You might also like
- John Dee - Sigillum Dei Aemeth or Seal of The Truth of God EnglishDocument2 pagesJohn Dee - Sigillum Dei Aemeth or Seal of The Truth of God Englishsatyr70286% (7)
- A Book of Beasts PDFDocument32 pagesA Book of Beasts PDFbrad drac100% (2)
- 721b TransmissionDocument36 pages721b TransmissionMohamed Mahgoub100% (1)
- Bloodborne Pathogens TrainingDocument28 pagesBloodborne Pathogens TrainingPeter GolanskiNo ratings yet
- MLT 107 Chapter 3 5 Infection Cont and QADocument29 pagesMLT 107 Chapter 3 5 Infection Cont and QACristina CunhaNo ratings yet
- 13 - Bloodborn PathogenDocument55 pages13 - Bloodborn PathogenghufranahmedkhanNo ratings yet
- Bloodborne Pathogens: Module Nr. 12Document55 pagesBloodborne Pathogens: Module Nr. 12Kh MoNo ratings yet
- Needle Stick InjuryDocument24 pagesNeedle Stick InjuryShivani TiwariNo ratings yet
- Bloodborne Pathogens 2019Document27 pagesBloodborne Pathogens 2019stephcuzinoNo ratings yet
- Introduction To Infection Prevention: Integrated Health Systems Strengthening-Service Delivery ActivityDocument38 pagesIntroduction To Infection Prevention: Integrated Health Systems Strengthening-Service Delivery ActivityMona KhanNo ratings yet
- Infectious Disease Control & Prevention: Introduction ToDocument75 pagesInfectious Disease Control & Prevention: Introduction ToJamie J. BartonNo ratings yet
- Week 4. Infection Control Fall 22-23Document40 pagesWeek 4. Infection Control Fall 22-23aisha.hadid31No ratings yet
- Nursing Clients With HIV Infection and AIDS: Learning ObjectivesDocument11 pagesNursing Clients With HIV Infection and AIDS: Learning Objectivesmorynayim-1No ratings yet
- Nursing Clients With HIV Infection and AIDS: Learning ObjectivesDocument11 pagesNursing Clients With HIV Infection and AIDS: Learning Objectivesmorynayim-1No ratings yet
- Jakartamicrobiological Risk AssessmentDocument20 pagesJakartamicrobiological Risk AssessmentAnna FiqriNo ratings yet
- Occupational Biohazards: Dr. Tajuddin Bantacut Department of Agroindustrial Technology Bogor Agricultural UniversityDocument29 pagesOccupational Biohazards: Dr. Tajuddin Bantacut Department of Agroindustrial Technology Bogor Agricultural UniversityAbdur RahmanNo ratings yet
- Infection Prevention and Control in The Endoscopy UnitDocument44 pagesInfection Prevention and Control in The Endoscopy Unityus sulisyantoNo ratings yet
- Needle Sticks Sharps Injuries: FactsDocument31 pagesNeedle Sticks Sharps Injuries: FactsDr. Ashish Jawarkar67% (3)
- Bloodborne Pathogens: The Occupational Safety and Health Administration StandardDocument55 pagesBloodborne Pathogens: The Occupational Safety and Health Administration StandardfatmawatiNo ratings yet
- Characterization of Pathogens: We Strive For Wisdom Chapter-2Document29 pagesCharacterization of Pathogens: We Strive For Wisdom Chapter-2AZ Amanii BossNo ratings yet
- NOTES CD Lecture Generic 2022Document182 pagesNOTES CD Lecture Generic 2022Meryville JacildoNo ratings yet
- LBS - The Economics of Pandemic - The Case of Covid-19Document98 pagesLBS - The Economics of Pandemic - The Case of Covid-19AryttNo ratings yet
- Phleb LecDocument44 pagesPhleb LecMikee Patricia TrinidadNo ratings yet
- ID EVD SudanVirusUganda EVDOverview 2022-11-02Document43 pagesID EVD SudanVirusUganda EVDOverview 2022-11-02Alan AzadNo ratings yet
- Communicable Disease PresentationDocument67 pagesCommunicable Disease PresentationMonaNo ratings yet
- Patient Management Course ReviewDocument76 pagesPatient Management Course ReviewclaraNo ratings yet
- PBH101 Lecture3 & 4Document57 pagesPBH101 Lecture3 & 4Peter CalvinsanNo ratings yet
- Human Immunodeficiency Virus (HIV) : Mohammad Al-Rawashdeh 54-5th CourseDocument39 pagesHuman Immunodeficiency Virus (HIV) : Mohammad Al-Rawashdeh 54-5th CourseMohammadSAL-RawashdehNo ratings yet
- BBP3 ADocument67 pagesBBP3 AMostafa AbdullahNo ratings yet
- Safety in Laboratory - Blok 1.4Document58 pagesSafety in Laboratory - Blok 1.4adystiNo ratings yet
- Hoeltke Chapter2 RevisedDocument44 pagesHoeltke Chapter2 RevisedKarby LeeNo ratings yet
- Needle Stick InjuryDocument27 pagesNeedle Stick InjuryVishal ThakareNo ratings yet
- If HP CDC Ipsm Covid 19 Imm OrientationDocument77 pagesIf HP CDC Ipsm Covid 19 Imm OrientationTheFisherman FriasNo ratings yet
- EpidemiologDocument35 pagesEpidemiologs.zainabtanweerNo ratings yet
- A Deadly Scourge: Role of The Microbiologists in The Investigation of An OutbreakDocument42 pagesA Deadly Scourge: Role of The Microbiologists in The Investigation of An Outbreaktummalapalli venkateswara raoNo ratings yet
- Lecuniversal PrecautionsDocument34 pagesLecuniversal PrecautionsRabia TahirNo ratings yet
- KMU CHN-LLL Final 2022Document20 pagesKMU CHN-LLL Final 2022AamirNo ratings yet
- Multidrug-Resistant - Organisms (MDROsDocument59 pagesMultidrug-Resistant - Organisms (MDROsTariq100% (2)
- Tatalaksana Post Exposure Prophylaxis Post Exposure ProphylaxisDocument29 pagesTatalaksana Post Exposure Prophylaxis Post Exposure Prophylaxisvianney boroNo ratings yet
- Clostridium Difficile Infection (CDI) : Prevention PrimerDocument80 pagesClostridium Difficile Infection (CDI) : Prevention PrimererpNo ratings yet
- Outbreak InvestigationDocument31 pagesOutbreak InvestigationSyed Sanan shahNo ratings yet
- Communicable DiseasesDocument123 pagesCommunicable DiseasesAndrea Marie T. Artajo-BoheromNo ratings yet
- Covid 19 Infection Prevention and Control CasicsDocument46 pagesCovid 19 Infection Prevention and Control CasicsCainta Mpl Jail TanNo ratings yet
- Ethical Issues in HIV Vaccine Trial (Notes)Document63 pagesEthical Issues in HIV Vaccine Trial (Notes)Nuur Mursyiidah MuhammadNo ratings yet
- Slides Covid19 FinalDocument106 pagesSlides Covid19 FinalgigigiugiNo ratings yet
- Manifestasi Klinis HIVDocument111 pagesManifestasi Klinis HIVFebrina EvaNo ratings yet
- Infection Control - Examiner RoleplayDocument3 pagesInfection Control - Examiner Roleplaysanju ghimireNo ratings yet
- 2 Infection Control in EndodonticsDocument117 pages2 Infection Control in EndodonticsShubham NaikNo ratings yet
- Biosafety in The LaboratoryDocument74 pagesBiosafety in The Laboratorykimotosan100% (1)
- Safety On Accident Site:: Bloodborne Pathogen AwarenessDocument69 pagesSafety On Accident Site:: Bloodborne Pathogen Awarenessdaily absurdNo ratings yet
- AIDSDocument34 pagesAIDSCrystal Ann TadiamonNo ratings yet
- First Lecture - Infection Control - WrittenDocument25 pagesFirst Lecture - Infection Control - Writtenmohamed elshialNo ratings yet
- Basic Principles and Procedures of Infection Prevenetion and ControlDocument98 pagesBasic Principles and Procedures of Infection Prevenetion and Controlbasl.hazm34No ratings yet
- Biosafety TrainingDocument28 pagesBiosafety TrainingIbrahim YaseenNo ratings yet
- Management of Hiv Infection and AidsDocument41 pagesManagement of Hiv Infection and AidsNamene zeniNo ratings yet
- Covid LBSDocument117 pagesCovid LBSj_siddharth24No ratings yet
- Module TM1:: 08 Understanding Clinical & Biomedical TerminologyDocument29 pagesModule TM1:: 08 Understanding Clinical & Biomedical TerminologyLarry CalubagNo ratings yet
- Hepatitis CCRN KFSH&RC Asma AlshehriDocument33 pagesHepatitis CCRN KFSH&RC Asma AlshehriasmashNo ratings yet
- Halodoc Webinar On COVID 2020-03-21 V 0.4Document75 pagesHalodoc Webinar On COVID 2020-03-21 V 0.4Gabriella NelwanNo ratings yet
- 312 Unit I (Lecture 2& 3)Document62 pages312 Unit I (Lecture 2& 3)FoxNo ratings yet
- Hiv& AidsDocument203 pagesHiv& Aidsclaire wacukaNo ratings yet
- Materi - Webinar - Dr. Apt. Tiana Milanda, M.si.Document39 pagesMateri - Webinar - Dr. Apt. Tiana Milanda, M.si.DWI RAHMA HALIDANo ratings yet
- Practical Manual for Detection of Parasites in Feces, Blood and Urine SamplesFrom EverandPractical Manual for Detection of Parasites in Feces, Blood and Urine SamplesNo ratings yet
- 1121FT2 Ir1415ccgbDocument8 pages1121FT2 Ir1415ccgbMohamed MahgoubNo ratings yet
- GNB MP Overview enDocument16 pagesGNB MP Overview enMohamed MahgoubNo ratings yet
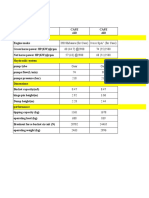
- Comparison SkidDocument2 pagesComparison SkidMohamed MahgoubNo ratings yet
- 621F Tier2Document12 pages621F Tier2Mohamed MahgoubNo ratings yet
- Ahmed Adel2Document177 pagesAhmed Adel2Mohamed MahgoubNo ratings yet
- Certificate: Eng. Mohamed Mahgoub ZakiDocument1 pageCertificate: Eng. Mohamed Mahgoub ZakiMohamed MahgoubNo ratings yet
- Application LSE - Egypt-1Document4 pagesApplication LSE - Egypt-1Mohamed MahgoubNo ratings yet
- I. Chapter 7 - Fire, Egress and 1st AidDocument76 pagesI. Chapter 7 - Fire, Egress and 1st AidMohamed MahgoubNo ratings yet
- Data ElectricDocument1 pageData ElectricMohamed MahgoubNo ratings yet
- Global Safety Strategy DiagramDocument3 pagesGlobal Safety Strategy DiagramMohamed MahgoubNo ratings yet
- J. Chapter 8 - HazwoperDocument118 pagesJ. Chapter 8 - HazwoperMohamed MahgoubNo ratings yet
- B. IntroductionDocument5 pagesB. IntroductionMohamed MahgoubNo ratings yet
- 2.1 Training and Basic SafetyDocument192 pages2.1 Training and Basic SafetyHatem HusseinNo ratings yet
- FDocument1 pageFMohamed MahgoubNo ratings yet
- Crane Lifting PlanDocument3 pagesCrane Lifting PlanMohamed MahgoubNo ratings yet
- Service Manual SM17 - 002 - 071.00: Boom Telescope Cylinder CalibrationDocument8 pagesService Manual SM17 - 002 - 071.00: Boom Telescope Cylinder CalibrationMohamed MahgoubNo ratings yet
- Load Summation and Limitation Electronics: Crane-SumdDocument3 pagesLoad Summation and Limitation Electronics: Crane-SumdMohamed MahgoubNo ratings yet
- Service Manual SM17 - 002 - 071.00: Boom Telescope Cylinder CalibrationDocument8 pagesService Manual SM17 - 002 - 071.00: Boom Telescope Cylinder CalibrationMohamed MahgoubNo ratings yet
- Load Limitation Electronics With 1 Set Point: Bridgeboy - 1RDocument2 pagesLoad Limitation Electronics With 1 Set Point: Bridgeboy - 1RMohamed MahgoubNo ratings yet
- CASE CAM WHL W0110-10E Lift Cylinder PistonDocument5 pagesCASE CAM WHL W0110-10E Lift Cylinder PistonMohamed MahgoubNo ratings yet
- An Objective of Dress Code PolicyDocument4 pagesAn Objective of Dress Code PolicySiddhraj Singh KushwahaNo ratings yet
- Correct Translation of 2-16Document19 pagesCorrect Translation of 2-16muhammad_zubair708110No ratings yet
- Investment Opportunities: Equity MarketsDocument38 pagesInvestment Opportunities: Equity MarketsRanjeet SinghNo ratings yet
- Steps To Create Payment Document in R12 PayablesDocument2 pagesSteps To Create Payment Document in R12 Payablessrees_15No ratings yet
- Analgesic ActivityDocument4 pagesAnalgesic ActivitypranaliankitNo ratings yet
- TSH TestDocument5 pagesTSH TestdenalynNo ratings yet
- Characters: Philadelphia Here I Come! by Brian FrielDocument4 pagesCharacters: Philadelphia Here I Come! by Brian FrielDominic LenihanNo ratings yet
- Eco 407Document4 pagesEco 407LUnweiNo ratings yet
- The Absurdity of The Official DoctrineDocument5 pagesThe Absurdity of The Official DoctrinemarpeqNo ratings yet
- Chapter 101-160Document297 pagesChapter 101-160Dipankar BoruahNo ratings yet
- G.R. No. 201354 September 21, 2016Document11 pagesG.R. No. 201354 September 21, 2016Winston YutaNo ratings yet
- Potential Nursing Diagnosis Problem Fdar / NCP: Activity # 2Document2 pagesPotential Nursing Diagnosis Problem Fdar / NCP: Activity # 2Karl KiwisNo ratings yet
- Quality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisDocument15 pagesQuality of Life After Functional Endoscopic Sinus Surgery in Patients With Chronic RhinosinusitisNarendraNo ratings yet
- Telesis Events - Construction Contract Essentials - WorkbookDocument52 pagesTelesis Events - Construction Contract Essentials - WorkbookassmonkeysNo ratings yet
- Niper SyllabusDocument9 pagesNiper SyllabusdirghayuNo ratings yet
- Father Saturnino Urios University Engineering and Technology Program Butuan CityDocument16 pagesFather Saturnino Urios University Engineering and Technology Program Butuan CityTalal SultanNo ratings yet
- The Impact of Climatic and Cultural Factors On Openings in Traditional Houses in MaharashtraDocument14 pagesThe Impact of Climatic and Cultural Factors On Openings in Traditional Houses in Maharashtracoldflame81No ratings yet
- Organisational Behaviour - II India Yamaha Motors Interim PPT (Download To View Full Presentation)Document28 pagesOrganisational Behaviour - II India Yamaha Motors Interim PPT (Download To View Full Presentation)mahtaabkNo ratings yet
- Merger of Bank of Karad Ltd. (BOK) With Bank of India (BOI)Document17 pagesMerger of Bank of Karad Ltd. (BOK) With Bank of India (BOI)Alexander DeckerNo ratings yet
- World War I Almanac Almanacs of American WarsDocument561 pagesWorld War I Almanac Almanacs of American WarsMatheus Benedito100% (1)
- TestFunda - Puzzles 1Document39 pagesTestFunda - Puzzles 1Gerald KohNo ratings yet
- Noorul Islam Centre For Higher Education Noorul Islam University, Kumaracoil M.E. Biomedical Instrumentation Curriculum & Syllabus Semester IDocument26 pagesNoorul Islam Centre For Higher Education Noorul Islam University, Kumaracoil M.E. Biomedical Instrumentation Curriculum & Syllabus Semester Iisaac RNo ratings yet
- Rule Against Multiplicity and Child PornoDocument3 pagesRule Against Multiplicity and Child PornoHouston Criminal Lawyer John T. FloydNo ratings yet
- Chuyen de GerundifninitiveDocument7 pagesChuyen de GerundifninitiveThao TrinhNo ratings yet
- Taschen Tradecat 2014 01 Tam 1402181720 Id 775697 PDFDocument57 pagesTaschen Tradecat 2014 01 Tam 1402181720 Id 775697 PDFLuiza Oliveira100% (1)
- Noceda vs. Court of Appeals (Property Case)Document3 pagesNoceda vs. Court of Appeals (Property Case)jokuanNo ratings yet
- Kuo SzuYu 2014 PHD ThesisDocument261 pagesKuo SzuYu 2014 PHD ThesiskatandeNo ratings yet
- 17PME328E: Process Planning and Cost EstimationDocument48 pages17PME328E: Process Planning and Cost EstimationDeepak MisraNo ratings yet