You might also like
- Topical Reviews in Neurosurgery: Volume 1From EverandTopical Reviews in Neurosurgery: Volume 1J. M. Rice EdwardsNo ratings yet
- Manual for Iv Therapy Procedures & Pain Management: Fourth EditionFrom EverandManual for Iv Therapy Procedures & Pain Management: Fourth EditionNo ratings yet
- Pautas Basadas en La Evidencia para El DesteteDocument23 pagesPautas Basadas en La Evidencia para El DesteteJuan Pa BramantiNo ratings yet
- Protocolos Weaining 2011Document14 pagesProtocolos Weaining 2011perla islasNo ratings yet
- The Efficacy of Medicinal Leeches in Plastic and Reconstructive Surgery - A Systematic Review of 277 Reported Clinical Cases-2Document11 pagesThe Efficacy of Medicinal Leeches in Plastic and Reconstructive Surgery - A Systematic Review of 277 Reported Clinical Cases-2Wara Samsarga GedeNo ratings yet
- Clinical Pathway, LosDocument3 pagesClinical Pathway, LosImuzz Al GhassanNo ratings yet
- Bender2003 PDFDocument6 pagesBender2003 PDFVirgo WNo ratings yet
- Pathogenesis and Treatment of Varicoceles: Controversy Still Surrounds Surgical TreatmentDocument2 pagesPathogenesis and Treatment of Varicoceles: Controversy Still Surrounds Surgical TreatmentFenny LiNo ratings yet
- Use of A Shared Canister Protocol For The Delivery of Metered-Dose Inhalers in Mechanically Ventilated SubjectsDocument8 pagesUse of A Shared Canister Protocol For The Delivery of Metered-Dose Inhalers in Mechanically Ventilated SubjectsevyNo ratings yet
- Chron I SubduralDocument9 pagesChron I Subduralelton fidelisNo ratings yet
- Nut in Clin Prac - 2011 - Simmons - Tubing MisconnectionsDocument8 pagesNut in Clin Prac - 2011 - Simmons - Tubing Misconnectionsmohamed hattaNo ratings yet
- 12Hiệu quả mở kq sớm pt gộp 2015Document10 pages12Hiệu quả mở kq sớm pt gộp 2015Cường Nguyễn HùngNo ratings yet
- Managing The Risks and BenefitDocument8 pagesManaging The Risks and BenefitcacaNo ratings yet
- 2017 Una Guia para Las Directrices Sepsis 2016Document5 pages2017 Una Guia para Las Directrices Sepsis 2016mpacajeNo ratings yet
- Jurnal Suction English PDFDocument4 pagesJurnal Suction English PDFJoko SuprionoNo ratings yet
- 11 Optimizing The Management 1598065529Document12 pages11 Optimizing The Management 1598065529César ArveláezNo ratings yet
- AnestesiDocument9 pagesAnestesiSianipar RomulussNo ratings yet
- Heart & Lung: Care of Critically Ill AdultsDocument13 pagesHeart & Lung: Care of Critically Ill AdultsRabiyatul AwaliyahNo ratings yet
- What Is A Clinical Pathway? Development of A Definition To Inform The DebateDocument4 pagesWhat Is A Clinical Pathway? Development of A Definition To Inform The DebateRSIA MOELIANo ratings yet
- 1 - Outcomes ResearchDocument12 pages1 - Outcomes ResearchMauricio Ruiz MoralesNo ratings yet
- Turning Frequency in Adult Bedridden Patients To Prevent Hospital-Acquired Pressure Ulcer: A Scoping ReviewDocument12 pagesTurning Frequency in Adult Bedridden Patients To Prevent Hospital-Acquired Pressure Ulcer: A Scoping ReviewfajaqaNo ratings yet
- Enhanced Recovery After Surgery JournalDocument9 pagesEnhanced Recovery After Surgery JournalDea DickytaNo ratings yet
- NormalsalineinstillationbeforeendotrachealsuctioningDocument7 pagesNormalsalineinstillationbeforeendotrachealsuctioningEuis Maryah SyahidahNo ratings yet
- Art 3A10.1186 2Fs12879 016 1665 1Document9 pagesArt 3A10.1186 2Fs12879 016 1665 1tmrezatandiNo ratings yet
- Jurnal Tati Social Support .PDF 2Document3 pagesJurnal Tati Social Support .PDF 2Artati ArsyadNo ratings yet
- Practice Guidelines For Central Venous Access PDFDocument35 pagesPractice Guidelines For Central Venous Access PDFJulio AltamiranoNo ratings yet
- Pico PaperDocument7 pagesPico Paperapi-2403520430% (1)
- 03 Na CB GuidelinesDocument152 pages03 Na CB GuidelinesPutri Zahra ArdiyanitaNo ratings yet
- Lost in Knowledge Translation: Time For A Map?Document12 pagesLost in Knowledge Translation: Time For A Map?Elaine SilveiraNo ratings yet
- Health Expectations - 2017 - Rojas García - Impact and Experiences of Delayed Discharge A Mixed Studies Systematic ReviewDocument16 pagesHealth Expectations - 2017 - Rojas García - Impact and Experiences of Delayed Discharge A Mixed Studies Systematic ReviewGabriela ObonNo ratings yet
- Swart 2016Document7 pagesSwart 2016TommysNo ratings yet
- The Pap Test and Bethesda 2014: ReviewDocument12 pagesThe Pap Test and Bethesda 2014: ReviewIndhumathiNo ratings yet
- Jama Orkin 2021 SC 210001 1626283660.02954Document9 pagesJama Orkin 2021 SC 210001 1626283660.02954vaideeswari kumarNo ratings yet
- Drenaje de Secreciones Subglóticas para La Prevención de La Neumonía Asociada A Ventilación Mecánica Revisión Sistemática y MetanálisisDocument7 pagesDrenaje de Secreciones Subglóticas para La Prevención de La Neumonía Asociada A Ventilación Mecánica Revisión Sistemática y MetanálisisrobertoNo ratings yet
- Weaning An Adult Patient From Invasive Mechanical VentilationDocument22 pagesWeaning An Adult Patient From Invasive Mechanical VentilationYuanda ArztNo ratings yet
- 2012 Guides Blood TransfusionDocument4 pages2012 Guides Blood TransfusionRandy Mar TagudarNo ratings yet
- Recognition of Clinical Deterioration, A Clinical Leadership Opportunity For Nurse ExecutiveDocument6 pagesRecognition of Clinical Deterioration, A Clinical Leadership Opportunity For Nurse ExecutivePAULA SORAIA CHENNo ratings yet
- Literature Review Final DraftDocument8 pagesLiterature Review Final Draftapi-521003884No ratings yet
- Developing A Neonatal Unit Ventilation Protocol For The Preterm BabyDocument6 pagesDeveloping A Neonatal Unit Ventilation Protocol For The Preterm BabyMALIK MANASRAHNo ratings yet
- CAP in AdultsDocument46 pagesCAP in AdultsKatheryn HernandezAlvarezNo ratings yet
- Journal SatuDocument6 pagesJournal SatuIntan DwiNo ratings yet
- Factors That Influence Validity (1) : Study Design, Doses and PowerDocument2 pagesFactors That Influence Validity (1) : Study Design, Doses and PowerHabib DawarNo ratings yet
- Asthma Diagnosis SystemDocument10 pagesAsthma Diagnosis SystemAbanum ChuksNo ratings yet
- Airway Pressure Release Ventilation A Review of The Evidence, Theoretical Benefits, and Alternative Titration StrategiesDocument9 pagesAirway Pressure Release Ventilation A Review of The Evidence, Theoretical Benefits, and Alternative Titration StrategiesJose Morato E FlavianeNo ratings yet
- Prolonged Mechanical Ventilation Alters Diaphragmatic Structure and FunctionDocument17 pagesProlonged Mechanical Ventilation Alters Diaphragmatic Structure and FunctionmvmarentesNo ratings yet
- Risk-Based Reboot: New WHO Guidance For Laboratory BiosafetyDocument2 pagesRisk-Based Reboot: New WHO Guidance For Laboratory BiosafetyArturo Eduardo Huarcaya OntiverosNo ratings yet
- Fluid Administration For Acute Circulatory Dysfunction Using Basic Monitoring Narrative Review and Expert Panel Recommendations From An ESICM Task Force Maurizio CecconDocument12 pagesFluid Administration For Acute Circulatory Dysfunction Using Basic Monitoring Narrative Review and Expert Panel Recommendations From An ESICM Task Force Maurizio CecconEllys Macías PeraltaNo ratings yet
- Reliability of Pulse Pressure and Stroke Volume Variation in Assessing Fluid Responsiveness in The Operating Room: A Metanalysis and A MetaregressionDocument12 pagesReliability of Pulse Pressure and Stroke Volume Variation in Assessing Fluid Responsiveness in The Operating Room: A Metanalysis and A MetaregressionAlida Cubas CabanillasNo ratings yet
- Digital Chest Drainage System Versus Traditional Chest Drainage System After Pulmonary Resection: A Systematic Review and Meta-AnalysisDocument6 pagesDigital Chest Drainage System Versus Traditional Chest Drainage System After Pulmonary Resection: A Systematic Review and Meta-AnalysisSamantha AdrianneNo ratings yet
- Laboratory Test Turnaround Time and The Needs of Medical CareDocument2 pagesLaboratory Test Turnaround Time and The Needs of Medical Caremy accountNo ratings yet
- Proposal PaperDocument29 pagesProposal Paperapi-698305049No ratings yet
- Chest: Section I: GuidelinesDocument21 pagesChest: Section I: GuidelinesMonica PetreNo ratings yet
- Bronchiolitis and Pulse Oximetry Choosing Wisely With A Technological Pandora's Box JAMA Pediatrics 2016Document2 pagesBronchiolitis and Pulse Oximetry Choosing Wisely With A Technological Pandora's Box JAMA Pediatrics 2016nathalia_pastasNo ratings yet
- p2 - Patients and Carers Experiences of InteractingDocument12 pagesp2 - Patients and Carers Experiences of InteractingShruthi KrishnamoorthyNo ratings yet
- Hex 21 41Document16 pagesHex 21 41fadedoyinNo ratings yet
- Bethesda 2014Document12 pagesBethesda 2014VinhNo ratings yet
- Paramedics and Scope of Practice: EditorialsDocument3 pagesParamedics and Scope of Practice: Editorialsbibin babuNo ratings yet
- Wiedeman Comparison of Two Fluid-Management Strategies in Acute Lung Injury NEJM 2006Document12 pagesWiedeman Comparison of Two Fluid-Management Strategies in Acute Lung Injury NEJM 2006Della Puspita SariNo ratings yet
- Raise Standards For Preclinical Cancer ResearchDocument3 pagesRaise Standards For Preclinical Cancer ResearchMiguel CastroNo ratings yet
- Parenteral Products: The Preparation and Quality Control of Products for InjectionFrom EverandParenteral Products: The Preparation and Quality Control of Products for InjectionNo ratings yet
- ESI Triage by Dr. Ryan MiranoDocument34 pagesESI Triage by Dr. Ryan MiranoEarl Kristoffer PiranteNo ratings yet
- Standard Nurse Protocols FOR Tuberculosis (TB)Document39 pagesStandard Nurse Protocols FOR Tuberculosis (TB)Wikan Purwihantoro SudarmajiNo ratings yet
- ICN, 2015 (Pakai)Document107 pagesICN, 2015 (Pakai)Annisa Nurfiatul AiniNo ratings yet
- The in Uence of Ow Rate On Breathing Circuit Compliance and Tidal Volume Delivered To Patients in Mechanical VentilationDocument12 pagesThe in Uence of Ow Rate On Breathing Circuit Compliance and Tidal Volume Delivered To Patients in Mechanical VentilationWikan Purwihantoro SudarmajiNo ratings yet
- CheckLists-5 2022Document2 pagesCheckLists-5 2022Wikan Purwihantoro SudarmajiNo ratings yet
- 6167 37766 1 PBDocument7 pages6167 37766 1 PBMica ElaNo ratings yet
- 4675 10359 2 PBDocument7 pages4675 10359 2 PBMonica BorjaNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaWikan Purwihantoro SudarmajiNo ratings yet
- Paans 2011Document18 pagesPaans 2011Wikan Purwihantoro SudarmajiNo ratings yet
- ScopusresultsDocument1 pageScopusresultsWikan Purwihantoro SudarmajiNo ratings yet
- Artikel 2 (Using SNL)Document4 pagesArtikel 2 (Using SNL)Wikan Purwihantoro SudarmajiNo ratings yet
- Em-2014 Recommendations For Hospital Emergency Codes FinalDocument35 pagesEm-2014 Recommendations For Hospital Emergency Codes FinalWikan Purwihantoro SudarmajiNo ratings yet
- 1472 6955 11 11Document12 pages1472 6955 11 11Wikan Purwihantoro SudarmajiNo ratings yet
- Elisa Family The Next Level 3 2018 enDocument26 pagesElisa Family The Next Level 3 2018 enWikan Purwihantoro SudarmajiNo ratings yet
- PK 1-4 SortingDocument16 pagesPK 1-4 SortingWikan Purwihantoro SudarmajiNo ratings yet
- Ch18 Zinke3e Short Section 5Document23 pagesCh18 Zinke3e Short Section 5HaNo ratings yet
- Febrile Antigens Package InsertDocument2 pagesFebrile Antigens Package InsertAhmed AliNo ratings yet
- "First Time in History" - Cancer Vanishes For Every Patient in Drug TrialDocument3 pages"First Time in History" - Cancer Vanishes For Every Patient in Drug TrialDIPIN JAINNo ratings yet
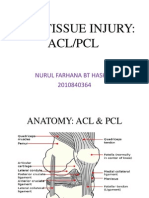
- Acl PCL PresentationDocument17 pagesAcl PCL PresentationSafwan Idham RamlanNo ratings yet
- Unit I (Hypertension) Part 1Document77 pagesUnit I (Hypertension) Part 1RUSSEL JAN ROJASNo ratings yet
- Hubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutDocument7 pagesHubungan Pelaksanaan Screening Test Menelan Dengan Kejadian Disfagia Pada Pasien Baru Yang Menderita Stroke AkutmaydamayNo ratings yet
- Serpentina Treatment: A Review of LiteratureDocument11 pagesSerpentina Treatment: A Review of LiteratureZahra FirdausNo ratings yet
- Wound Cleansing: Benefits of Hypochlorous AcidDocument5 pagesWound Cleansing: Benefits of Hypochlorous Acidlps DiamondNo ratings yet
- Drug Study (Ceftriaxone)Document2 pagesDrug Study (Ceftriaxone)Keij Araneta93% (15)
- Bragdon V AbbottDocument22 pagesBragdon V AbbottZNo ratings yet
- Leech TherapyDocument2 pagesLeech TherapyEmelda MelNo ratings yet
- First Pediatric Quiz-مدمجDocument145 pagesFirst Pediatric Quiz-مدمجjadarcNo ratings yet
- Birth Control Made Simple 2010Document5 pagesBirth Control Made Simple 2010Richard WahlNo ratings yet
- Pediatric Rheumatology CarteDocument628 pagesPediatric Rheumatology CarteCrischentian BrinzaNo ratings yet
- An Adhd Epidemic and Other Misdiagnosed Mental Illnesses in Children Final ReportDocument108 pagesAn Adhd Epidemic and Other Misdiagnosed Mental Illnesses in Children Final Reportapi-350787181100% (1)
- Trusted Medical Answers-In Seconds.: Helminth InfectionsDocument33 pagesTrusted Medical Answers-In Seconds.: Helminth InfectionsntnquynhproNo ratings yet
- Chapter 24 INTERSTITIAL LUNG DISEASEDocument10 pagesChapter 24 INTERSTITIAL LUNG DISEASEZahra Margrette SchuckNo ratings yet
- 303 - Gastrointestinal Physiology) Gastric Secretion - The Cephalic - Gastric PhaseDocument5 pages303 - Gastrointestinal Physiology) Gastric Secretion - The Cephalic - Gastric Phasekedas70No ratings yet
- Introduction To Physical ExaminationDocument13 pagesIntroduction To Physical ExaminationMuhammad SyarmineNo ratings yet
- Peroneus Longus Tendon Rupture: A Case Report: BackgroundDocument14 pagesPeroneus Longus Tendon Rupture: A Case Report: BackgroundAlgivar DaudNo ratings yet
- Lesson Plan Reproductive SystemDocument3 pagesLesson Plan Reproductive SystemMaryJoyceReyes50% (2)
- HEMAREV Merged PDFDocument120 pagesHEMAREV Merged PDFMae BaechuNo ratings yet
- Hughes Selection of Remedy PDFDocument47 pagesHughes Selection of Remedy PDFNavya VaddimukkalaNo ratings yet
- Lucy Mayienga CV RecentDocument3 pagesLucy Mayienga CV Recentlucy.mayiengaNo ratings yet
- Designing Reliable Practices For IV Push Medication Use Handout PDFDocument17 pagesDesigning Reliable Practices For IV Push Medication Use Handout PDFalejandromfunes1749No ratings yet
- Covid 19 Sars - Cov-2 Rna: Department of Molecular BiologyDocument1 pageCovid 19 Sars - Cov-2 Rna: Department of Molecular BiologyKunal DagaNo ratings yet
- Asha Monthly Reports - Aprial MonthDocument64 pagesAsha Monthly Reports - Aprial MonthSamuel SourabNo ratings yet
- Compartment Syndrome AinulDocument32 pagesCompartment Syndrome AinulShidevNo ratings yet
- Neuromuscular Blocking AgentsnewDocument22 pagesNeuromuscular Blocking Agentsnewvinay0717100% (1)
- Recist Book 1 1 HandoutDocument26 pagesRecist Book 1 1 HandoutJose Alfonso CNo ratings yet