You might also like
- A Plan for a Single-Payer Health Care System: The Best Health Care in the WorldFrom EverandA Plan for a Single-Payer Health Care System: The Best Health Care in the WorldNo ratings yet
- Health System in TaiwanDocument5 pagesHealth System in TaiwanIraaNo ratings yet
- Health-Fi Nancing Reforms in Southeast AsiaDocument12 pagesHealth-Fi Nancing Reforms in Southeast AsiaKutu KupretNo ratings yet
- Review Jurnal Pembiayaan Kesehatan 2Document5 pagesReview Jurnal Pembiayaan Kesehatan 2SUCI PERMATANo ratings yet
- sdg3 AkucheDocument31 pagessdg3 AkucheJohn-adewaleSmithNo ratings yet
- An Overview of The Healthcare System in Taiwan PDFDocument6 pagesAn Overview of The Healthcare System in Taiwan PDFIraaNo ratings yet
- BMC Health Services ResearchDocument9 pagesBMC Health Services ResearchEirics BrondyNo ratings yet
- Introduction to the Health Care IndustryDocument47 pagesIntroduction to the Health Care IndustryKshitiz KadamNo ratings yet
- Health Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To SubscribeDocument12 pagesHealth Affairs: For Reprints, Links & Permissions: E-Mail Alerts: To SubscribeDedet TriwahyudiNo ratings yet
- Triple Aim HospitalsDocument12 pagesTriple Aim HospitalsaNo ratings yet
- Anusha Verma Kittinan Chayanuwat Win Final DraftDocument7 pagesAnusha Verma Kittinan Chayanuwat Win Final Draftapi-551359428No ratings yet
- The Use of Reproductive Healthcare at Commune Health Stations in A Changing Health System in VietnamDocument9 pagesThe Use of Reproductive Healthcare at Commune Health Stations in A Changing Health System in VietnamjlventiganNo ratings yet
- Chapter One by Hamida AdamDocument4 pagesChapter One by Hamida Adamadamhamida351No ratings yet
- Common Health Issues: RationaleDocument7 pagesCommon Health Issues: RationaleClyde CapadnganNo ratings yet
- Demand in Health Care AnalysisDocument9 pagesDemand in Health Care AnalysisZewdu MinwuyeletNo ratings yet
- Journal Pone 0152866Document20 pagesJournal Pone 0152866yulya lasmitaNo ratings yet
- Pages From IJPHRD February - 2020-3Document5 pagesPages From IJPHRD February - 2020-3Tengiz VerulavaNo ratings yet
- Lva1 App6892Document62 pagesLva1 App6892Pallavi PalluNo ratings yet
- Background and Rationale: Global Forum For Health Research) The World Health Organization Defines Social DeterminantsDocument7 pagesBackground and Rationale: Global Forum For Health Research) The World Health Organization Defines Social DeterminantsAnne KathrineNo ratings yet
- The National Health Insurance Scheme: Perceptions and Experiences of Health Care Providers and Clients in Two Districts of GhanaDocument13 pagesThe National Health Insurance Scheme: Perceptions and Experiences of Health Care Providers and Clients in Two Districts of GhanaevitadewayaniNo ratings yet
- UHC Country Support PDFDocument12 pagesUHC Country Support PDFdiah irfainiNo ratings yet
- Health Systems 2009 20aug ADocument74 pagesHealth Systems 2009 20aug ANational Child Health Resource Centre (NCHRC)No ratings yet
- Trends Affecting NSG PracticeDocument22 pagesTrends Affecting NSG PracticeshaitabliganNo ratings yet
- HLTH 101 PaperDocument8 pagesHLTH 101 Paperapi-548493910No ratings yet
- Yen 2014Document10 pagesYen 2014Sukandriani UtamiNo ratings yet
- Iubjbkb KLDocument21 pagesIubjbkb KLJohn-adewaleSmithNo ratings yet
- International Journal For Equity in HealthDocument10 pagesInternational Journal For Equity in HealthNelmarcioNo ratings yet
- Getting India's Health Care System Out of The ICUDocument2 pagesGetting India's Health Care System Out of The ICUPulokesh GhoshNo ratings yet
- Presentation On Health Care System ModelsDocument37 pagesPresentation On Health Care System ModelsTashi Makpen100% (1)
- Health-Seeking Behaviour and Health Outcome Among Uninsured Patients Attending A Primary Care Clinic of A Teaching Hospital in Southwestern NigeriaDocument7 pagesHealth-Seeking Behaviour and Health Outcome Among Uninsured Patients Attending A Primary Care Clinic of A Teaching Hospital in Southwestern NigeriaInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Healthcare Systems Around the WorldDocument6 pagesHealthcare Systems Around the World3500No ratings yet
- Ameyaw_2021_Is the National Health_Insurance Helping Pregnant Women Access HealthcareDocument9 pagesAmeyaw_2021_Is the National Health_Insurance Helping Pregnant Women Access Healthcarepapaebojackson2004No ratings yet
- 2015 3 3 Information Brief On Health Systems Strengthening v5 Final With MSH LogoDocument10 pages2015 3 3 Information Brief On Health Systems Strengthening v5 Final With MSH LogoNigusu GetachewNo ratings yet
- Equity in Health Care Financing: The Case of MalaysiaDocument15 pagesEquity in Health Care Financing: The Case of MalaysiaViorentina YofianiNo ratings yet
- Advantages and Disadvantages of Free Medical Health Care 1Document3 pagesAdvantages and Disadvantages of Free Medical Health Care 1Gladys vidzoNo ratings yet
- Research Article Willingness To Pay For Social Health Insurance and Associated Factors Among Health Care Providers in Addis Ababa, EthiopiaDocument7 pagesResearch Article Willingness To Pay For Social Health Insurance and Associated Factors Among Health Care Providers in Addis Ababa, EthiopiaaisyahNo ratings yet
- Training needs analysis and module design for hospital staffDocument99 pagesTraining needs analysis and module design for hospital staffpolly1963No ratings yet
- WHR2010 Regional StrategyDocument16 pagesWHR2010 Regional StrategyADB Health Sector GroupNo ratings yet
- Health System in AustraliaDocument7 pagesHealth System in AustraliaNadia Novernia Cristy KatuukNo ratings yet
- Universal Health Coverage of Bangladesh - Analysis Through The Framework of Alford's Theory of Structural Interests in Health Care PPT 28 PresentedDocument30 pagesUniversal Health Coverage of Bangladesh - Analysis Through The Framework of Alford's Theory of Structural Interests in Health Care PPT 28 PresentedRashed ShukornoNo ratings yet
- WCF India Provides Affordable HealthcareDocument24 pagesWCF India Provides Affordable HealthcarekarhtiNo ratings yet
- The Community Health Foundation of ClevelandDocument5 pagesThe Community Health Foundation of ClevelandShaayaan SayedNo ratings yet
- Why Should We Start Giving Importance To Health SectorDocument3 pagesWhy Should We Start Giving Importance To Health SectorShreyas RenukaradhyaNo ratings yet
- Kreng2011 PDFDocument8 pagesKreng2011 PDFDedet TriwahyudiNo ratings yet
- Health Care Financing - 8Document13 pagesHealth Care Financing - 8copy smart50% (2)
- Health Care Guide Provides Overview of Systems and ForecastsDocument203 pagesHealth Care Guide Provides Overview of Systems and ForecastsNiro ThakurNo ratings yet
- Health Systems Strengthening - The University of MelbourneDocument14 pagesHealth Systems Strengthening - The University of MelbourneEstefanía MariñoNo ratings yet
- Hi 225 FinalpaperDocument11 pagesHi 225 Finalpaperapi-708689221No ratings yet
- Medical Tribune September 2012 PHDocument33 pagesMedical Tribune September 2012 PHAsmphLibrary OrtigasNo ratings yet
- AllDocument48 pagesAllnanchieNo ratings yet
- An Evaluation of Health Systems Equity In: Indonesia: Study ProtocolDocument10 pagesAn Evaluation of Health Systems Equity In: Indonesia: Study ProtocolChristhin EsterNo ratings yet
- Total Project ProfileDocument75 pagesTotal Project ProfileVenkata SubbaiahNo ratings yet
- Research Paper 2 - For PopDocument8 pagesResearch Paper 2 - For Popapi-310412032No ratings yet
- Fixing India's Healthcare System - Carnegie Endowment For International PeaceDocument3 pagesFixing India's Healthcare System - Carnegie Endowment For International PeaceMohammad UzairNo ratings yet
- Community Nursing and Care Continuity LEARNING OUTCOMES After CompletingDocument23 pagesCommunity Nursing and Care Continuity LEARNING OUTCOMES After Completingtwy113100% (1)
- Module 7Document36 pagesModule 7Joanne Michelle B. DueroNo ratings yet
- Tackling Out-Of-Pocket Health Care Costs A Discussion Paper: Lesley Russell Jennifer DoggettDocument15 pagesTackling Out-Of-Pocket Health Care Costs A Discussion Paper: Lesley Russell Jennifer DoggettLesley Russell100% (1)
- Health Economic - Case StudyDocument4 pagesHealth Economic - Case StudyMa. Lyn ArandiaNo ratings yet
- HCR Backgrounder Cost 090209Document2 pagesHCR Backgrounder Cost 090209Satriya PranataNo ratings yet
- JLN ProviderPayment MainGuide InteractivePDF 2015Document59 pagesJLN ProviderPayment MainGuide InteractivePDF 2015JulienneNo ratings yet
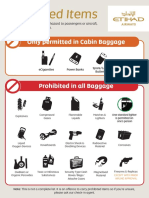
- Prohibited ItemsDocument1 pageProhibited Itemsambet TayloNo ratings yet
- Hussmanns, R. (2004) - Measuring The Informal Economy From Employment in The PDFDocument42 pagesHussmanns, R. (2004) - Measuring The Informal Economy From Employment in The PDFOtrorodrigoNo ratings yet
- Hussmanns, R. (2004) - Measuring The Informal Economy From Employment in The PDFDocument42 pagesHussmanns, R. (2004) - Measuring The Informal Economy From Employment in The PDFOtrorodrigoNo ratings yet
- Valenzuela NewsDocument1 pageValenzuela NewsChelsea Mei De AsisNo ratings yet
- Literature Review of EhrDocument5 pagesLiterature Review of Ehreatlotbnd100% (1)
- Professional Capstone and Practicum Reflective JournalDocument8 pagesProfessional Capstone and Practicum Reflective JournalBonnieNo ratings yet
- CS Form No. 212 Attachment - Work Experience Sheet...Document3 pagesCS Form No. 212 Attachment - Work Experience Sheet...Jm uniteNo ratings yet
- Thesis On Health Care Management PDFDocument5 pagesThesis On Health Care Management PDFlaurajohnsonphoenix100% (2)
- Benefits Enrollment InformationDocument7 pagesBenefits Enrollment Informationjaiden woodNo ratings yet
- Tob (Caesar)Document79 pagesTob (Caesar)doharadwan84No ratings yet
- Navi Health Insurance - Know Your PolicyDocument5 pagesNavi Health Insurance - Know Your PolicyPrajjal ChakrabartyNo ratings yet
- Contact List 10.05.2023Document37 pagesContact List 10.05.2023John Benedict Sta AnaNo ratings yet
- HCC Coding - Jan 2021Document29 pagesHCC Coding - Jan 2021Sonali PawarNo ratings yet
- Add-Walk in InterviewDocument5 pagesAdd-Walk in InterviewshahbazNo ratings yet
- MDR 030508841058Document1 pageMDR 030508841058Jarro Dela TorreNo ratings yet
- Health Insurance in Myanmar The Views and PerceptiDocument14 pagesHealth Insurance in Myanmar The Views and PerceptiHtet Lynn HtunNo ratings yet
- CV - KBGDocument6 pagesCV - KBGKylie GolindangNo ratings yet
- Antibiotic Time-Out ChecklistDocument2 pagesAntibiotic Time-Out ChecklistNawwal Naeem100% (1)
- Nrad Full ReportDocument115 pagesNrad Full ReportSophia RoseNo ratings yet
- Primary Health Care Introduction, Principles and ElentsDocument29 pagesPrimary Health Care Introduction, Principles and ElentsAli emillyNo ratings yet
- rptHosOPGL 2Document1 pagerptHosOPGL 2amir ashraf mokhtarNo ratings yet
- Impact of Multimodal Intervention Strategies On Compliance To Hand Hygiene Practices Among Staff Nurses in Obstetric and Gynaecological WardsDocument1 pageImpact of Multimodal Intervention Strategies On Compliance To Hand Hygiene Practices Among Staff Nurses in Obstetric and Gynaecological WardsALYSSA MARIE MATANo ratings yet
- Rural Hospital Closures Threaten Access ReportDocument10 pagesRural Hospital Closures Threaten Access ReportCourtney RowlesNo ratings yet
- Midwifery Certificate Program - National Midwifery InstituteDocument10 pagesMidwifery Certificate Program - National Midwifery InstituteTheMothershipNo ratings yet
- Reflective Journal CHN in Brgy Capo MSINONDocument2 pagesReflective Journal CHN in Brgy Capo MSINONjan paul galizaNo ratings yet
- List of Clinic Chains in UsDocument90 pagesList of Clinic Chains in Usarpit.mNo ratings yet
- ECardDocument3 pagesECardravitheleoNo ratings yet
- Eligibility Results NoticeDocument12 pagesEligibility Results NoticefullmetalrebelNo ratings yet
- National E-Health Framework by Dr. Enrique TayagDocument18 pagesNational E-Health Framework by Dr. Enrique TayagMark Anthony EllanaNo ratings yet
- The Public Health NurseDocument3 pagesThe Public Health NursedenNo ratings yet
- MR (Medical Representative) - 28Document2 pagesMR (Medical Representative) - 28rakesharain123No ratings yet
- NeonatalpainscalesDocument4 pagesNeonatalpainscalesapi-665163291No ratings yet
- E-Health and Storage Group 1 (NCM 113 THEORY)Document10 pagesE-Health and Storage Group 1 (NCM 113 THEORY)Ralph Elvin MacanlalayNo ratings yet