You might also like
- Fault Diagnosis and Sustainable Control of Wind Turbines: Robust Data-Driven and Model-Based StrategiesFrom EverandFault Diagnosis and Sustainable Control of Wind Turbines: Robust Data-Driven and Model-Based StrategiesRating: 4 out of 5 stars4/5 (1)
- 2019 Article 2021Document16 pages2019 Article 2021gloNo ratings yet
- Medical Device Management SoftwareDocument6 pagesMedical Device Management SoftwareMuhammad IzzuddinNo ratings yet
- Developing An In-House Computerized Maintenance Management System For HospitalsDocument9 pagesDeveloping An In-House Computerized Maintenance Management System For Hospitalsاديب جازمNo ratings yet
- Evidence-Based Mathematical Maintenance Model For Medical EquipmentDocument5 pagesEvidence-Based Mathematical Maintenance Model For Medical EquipmentJessica HrovatinNo ratings yet
- How to Identify and Analyze Hospital RisksDocument12 pagesHow to Identify and Analyze Hospital Risksver_at_workNo ratings yet
- Hospital Equipment Planning &selectionpmrpntDocument26 pagesHospital Equipment Planning &selectionpmrpntCHIKKABASAPPA90% (10)
- Critical Care Environment: BOX 2.1 Business Case: Sample HeadingsDocument8 pagesCritical Care Environment: BOX 2.1 Business Case: Sample HeadingsIqbal Yusuf AshariNo ratings yet
- State of The Art - Precautionary MaintenaceDocument12 pagesState of The Art - Precautionary MaintenacejavinavasNo ratings yet
- Final ThesisDocument69 pagesFinal ThesisAswin WSNo ratings yet
- E (OTDA: O T D A) : Valuation of An Operating Theatre Design by A Software Program Perating Heatre Esign NalyzerDocument8 pagesE (OTDA: O T D A) : Valuation of An Operating Theatre Design by A Software Program Perating Heatre Esign NalyzerOlim AriyaNo ratings yet
- Proposal For An Implementation Framework For DigitDocument18 pagesProposal For An Implementation Framework For DigitAndréNo ratings yet
- Predictive Maintenance (PDM) Structure Using Internet of Things (Iot) For Mechanical Equipment Used Into Hospitals in RwandaDocument23 pagesPredictive Maintenance (PDM) Structure Using Internet of Things (Iot) For Mechanical Equipment Used Into Hospitals in RwandaHassamNo ratings yet
- IHFG Part e CompleteDocument8 pagesIHFG Part e Completevirtech1No ratings yet
- Part e CompleteDocument9 pagesPart e CompleteSonia PareekNo ratings yet
- Cuestionario Nro. 1Document10 pagesCuestionario Nro. 1Ronald ContrerasNo ratings yet
- EU US PostMarket Surveillance Whitepaper PDFDocument7 pagesEU US PostMarket Surveillance Whitepaper PDFLakshmana Perumal RamarajNo ratings yet
- Protocols and procedures for medical equipment managementDocument9 pagesProtocols and procedures for medical equipment managementAmir100% (1)
- Maintenance strategies overview focusing on concepts and approachesDocument14 pagesMaintenance strategies overview focusing on concepts and approachesThaierNo ratings yet
- Kevin Moon Proposed DoH Maintenance StandardsDocument35 pagesKevin Moon Proposed DoH Maintenance StandardsKarthik RajaNo ratings yet
- Integrated Healthcare Facilities InfrastructureDocument44 pagesIntegrated Healthcare Facilities InfrastructuremubarakelkadyNo ratings yet
- A Fuzzy Approach For Medical Equipment Replacement Planning: KeywordsDocument7 pagesA Fuzzy Approach For Medical Equipment Replacement Planning: Keywordsthe7king the7kingNo ratings yet
- Maintenance Management AssignmentDocument20 pagesMaintenance Management AssignmentRiya GuptaNo ratings yet
- MaintenanceDocument2 pagesMaintenanceKarim Ahmed El SayedNo ratings yet
- Providence Healthcare Stevens County Utility Management PlanDocument9 pagesProvidence Healthcare Stevens County Utility Management PlanSuci GusriNo ratings yet
- MR-EC.01.01.01EP9-Utility-Systems-Management-Plan-2021Document19 pagesMR-EC.01.01.01EP9-Utility-Systems-Management-Plan-2021LourenaChanNo ratings yet
- A Simple Quantitative Model For Replacement of Medical Equipment Proposed To Developing CountriesDocument4 pagesA Simple Quantitative Model For Replacement of Medical Equipment Proposed To Developing Countriesanon_242490661No ratings yet
- Of Active Medical Devices-Malaysia Standard MS 2058:2009 Syed Mustafa KamalDocument6 pagesOf Active Medical Devices-Malaysia Standard MS 2058:2009 Syed Mustafa KamalArif YamanNo ratings yet
- A Review of Prognostics and Health Management of Machine ToolsDocument22 pagesA Review of Prognostics and Health Management of Machine ToolsAchraf KachafNo ratings yet
- 368-1425-1-PBDocument9 pages368-1425-1-PBKassahun AwokeNo ratings yet
- Medical Devices Inspection and Maintenance A Literature ReviewDocument11 pagesMedical Devices Inspection and Maintenance A Literature ReviewAya AhmedNo ratings yet
- Me6012 - Maintenance EngineeringDocument13 pagesMe6012 - Maintenance EngineeringIyswaryaNo ratings yet
- ME2037 Maintenance EngineeringDocument51 pagesME2037 Maintenance EngineeringVicky Vignesh100% (1)
- Medical Equipment Management Plan 11 021Document7 pagesMedical Equipment Management Plan 11 021Diniyas Rorisa100% (1)
- Section-I 3) Explain The Various Components of Logistics Management. 10Document12 pagesSection-I 3) Explain The Various Components of Logistics Management. 10Rajni KumariNo ratings yet
- Medip, IJRMS-7730 ODocument6 pagesMedip, IJRMS-7730 OsundarcetNo ratings yet
- Biomedical Equip PlanningDocument6 pagesBiomedical Equip PlanningOcwich FrancisNo ratings yet
- Ensuring The Safety of Critical Systems Is of Utmost Importance in Various IndustriesDocument4 pagesEnsuring The Safety of Critical Systems Is of Utmost Importance in Various IndustriesKrizzia FloresNo ratings yet
- Ar Fieldsafety PolicyDocument5 pagesAr Fieldsafety Policyme.ddfNo ratings yet
- A New Approach For Preventive MaintenancDocument4 pagesA New Approach For Preventive MaintenancLâm Phạm100% (1)
- ME2037 Maintenance EngineeringDocument46 pagesME2037 Maintenance Engineeringrp0212100% (2)
- HTM & Biomedical EngineeringDocument27 pagesHTM & Biomedical Engineeringheru pratiknoNo ratings yet
- Part e IntroductionDocument5 pagesPart e IntroductionDhairyasheel PatilNo ratings yet
- Maintenance 2 Mark PDFDocument38 pagesMaintenance 2 Mark PDFSaravanan HNo ratings yet
- Clinical Engineering Functions and EvolutionDocument47 pagesClinical Engineering Functions and Evolutionamirali.bme4527No ratings yet
- Efficient Equipment Management Software for HospitalsDocument6 pagesEfficient Equipment Management Software for HospitalshendranatjNo ratings yet
- Guidelines On Infection Control Practice in The Clinic Setting Dec 2011Document52 pagesGuidelines On Infection Control Practice in The Clinic Setting Dec 2011Just MahasiswaNo ratings yet
- Clinical Engineering in MexicoDocument7 pagesClinical Engineering in MexicoAna LauraNo ratings yet
- Medical Equipment Management - Binseng WangDocument5 pagesMedical Equipment Management - Binseng WangIanca MoraesNo ratings yet
- Testing Multi-Function Medical MonitorsDocument16 pagesTesting Multi-Function Medical MonitorsKarthik Raj VNo ratings yet
- Mantenimiento de EquiposDocument13 pagesMantenimiento de EquiposLAURA CAMILA FRANCO ZAMBRANONo ratings yet
- mca-27-00002 (1)Document21 pagesmca-27-00002 (1)Rittik Kumar NaskarNo ratings yet
- Medical Devices Inspection and Maintenance A Literature ReviewDocument10 pagesMedical Devices Inspection and Maintenance A Literature ReviewlchirinoscautinhoNo ratings yet
- Clinical Risk Management 1.23Document8 pagesClinical Risk Management 1.23MICHAEL BONFACE OJIAMBONo ratings yet
- Risk Based Maintanance PDFDocument9 pagesRisk Based Maintanance PDFRafaelPachecoNo ratings yet
- Itudorache,+8 UDROIU PLESANU Approaches+to+Medical+EquipmentDocument7 pagesItudorache,+8 UDROIU PLESANU Approaches+to+Medical+EquipmentMohd Khidir GazaliNo ratings yet
- Duke Hospital Utility PlanDocument4 pagesDuke Hospital Utility PlanusakNo ratings yet
- 02 Clinical EngineeringDocument47 pages02 Clinical EngineeringasdfghjhgfdsaasdfghjNo ratings yet
- A Fuzzy TOPSIS-Based Approach To Maintenance Strategy Selection: A Case StudyDocument8 pagesA Fuzzy TOPSIS-Based Approach To Maintenance Strategy Selection: A Case StudyteddiyfentawNo ratings yet
- MM 25th AugustDocument12 pagesMM 25th AugustAbhishek ChaubeyNo ratings yet
- Catalog Schneider Var SetDocument72 pagesCatalog Schneider Var SetMihai Butnaru-PaladeNo ratings yet
- In Touch Tag ViewerDocument28 pagesIn Touch Tag ViewerGalang Pandu SatyaNo ratings yet
- Wilkerson CompanyDocument26 pagesWilkerson CompanyChris Vincent50% (2)
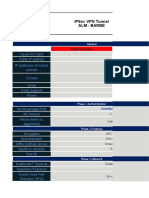
- IPSec VPN Tunnel DetailsDocument5 pagesIPSec VPN Tunnel DetailsjgdNo ratings yet
- 25 Mechanical Engineering Interview Questions and Answers - Freshers, ExperiencedDocument3 pages25 Mechanical Engineering Interview Questions and Answers - Freshers, Experiencedmehul kapadiaNo ratings yet
- KW DTV Release NotesDocument13 pagesKW DTV Release NotesMauricio AguilarNo ratings yet
- 1220 Developing Possible SolutionsDocument7 pages1220 Developing Possible SolutionsMannyNo ratings yet
- Dissertation Brinkmeier 061124Document180 pagesDissertation Brinkmeier 061124AlbertoCostoyaNo ratings yet
- Cisco Catalyst 9300 Switch DatasheetDocument14 pagesCisco Catalyst 9300 Switch Datasheetbonsai todayNo ratings yet
- Assignment On Institution EconomicsDocument3 pagesAssignment On Institution EconomicsSinhaShehabNo ratings yet
- KISTLER Torque Sensor Type 4503ADocument6 pagesKISTLER Torque Sensor Type 4503ASantiago MolinaNo ratings yet
- VMware VCloud Networking and Security 5.1 - Tech OverviewDocument25 pagesVMware VCloud Networking and Security 5.1 - Tech OverviewSanjeev TyagiNo ratings yet
- Quiz MeasurementDocument2 pagesQuiz MeasurementRAC REOPTANo ratings yet
- Elcometer Digital Surface Profile Gauge 223Document10 pagesElcometer Digital Surface Profile Gauge 223Stephen LeighNo ratings yet
- CS92 en LRDocument8 pagesCS92 en LRAnderson AntunesNo ratings yet
- Til 1719Document4 pagesTil 1719FRANCISCO JOSE GARCIA IBAÑEZNo ratings yet
- A01 PLCDocument78 pagesA01 PLCDaniel salgado yañezNo ratings yet
- IEC 61467 (Ed1.0) Insulators AC Power Arc Tests PDFDocument11 pagesIEC 61467 (Ed1.0) Insulators AC Power Arc Tests PDFLucyana RosaNo ratings yet
- ISHO Handover Issues in CM Mode INTERNALDocument19 pagesISHO Handover Issues in CM Mode INTERNALFachrudinSudomoNo ratings yet
- Linde HPR 02 DatasheetDocument48 pagesLinde HPR 02 Datasheetdavor1414100% (1)
- Handbook of Practice Management - 9th EditionDocument307 pagesHandbook of Practice Management - 9th EditiongheorghemonicaNo ratings yet
- UniPunch SystemDocument52 pagesUniPunch Systemmohammad2k2No ratings yet
- Bluetooth HandoutDocument26 pagesBluetooth HandoutsaafinlandNo ratings yet
- Multitenant Applications SuccinctlyDocument153 pagesMultitenant Applications SuccinctlyJonathan Lazo IrusNo ratings yet
- Installation, Service, and User Guide: IBM System Storage SAN80B-4Document87 pagesInstallation, Service, and User Guide: IBM System Storage SAN80B-4Fouad BaroutNo ratings yet
- Mindwave Mobile & ArduinoDocument12 pagesMindwave Mobile & ArduinoMuhammad Shafiq Abdul KarimNo ratings yet
- Stinger MRT-36A DSL Access Concentrator: Applications BenefitsDocument2 pagesStinger MRT-36A DSL Access Concentrator: Applications BenefitsJuanNo ratings yet
- Sepam Series 20 and Its Optional ModulesDocument2 pagesSepam Series 20 and Its Optional ModulesEphraem KalisNo ratings yet
- BAPI Types and RFC Function ModulesDocument6 pagesBAPI Types and RFC Function ModulesMrconfusionSapNo ratings yet