You might also like
- Pediatric Endocrinology Review MCQsDocument104 pagesPediatric Endocrinology Review MCQsTirou100% (1)
- DermatitisDocument44 pagesDermatitisAyuMardewi50% (2)
- Contact Dermatitis BJD Guidelines May 2009Document9 pagesContact Dermatitis BJD Guidelines May 2009Cynthia OktariszaNo ratings yet
- Acute Heart Failure WORKBOOKDocument28 pagesAcute Heart Failure WORKBOOKFadhlan ABNo ratings yet
- Fibromyalgia Clinical Guidelines and Treatments PDFDocument198 pagesFibromyalgia Clinical Guidelines and Treatments PDFLore Barrera100% (1)
- HRPB Drug Formulary 2018Document244 pagesHRPB Drug Formulary 2018tiuwangNo ratings yet
- Allergic Contact DermatitisDocument11 pagesAllergic Contact DermatitisSf AkhadiyatiNo ratings yet
- Contact Dermatitis: Allergic and IrritantDocument9 pagesContact Dermatitis: Allergic and IrritantatikaNo ratings yet
- Allergic Contact DermatitisDocument6 pagesAllergic Contact DermatitisCrysnaNo ratings yet
- BAHAN Chapter 24Document33 pagesBAHAN Chapter 24S FznsNo ratings yet
- Identifying The Cause of Contact DermatitisDocument6 pagesIdentifying The Cause of Contact DermatitiswadejackNo ratings yet
- Dermatitis Kontak Alergi (DKA)Document25 pagesDermatitis Kontak Alergi (DKA)tryhabibullahNo ratings yet
- Case Report Dermatitis ContactDocument10 pagesCase Report Dermatitis ContactMuhammad Aktora Tarigan100% (1)
- Systemic Contact DermatitisDocument6 pagesSystemic Contact DermatitisUty PutriNo ratings yet
- Allergic Contact Dermatitis GuideDocument12 pagesAllergic Contact Dermatitis GuideDaisy HamdaliNo ratings yet
- Contact Dermatitis: Key PointsDocument8 pagesContact Dermatitis: Key Pointssaimon reyNo ratings yet
- JR DR Arif Dermatitis Atopi Kelompok 1Document46 pagesJR DR Arif Dermatitis Atopi Kelompok 1regina pingkanNo ratings yet
- Eczema Types, Causes, and Management in 40 CharactersDocument56 pagesEczema Types, Causes, and Management in 40 CharactersAdam AriwibawaNo ratings yet
- Bercak MerahDocument16 pagesBercak MerahFary SatriadiNo ratings yet
- Jurnal Reading DADocument18 pagesJurnal Reading DAWinendy Deo HaryantoNo ratings yet
- Dermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityDocument34 pagesDermatitis & Urticaria: Department of Dermato Venereology Faculty of Medicine Gadjah Mada UniversityadystiNo ratings yet
- Penatalaksanaan Dermatitis AtopicDocument13 pagesPenatalaksanaan Dermatitis AtopicDini MayrisdayaniNo ratings yet
- AD Review PDFDocument13 pagesAD Review PDFalfarizyjefryNo ratings yet
- Irritant Contact Dermatitis: Practice EssentialsDocument4 pagesIrritant Contact Dermatitis: Practice EssentialsHiedajatNo ratings yet
- A Hands On Approach To Patch TestingDocument11 pagesA Hands On Approach To Patch TestingSundar RamanathanNo ratings yet
- Dermatitis: K. Puviyarasi Dept of MSN MNCDocument26 pagesDermatitis: K. Puviyarasi Dept of MSN MNCPuviyarasi100% (2)
- Seminar: Sinéad M Langan, Alan D Irvine, Stephan WeidingerDocument16 pagesSeminar: Sinéad M Langan, Alan D Irvine, Stephan WeidingerMaria Paulina EstradaNo ratings yet
- Lancet Atopic DermatitisDocument10 pagesLancet Atopic DermatitisRui CarmoNo ratings yet
- Diagnosis and Treatment of Allergic Skin Disorders in The ElderlyDocument9 pagesDiagnosis and Treatment of Allergic Skin Disorders in The ElderlyfelipetheNo ratings yet
- DddsDocument50 pagesDddsOsama AlhaseNo ratings yet
- Chapter 24:: Allergic Contact Dermatitis:: Jake E. Turrentine, Michael P. SheehanDocument19 pagesChapter 24:: Allergic Contact Dermatitis:: Jake E. Turrentine, Michael P. SheehanInke LubisNo ratings yet
- DermaDocument9 pagesDermaZain Ul AbidinNo ratings yet
- Atopic DermatitisDocument6 pagesAtopic DermatitisJhuli Elizabeth CNo ratings yet
- Atopic Dermatitis & MelanomaDocument15 pagesAtopic Dermatitis & MelanomaShalu RjNo ratings yet
- Allergic Skin Conditions - Causes, Clinical Features and TreatmentDocument4 pagesAllergic Skin Conditions - Causes, Clinical Features and TreatmentAnshuman PadheeNo ratings yet
- Canine Atopic Dermatitis - A Practical ApproachDocument15 pagesCanine Atopic Dermatitis - A Practical ApproachlirmvetNo ratings yet
- 1476 ArticleText 6472 1 10 20100118 PDFDocument6 pages1476 ArticleText 6472 1 10 20100118 PDFJayantiNo ratings yet
- Hand EczemaDocument18 pagesHand EczemaNella AztyNo ratings yet
- Contact Dermatitis in ChildrenDocument6 pagesContact Dermatitis in ChildrenYogi SanjayaNo ratings yet
- Dermatitis & Eczema 2007Document83 pagesDermatitis & Eczema 2007La Ode Rinaldi100% (2)
- Dyshidrotic Eczema: BackgroundDocument5 pagesDyshidrotic Eczema: BackgroundHiedajatNo ratings yet
- Dermatitis vs Eczema: Understanding the DifferencesDocument136 pagesDermatitis vs Eczema: Understanding the DifferencesfachruNo ratings yet
- ECZEMA: AN OVERVIEW OF TYPES AND MANAGEMENTDocument47 pagesECZEMA: AN OVERVIEW OF TYPES AND MANAGEMENTSalsabila Al-Basheer100% (1)
- Makieieva Atopic Dermatitis, Allergic Rhinitis 21-34153Document22 pagesMakieieva Atopic Dermatitis, Allergic Rhinitis 21-34153Ibtissame BadadNo ratings yet
- Dermatological History and Examination: Key PointsDocument3 pagesDermatological History and Examination: Key Pointsasalizwa ludlalaNo ratings yet
- Cap. 10. SKIN DISEASES PDFDocument14 pagesCap. 10. SKIN DISEASES PDFoana policarpovNo ratings yet
- Hand Eczema TreatmentDocument9 pagesHand Eczema TreatmentCharcravorti AyatollahsNo ratings yet
- Dermatitis Kontak Alergi Laporan KasusDocument10 pagesDermatitis Kontak Alergi Laporan Kasushy diyNo ratings yet
- Penyakit Dermatitis: Dr. Kristo A. Nababan, SPKKDocument47 pagesPenyakit Dermatitis: Dr. Kristo A. Nababan, SPKKDaniel Suarez ParapatNo ratings yet
- Atopic DermatitisDocument14 pagesAtopic DermatitisityNo ratings yet
- Eczema and DermatitisDocument24 pagesEczema and Dermatitisjackofmanytrades100% (1)
- Eczema, Psoriasis, Cutaneous Infections, Acne, and Other Common Skin DisordersDocument6 pagesEczema, Psoriasis, Cutaneous Infections, Acne, and Other Common Skin DisordersElrey InocianNo ratings yet
- Pecial Article Raca SpecjalnaDocument18 pagesPecial Article Raca SpecjalnaKrzysztof ŁukasikNo ratings yet
- Eczema & Psoriasis Treatment GuideDocument69 pagesEczema & Psoriasis Treatment GuideKeith OmwoyoNo ratings yet
- Atopic Dermatitis: A Review of Diagnosis and TreatmentDocument11 pagesAtopic Dermatitis: A Review of Diagnosis and TreatmentLeona NgadiahNo ratings yet
- Jurnal FixDocument27 pagesJurnal FixPanji Wage KosasihNo ratings yet
- EL Skin Allergies Scratching The Surface PatientDocument1 pageEL Skin Allergies Scratching The Surface PatientHulkuhulk 1No ratings yet
- Atopic DermatitisDocument8 pagesAtopic DermatitiskoesantoNo ratings yet
- Atopic Dermatitis Seminar GuideDocument7 pagesAtopic Dermatitis Seminar GuidetazzycaNo ratings yet
- Complete Medical Guide for Disease Volume VII; Atopic DermatitisFrom EverandComplete Medical Guide for Disease Volume VII; Atopic DermatitisNo ratings yet
- Practical Patch Testing and Chemical Allergens in Contact DermatitisFrom EverandPractical Patch Testing and Chemical Allergens in Contact DermatitisNo ratings yet
- Contact Urticaria Syndrome: Diagnosis and ManagementFrom EverandContact Urticaria Syndrome: Diagnosis and ManagementAna M. Giménez-ArnauNo ratings yet
- Derm 14julDocument103 pagesDerm 14juljoseph joshua ngushualNo ratings yet
- Dermatology Module 2Document16 pagesDermatology Module 2joseph joshua ngushualNo ratings yet
- Posttest AnswersDocument2 pagesPosttest Answersjoseph joshua ngushualNo ratings yet
- Topical and Systemic Corticosteroids: Potency Rankings, Uses, and Side EffectsDocument4 pagesTopical and Systemic Corticosteroids: Potency Rankings, Uses, and Side Effectsjoseph joshua ngushualNo ratings yet
- Shock - Critical Care Medicine - MSD Manual Professional EditionDocument11 pagesShock - Critical Care Medicine - MSD Manual Professional Editionazaria zhafirahNo ratings yet
- Daily Monitoring TGL 24 Desember 2020Document12 pagesDaily Monitoring TGL 24 Desember 2020nada cintakuNo ratings yet
- Pneumonia Patho & SignsDocument1 pagePneumonia Patho & SignsVishalNo ratings yet
- Amyotrophic Lateral Sclerosis (Als)Document6 pagesAmyotrophic Lateral Sclerosis (Als)Michelle Teodoro100% (1)
- (Mebooksfree Net) Oxf&tex&uro&sur&1stDocument1,201 pages(Mebooksfree Net) Oxf&tex&uro&sur&1stMohammadSAL-Rawashdeh100% (2)
- Risperidone - Drug Information - UpToDateDocument81 pagesRisperidone - Drug Information - UpToDateEduardo AguilarNo ratings yet
- Obstructive Jaundice: Causes, Symptoms and DiagnosisDocument69 pagesObstructive Jaundice: Causes, Symptoms and DiagnosisAbdirazak HassanNo ratings yet
- NCM 2144 - Respiratory AgentsDocument61 pagesNCM 2144 - Respiratory AgentsBena JagonobNo ratings yet
- Causes of Metabolic AcidosisDocument3 pagesCauses of Metabolic AcidosisLorenn AdarnaNo ratings yet
- Core Curriculum NefrolitiasisDocument13 pagesCore Curriculum NefrolitiasisOscar MoralesNo ratings yet
- Microbiology Bacteria Section ReviewDocument18 pagesMicrobiology Bacteria Section ReviewSaransh GhimireNo ratings yet
- Diseases: Soekimin Dept. of Anatomical Patology Universitas Sumatera Utara MedanDocument124 pagesDiseases: Soekimin Dept. of Anatomical Patology Universitas Sumatera Utara MedanZayadhaHazriniNo ratings yet
- Professional Development of Obstetrician & GynaecologistDocument116 pagesProfessional Development of Obstetrician & GynaecologistDeepa YadavNo ratings yet
- Overcome Chronic and Autoimmune Diseases with a Cleansing DietDocument11 pagesOvercome Chronic and Autoimmune Diseases with a Cleansing Dietromalfio100% (1)
- Dermatology Resident NotesDocument37 pagesDermatology Resident Notesedgar mandengNo ratings yet
- B.C. Soldiers Buried in The NetherlandsDocument3 pagesB.C. Soldiers Buried in The NetherlandsThe ProvinceNo ratings yet
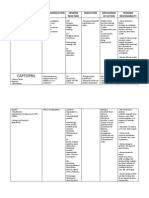
- Amlodipine Captopril MetronidazoleDocument5 pagesAmlodipine Captopril Metronidazolekhrysty1506No ratings yet
- Liquorice Root: A Monograph On World Wide Trade ofDocument12 pagesLiquorice Root: A Monograph On World Wide Trade ofVinay MishraNo ratings yet
- Lopressor (Metoprolol) 100mgDocument2 pagesLopressor (Metoprolol) 100mgAdrianne Bazo100% (2)
- NCLEX Exam Basic 3Document6 pagesNCLEX Exam Basic 3Maria Garcia Pimentel Vanguardia IINo ratings yet
- Anaphylaxis in Infants - UpToDateDocument21 pagesAnaphylaxis in Infants - UpToDatealinaNo ratings yet
- 17 Nrcme Practice TestDocument19 pages17 Nrcme Practice Testdr_milan100% (1)
- Peripheral Nerve DisordersDocument33 pagesPeripheral Nerve Disordersbpt2No ratings yet
- IsjsjsDocument13 pagesIsjsjsMarsh MallowNo ratings yet
- Micro Q Final 2Document45 pagesMicro Q Final 2Rashed Aiman Sameer Alsayyed AlalqamawiNo ratings yet