You might also like
- Autism Resource GuideDocument22 pagesAutism Resource Guideapi-541216557No ratings yet
- Interpersonal CommunicationDocument17 pagesInterpersonal Communicationmill0% (1)
- Oregon SOS Audit On Child WelfareDocument49 pagesOregon SOS Audit On Child WelfareSinclair Broadcast Group - Eugene100% (1)
- Sds 101 Stand-Up Project - Group 2Document19 pagesSds 101 Stand-Up Project - Group 2Jeydrew TVNo ratings yet
- Community Needs Assessment Postpartum DepressionDocument26 pagesCommunity Needs Assessment Postpartum Depressionapi-607536364No ratings yet
- Business Plan For The Adyaka Orohans Vocational Training Institute (Aovti) ProjectDocument13 pagesBusiness Plan For The Adyaka Orohans Vocational Training Institute (Aovti) Projecta.hasan670No ratings yet
- Homeroom Guidance: Quarter 3 - Module 8: The Power (Positivity, Optimism and Resiliency) To CopeDocument13 pagesHomeroom Guidance: Quarter 3 - Module 8: The Power (Positivity, Optimism and Resiliency) To CopeRoela Marie Albania100% (1)
- HCIN-541 Module 7 Final Project Business Proposal PaperDocument11 pagesHCIN-541 Module 7 Final Project Business Proposal PaperJulian CorralNo ratings yet
- Ogl 350 Scap 1Document14 pagesOgl 350 Scap 1api-685951540No ratings yet
- Nursing 1003 ProjectDocument15 pagesNursing 1003 Project2sdbbkry2hNo ratings yet
- Assessment On The Effectiveness of Adopt A Child Program in Community Development - CompressDocument17 pagesAssessment On The Effectiveness of Adopt A Child Program in Community Development - CompressLowis Sydney VillaNo ratings yet
- Teen Pregnancy Dec08 PDFDocument28 pagesTeen Pregnancy Dec08 PDFDwi WulandariNo ratings yet
- Mental Health and Children at Glance 23Document2 pagesMental Health and Children at Glance 23WVLT NewsNo ratings yet
- Final ProjectDocument5 pagesFinal Projectapi-701085431No ratings yet
- Mendocino County Grand Jury - A Priority To Challenge The Plight of Young People, June 3, 2010Document7 pagesMendocino County Grand Jury - A Priority To Challenge The Plight of Young People, June 3, 2010Rick ThomaNo ratings yet
- Pediatric Community Mental HealthDocument35 pagesPediatric Community Mental HealthShirleyNo ratings yet
- National Child Protection Statistics 2014: Prevention (Cbcap) Prevention (Capta)Document14 pagesNational Child Protection Statistics 2014: Prevention (Cbcap) Prevention (Capta)MarryRose Dela Torre FerrancoNo ratings yet
- Dep2008 0058Document31 pagesDep2008 0058Sonia DzierzyńskaNo ratings yet
- Observation and Assessment Research Paper Davis AllisonDocument63 pagesObservation and Assessment Research Paper Davis Allisonapi-609125940No ratings yet
- Community Project Fall Risk Prevention 1Document15 pagesCommunity Project Fall Risk Prevention 1api-639508852No ratings yet
- Project Proposal 1Document7 pagesProject Proposal 1Imteaz Ibn YasinNo ratings yet
- Scaling Up A Large Program in Rural Areas: May 2020 WebinarDocument35 pagesScaling Up A Large Program in Rural Areas: May 2020 WebinarAlguémNo ratings yet
- 1 RUNNING HEAD: Organizational Analysis: County of San BernardinoDocument4 pages1 RUNNING HEAD: Organizational Analysis: County of San BernardinopaulinestrakaNo ratings yet
- HCA 112 Capstone ProjectDocument16 pagesHCA 112 Capstone ProjectDr Nithya RajanNo ratings yet
- Social Protection Project PhiDocument3 pagesSocial Protection Project PhiMark GabonNo ratings yet
- Wipro CSR Projects 1702149035Document46 pagesWipro CSR Projects 1702149035Liberal CatNo ratings yet
- Assessment On The Effectiveness of Adopt A Child Program in Community DevelopmentDocument17 pagesAssessment On The Effectiveness of Adopt A Child Program in Community DevelopmentjuvysobrevillaNo ratings yet
- Community Health Project Paper 1Document11 pagesCommunity Health Project Paper 1api-630699625No ratings yet
- Key Words: Conditional Cash Transfer, Pantawid Pamilyang Pilipino Program, Perceived EffectsDocument55 pagesKey Words: Conditional Cash Transfer, Pantawid Pamilyang Pilipino Program, Perceived EffectsButchoy GemaoNo ratings yet
- Fca Practice Module 3Document12 pagesFca Practice Module 3Asteria BersanoNo ratings yet
- Poster: Canadian Family Policy Assessment Tool (2012)Document1 pagePoster: Canadian Family Policy Assessment Tool (2012)kidSKAN DirectorNo ratings yet
- HMG National Replication BriefDocument2 pagesHMG National Replication BriefvmeederNo ratings yet
- Proposal 2Document19 pagesProposal 2api-543853977No ratings yet
- Capacity Building 2022Document3 pagesCapacity Building 2022MSWD CamilingNo ratings yet
- Landscaping Process Zone&ADP Urban JKTDocument11 pagesLandscaping Process Zone&ADP Urban JKTOrang KedurusNo ratings yet
- PGI - MANIMTIM - Reaction Paper 10 - OHEPDocument1 pagePGI - MANIMTIM - Reaction Paper 10 - OHEPKim Adarem Joy ManimtimNo ratings yet
- Cordero, VLM - Community Bodies Dealing With The Child WelfareDocument20 pagesCordero, VLM - Community Bodies Dealing With The Child WelfareAlfred AtalinNo ratings yet
- Little Smiles Children's Oral Health Awareness Initiative: Final Program PlanDocument10 pagesLittle Smiles Children's Oral Health Awareness Initiative: Final Program Planapi-535394902No ratings yet
- Intern Website ReviewsDocument5 pagesIntern Website Reviewsapi-644788908No ratings yet
- Ed 243 Riley PresentationDocument13 pagesEd 243 Riley Presentationapi-523248253No ratings yet
- Recommendation AnnexesDocument217 pagesRecommendation AnnexesNeil ShellardNo ratings yet
- MCSD Reopening Plan 20-21Document39 pagesMCSD Reopening Plan 20-21News 8 WROCNo ratings yet
- Faktor Determinan Balita Stunting Pada DDocument14 pagesFaktor Determinan Balita Stunting Pada DVIRGINA PUTRINo ratings yet
- Nurs473 Community PresentationDocument15 pagesNurs473 Community Presentationapi-732023243No ratings yet
- Final PresentationDocument15 pagesFinal Presentationaisha bashirNo ratings yet
- Program Grant Proposal - EditedDocument24 pagesProgram Grant Proposal - Editedeunicemukui62No ratings yet
- Project PresentationDocument9 pagesProject Presentationapi-652480224No ratings yet
- Kalusugan NG Bata Pahalagahan - Outreach Program For ChildrenDocument25 pagesKalusugan NG Bata Pahalagahan - Outreach Program For ChildrenKimberly AcolNo ratings yet
- Homelessness in West SpringvilleDocument34 pagesHomelessness in West Springvilleapi-457077559No ratings yet
- EAPP (Concept Paper)Document6 pagesEAPP (Concept Paper)Fate TanyNo ratings yet
- 7 Rural-RemoteTribal 508Document22 pages7 Rural-RemoteTribal 508Esayase AsnakeNo ratings yet
- 4A N415 Community Care PlanDocument38 pages4A N415 Community Care PlanVhince PiscoNo ratings yet
- Impact of Covid 19 On Children and YouthDocument11 pagesImpact of Covid 19 On Children and YouthNinikoenhe MagalhãesNo ratings yet
- Arkansas Foster Care Strategic Plan 23 18Document19 pagesArkansas Foster Care Strategic Plan 23 18Madison HardcastleNo ratings yet
- 3494-Article Text-10674-1-10-20221208Document12 pages3494-Article Text-10674-1-10-20221208Tep B 21083 Luki LoviandiNo ratings yet
- Community DiagnosisDocument12 pagesCommunity Diagnosisodoyo7381No ratings yet
- Doylestown Hospital 2016 Community Health Needs Assessment Implementation PlanDocument7 pagesDoylestown Hospital 2016 Community Health Needs Assessment Implementation Planapi-342989632No ratings yet
- Cco The State of Childrens Mental Health ServicesDocument32 pagesCco The State of Childrens Mental Health ServicesAnnisa FitriaNo ratings yet
- Rural Child Care Innovation ProgramDocument28 pagesRural Child Care Innovation PrograminforumdocsNo ratings yet
- Incubating Indonesia’s Young Entrepreneurs:: Recommendations for Improving Development ProgramsFrom EverandIncubating Indonesia’s Young Entrepreneurs:: Recommendations for Improving Development ProgramsNo ratings yet
- Chapter 7Document5 pagesChapter 7JULLIE CARMELLE H. CHATTONo ratings yet
- Lesson For Week 9 - 11 Ix. The Moral AgentDocument15 pagesLesson For Week 9 - 11 Ix. The Moral Agentroselyn ayensaNo ratings yet
- MGT502 - Organizational Behaviour: Solved by Muhammad AfaaqDocument8 pagesMGT502 - Organizational Behaviour: Solved by Muhammad AfaaqAsif FareedNo ratings yet
- Student 4.1 Amount and Distribution of PracticeDocument29 pagesStudent 4.1 Amount and Distribution of PracticeFlicksh0tNo ratings yet
- The Structure and Development of Internal Working ModelsDocument15 pagesThe Structure and Development of Internal Working ModelsEsteli189No ratings yet
- Module 1: Getting Started: Lesson 1: Course OverviewDocument6 pagesModule 1: Getting Started: Lesson 1: Course OverviewJulie Pelleja MacaraegNo ratings yet
- Ethics and Values in Engineering Profession (Ese - 2018) - ReportsDocument14 pagesEthics and Values in Engineering Profession (Ese - 2018) - ReportsArindam DasNo ratings yet
- Characteristics of Slow LearnerDocument5 pagesCharacteristics of Slow LearnerFrejoles, Melva MaeNo ratings yet
- Thesis Topic 2Document4 pagesThesis Topic 2Akanksha VinnyNo ratings yet
- Lesson 2 Cont. in Euthenics 1Document9 pagesLesson 2 Cont. in Euthenics 1Darlene De PazNo ratings yet
- ACT Handout RDW - 2023Document16 pagesACT Handout RDW - 2023Cs ChiaraNo ratings yet
- FAMILY RolesDocument10 pagesFAMILY RolessamuelNo ratings yet
- The Journey of AdolescentsDocument17 pagesThe Journey of Adolescentscristina esplanaNo ratings yet
- Santos, Matthew Christian, DS - ABLCS 1-3 - UTS - Lesson On Culture, Beauty and The Female BodyDocument4 pagesSantos, Matthew Christian, DS - ABLCS 1-3 - UTS - Lesson On Culture, Beauty and The Female BodyMatthew Christian SantosNo ratings yet
- Self EsteemDocument2 pagesSelf EsteemSana HasanNo ratings yet
- Steinberg Et Al 1992 Ethnic Differences in Adolescent Achievement An Ecological Perspective SUMDocument4 pagesSteinberg Et Al 1992 Ethnic Differences in Adolescent Achievement An Ecological Perspective SUMLinh MaiNo ratings yet
- Health Care Ethics 1Document3 pagesHealth Care Ethics 1Nathalie kate petallarNo ratings yet
- CAE Writing ModelDocument3 pagesCAE Writing Modelchen ruanjingNo ratings yet
- School-Age Children Development Information - Mount Sinai - New York - 1636456827972Document6 pagesSchool-Age Children Development Information - Mount Sinai - New York - 1636456827972IMRAN USSINo ratings yet
- Scope and Sequence PYP Grade 6Document5 pagesScope and Sequence PYP Grade 6malissa nugeraNo ratings yet
- Ersey Blanchard Situational Leadership TheoryDocument19 pagesErsey Blanchard Situational Leadership TheoryJohn Reigh CatipayNo ratings yet
- Revised Self-And Family ManagementDocument9 pagesRevised Self-And Family ManagementGriyaNo ratings yet
- Implementation of Preference Selection Index (PSI) Method in The System of Support The Decision of The Selectionof Exemplary NursesDocument8 pagesImplementation of Preference Selection Index (PSI) Method in The System of Support The Decision of The Selectionof Exemplary Nurseszhafirah rahmadiniNo ratings yet
- Last Will and TestamentDocument2 pagesLast Will and TestamentKirithika HariharanNo ratings yet
- Decent Work EmploymentDocument7 pagesDecent Work EmploymentNovelyn PuaNo ratings yet
- Gen Z LearnersDocument2 pagesGen Z LearnersJSL Art collectionsNo ratings yet
- Thesis Chap1 5Document38 pagesThesis Chap1 5Llanevel VelascoNo ratings yet
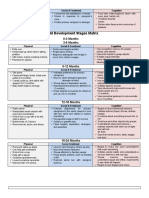
- Child Development Stages Matrix: 0-3 Months 3-6 MonthsDocument6 pagesChild Development Stages Matrix: 0-3 Months 3-6 MonthsJoenard Sadorra CabaelNo ratings yet