Book of Birds in SingaporeEllena GabrielleNo ratings yet
- Recognia Intraday Trader InfosheetDocument2 pagesRecognia Intraday Trader InfosheetDipesh PawaiyaNo ratings yet
- Quiet Healing CentreDocument12 pagesQuiet Healing CentredoliamahakNo ratings yet
- Kurukh GrammarDocument184 pagesKurukh GrammarBHABANI SHANKAR MINZNo ratings yet
- 0332713Document200 pages0332713JS DUFFEYNo ratings yet
- Tom MCQ UNIT 2Document14 pagesTom MCQ UNIT 2Kumar PachareNo ratings yet
- What's in Your BackpackDocument31 pagesWhat's in Your Backpackjohn ezekiel de asisNo ratings yet
- Digital Systems Design and PrototypingDocument633 pagesDigital Systems Design and PrototypingAshish Shrivastava50% (2)
- OM Best Practices Guidelines V3.0Document98 pagesOM Best Practices Guidelines V3.0Enrique Balan RomeroNo ratings yet
- Oripol Nan Secure BrochureDocument4 pagesOripol Nan Secure Brochuresanjeev.ranjan.npsNo ratings yet
- Autonomy of Art or Dignity of The Artwork? - Agnes HellerDocument20 pagesAutonomy of Art or Dignity of The Artwork? - Agnes HellerProfrFer100% (1)
- Cantor Set FunctionDocument15 pagesCantor Set FunctionRenato GaloisNo ratings yet
- Csec It Mock ExamDocument10 pagesCsec It Mock Examvidur_talreja100% (1)
- Types of Malware and Importance of Malware AnalysisDocument10 pagesTypes of Malware and Importance of Malware AnalysisshaletNo ratings yet
- DWDM Equipment-Alcatel 1620Document28 pagesDWDM Equipment-Alcatel 1620Cvenoth Kumar100% (2)
- Digital Booklet - Britney Spears - Work B CH (Single)Document5 pagesDigital Booklet - Britney Spears - Work B CH (Single)Gâu EheheNo ratings yet
- Dif Conrete Tension (Malvar)Document5 pagesDif Conrete Tension (Malvar)mohamed_gmal22No ratings yet
- Health Assessment of Structures PaperDocument4 pagesHealth Assessment of Structures PaperNirmal ModyNo ratings yet
- RTI Online Submit Request FormDocument1 pageRTI Online Submit Request FormRinky SharmaNo ratings yet
- Hazyl Delerosario@ctu Edu PHDocument4 pagesHazyl Delerosario@ctu Edu PHDulce Amor del RosarioNo ratings yet
- Estimation of Measurement Uncertainty Printout 2016-2Document94 pagesEstimation of Measurement Uncertainty Printout 2016-2GustavoCaicutoNo ratings yet