You might also like
- Anal Sex Secrets - A Guide To Great Anal Sex by Svetlana Ivanova - Read OnlineDocument4 pagesAnal Sex Secrets - A Guide To Great Anal Sex by Svetlana Ivanova - Read Onlinezamin4pak50% (2)
- CBT For Anxiety ManualDocument45 pagesCBT For Anxiety ManualCY Wu33% (3)
- Unit 10 CounsellingDocument24 pagesUnit 10 CounsellingMbuguz BeNel MuyaNo ratings yet
- Intercultural UnderstandingDocument15 pagesIntercultural Understandingapi-626136134No ratings yet
- 3 Techniques Used in Counselling Process in SchoolsDocument6 pages3 Techniques Used in Counselling Process in SchoolstimothyNo ratings yet
- Gouty GCPDocument48 pagesGouty GCPKylie GolindangNo ratings yet
- 6) Ethical and Legal Aspects in CounselingDocument23 pages6) Ethical and Legal Aspects in CounselingNadia Sultan100% (1)
- Clinical Judgement-An Essential Tool in The Nursing Profession PDFDocument10 pagesClinical Judgement-An Essential Tool in The Nursing Profession PDFNers SenNo ratings yet
- Ethical Issues and Professional AdvocacyDocument7 pagesEthical Issues and Professional AdvocacyShisham FernandezNo ratings yet
- Role of Feed Additives in Bangladesh Poultry Industries in 2003Document10 pagesRole of Feed Additives in Bangladesh Poultry Industries in 2003Md. Morshed AlamNo ratings yet
- Supervision in Clinical Practice A Practitioners Guide (Scaife, Joyce) (Z-Library)Document433 pagesSupervision in Clinical Practice A Practitioners Guide (Scaife, Joyce) (Z-Library)Sébastien MiraultNo ratings yet
- Ethical Practice of SupervisionDocument12 pagesEthical Practice of Supervisionapi-626136134No ratings yet
- Trauma-Informed Supervision Clinical Supervision of Substance Use D o CounselorsaDocument17 pagesTrauma-Informed Supervision Clinical Supervision of Substance Use D o Counselorsaapi-626136134No ratings yet
- Diass Q1 W2 D1Document25 pagesDiass Q1 W2 D1Eric AntonioNo ratings yet
- Supervision-Personal Wellness PlanDocument3 pagesSupervision-Personal Wellness Planapi-626136134No ratings yet
- Self Inspection of Quality AssuranceDocument5 pagesSelf Inspection of Quality Assuranceanoushia alviNo ratings yet
- Vol 19.1 - Sleep Disorders.2013Document252 pagesVol 19.1 - Sleep Disorders.2013Martoiu MariaNo ratings yet
- Disciplines and Ideas in Applied Social ScienceDocument17 pagesDisciplines and Ideas in Applied Social SciencechessieNo ratings yet
- Ethics in Supervision Consideration of The Supervisory Alliance and Countertransference Management of Psychology Doctoral StudentsDocument16 pagesEthics in Supervision Consideration of The Supervisory Alliance and Countertransference Management of Psychology Doctoral Studentsapi-626136134No ratings yet
- Approaches of CounsellingDocument7 pagesApproaches of CounsellingSamjhana Neupane100% (2)
- Arntz 1999 Childhood Imagery Rescripting Paper PDFDocument26 pagesArntz 1999 Childhood Imagery Rescripting Paper PDFelliotNo ratings yet
- Hce Finals Reviewer 11Document12 pagesHce Finals Reviewer 11ChskNo ratings yet
- Hce Finals Reviewer PDFDocument21 pagesHce Finals Reviewer PDFChskNo ratings yet
- Professional Portfolio Assignment Part DDocument6 pagesProfessional Portfolio Assignment Part Dapi-651962342No ratings yet
- Practitioner's Guide To Ethical Decision Making: The Center For Counseling Practice, Policy, and ResearchDocument6 pagesPractitioner's Guide To Ethical Decision Making: The Center For Counseling Practice, Policy, and Researchapi-310813184No ratings yet
- Diass AsaymentDocument2 pagesDiass AsaymentHungryNo ratings yet
- Crit Care Nurse-2012-Robichaux-65-72Document9 pagesCrit Care Nurse-2012-Robichaux-65-72Ana Carina TavaresNo ratings yet
- Professionalism and Ethical Decision MakingDocument3 pagesProfessionalism and Ethical Decision MakingDoaaNo ratings yet
- MODULE IV Converted 2Document29 pagesMODULE IV Converted 2Bangtan J-hopiaNo ratings yet
- Practioner's Guide To Ethical Decision MakingDocument6 pagesPractioner's Guide To Ethical Decision Makingsaurav.das2030No ratings yet
- Running Head: Conceptual Frameworks 1Document7 pagesRunning Head: Conceptual Frameworks 1Jackson KasakuNo ratings yet
- Lec 03 - Ethics in Decision MakingDocument22 pagesLec 03 - Ethics in Decision MakingmonkeNo ratings yet
- Paper - 4Document99 pagesPaper - 4Devyani JaiswalNo ratings yet
- 9663 SV 0 R92 M4Document1 page9663 SV 0 R92 M4sir BryanNo ratings yet
- Tog 12625Document8 pagesTog 12625saeed hasan saeedNo ratings yet
- CounsellingDocument55 pagesCounsellinghasna.psyyNo ratings yet
- Lesson 2 DiassDocument43 pagesLesson 2 DiassAvy Jane VismanosNo ratings yet
- Ethical Decision Making FrameworkDocument2 pagesEthical Decision Making FrameworkShanmugam EkambaramNo ratings yet
- EthicsinCounseling PDFDocument13 pagesEthicsinCounseling PDFPooja Varma100% (1)
- Hume SlidesCarnivalDocument21 pagesHume SlidesCarnivalAngelica CamaraoNo ratings yet
- Clinical Psychology - Midterm ReviewerDocument10 pagesClinical Psychology - Midterm ReviewerALEXIS LAROANo ratings yet
- DIASS Hands OutDocument9 pagesDIASS Hands OutEditha BalolongNo ratings yet
- How Can Leaders Influence ASafety CultureDocument11 pagesHow Can Leaders Influence ASafety CultureGustavo Tapia AvendañoNo ratings yet
- Discipline Lesson 2Document13 pagesDiscipline Lesson 2Jelmer FojasNo ratings yet
- Ethics & ValuesDocument18 pagesEthics & ValuesProf. LNo ratings yet
- Diass Handout 3Document2 pagesDiass Handout 3Charlene Mae GraciasNo ratings yet
- Critical Thinking Nursing ManagementDocument15 pagesCritical Thinking Nursing ManagementJosephine George JojoNo ratings yet
- Issues That Counselors Consider Ethical or Unethical in Counseling Relationship of Learners With Visual Impairment PDFDocument8 pagesIssues That Counselors Consider Ethical or Unethical in Counseling Relationship of Learners With Visual Impairment PDFKrizia PatinoNo ratings yet
- Reviewer LEMA MidtermDocument5 pagesReviewer LEMA Midtermmitchiiro02No ratings yet
- Bhallis Ethical Reflection Part 2Document16 pagesBhallis Ethical Reflection Part 2api-724240837No ratings yet
- Week 4 Diass 3.0Document6 pagesWeek 4 Diass 3.0Niña Reinne Serviñas MapaNo ratings yet
- Counselor Ethical Boundaries and Practices Melissa AguirreDocument8 pagesCounselor Ethical Boundaries and Practices Melissa Aguirreapi-385824900No ratings yet
- Group 7 - Make Ethical Decisions - 12.1.2021Document52 pagesGroup 7 - Make Ethical Decisions - 12.1.2021alia126No ratings yet
- Guidance and Counselling - Types of Counselling Mrs. Remedios CastrilloDocument4 pagesGuidance and Counselling - Types of Counselling Mrs. Remedios CastrilloLeila PañaNo ratings yet
- Competency Areas: Area 1: Professional Responsibilities Area 2: CommunicationDocument16 pagesCompetency Areas: Area 1: Professional Responsibilities Area 2: CommunicationttsxxxNo ratings yet
- CNL-505 T8 E-Portfolio - Benchmark - Counselor Ethical Boundaries and PracticesDocument8 pagesCNL-505 T8 E-Portfolio - Benchmark - Counselor Ethical Boundaries and Practicesmhernandez460No ratings yet
- HIVAnx Counselguide 051409 - 0Document23 pagesHIVAnx Counselguide 051409 - 0takundaNo ratings yet
- Diass Q1 W4-5Document19 pagesDiass Q1 W4-5RosilaArancesUcatNo ratings yet
- Essential Counseling Techniques and SkillsDocument3 pagesEssential Counseling Techniques and SkillsRaymund MativoNo ratings yet
- Ethical & Legal Dimensions of HealthcareDocument9 pagesEthical & Legal Dimensions of HealthcareMark MadridanoNo ratings yet
- UNIT IV VIII Health EducationDocument18 pagesUNIT IV VIII Health Educationshaharymunar2005No ratings yet
- Frameworks For Ethical Decision-Making - PLP1Document23 pagesFrameworks For Ethical Decision-Making - PLP1claire yowsNo ratings yet
- Unit Guidance and Counselling in Nursing: EducationDocument22 pagesUnit Guidance and Counselling in Nursing: EducationRinchin ChhotenNo ratings yet
- Module 3Document8 pagesModule 3Nicol Jay DuriguezNo ratings yet
- Hapter: Alues Thics AND DvocacyDocument4 pagesHapter: Alues Thics AND DvocacyDianna Rose BelenNo ratings yet
- Techniques of CounsellingDocument3 pagesTechniques of CounsellingVictini codeNo ratings yet
- Why An Ethical Decision-Making Framework?Document3 pagesWhy An Ethical Decision-Making Framework?zeezee060No ratings yet
- Guidance 105 Agravante, Ma. CristyDocument8 pagesGuidance 105 Agravante, Ma. CristyMa. Cristy AgravanteNo ratings yet
- DIASS - CounselingDocument54 pagesDIASS - CounselingAlessandra R. CaballeroNo ratings yet
- Clinical Research Associate - The Comprehensive Guide: Vanguard ProfessionalsFrom EverandClinical Research Associate - The Comprehensive Guide: Vanguard ProfessionalsNo ratings yet
- Supervision: Philosophy, Theory, & PlanDocument13 pagesSupervision: Philosophy, Theory, & Planapi-626136134No ratings yet
- BoundariesDocument8 pagesBoundariesapi-626136134No ratings yet
- Mandated Supervision EthicsDocument28 pagesMandated Supervision Ethicsapi-626136134No ratings yet
- Felt SecurityDocument9 pagesFelt Securityapi-626136134No ratings yet
- Psychological ServicesDocument13 pagesPsychological Servicesapi-626136134No ratings yet
- Safe SpaceDocument7 pagesSafe Spaceapi-626136134No ratings yet
- Preventing VT CF and Bo in Forensic Mental HealthDocument13 pagesPreventing VT CF and Bo in Forensic Mental Healthapi-626136134No ratings yet
- Preparing Female Clinicians For Challenging OffendersDocument11 pagesPreparing Female Clinicians For Challenging Offendersapi-626136134No ratings yet
- Supervision Outcomes SurveyDocument2 pagesSupervision Outcomes Surveyapi-626497212No ratings yet
- Falenders Supervisors Self-AssessmentDocument2 pagesFalenders Supervisors Self-Assessmentapi-626136134No ratings yet
- Quarterly-Progress-Report 1Document5 pagesQuarterly-Progress-Report 1api-626136134No ratings yet
- D 0 Ac 0 DB 6235 CB 766 FD 3 BDocument8 pagesD 0 Ac 0 DB 6235 CB 766 FD 3 Bapi-626136134No ratings yet
- Power Dynamics in Supervision ScaleDocument8 pagesPower Dynamics in Supervision Scaleapi-626136134No ratings yet
- Competency BenchmarksDocument30 pagesCompetency Benchmarksapi-626136134No ratings yet
- Constructing and Maintaining Appropriate Boundaries Within Clinical Supervision RelationshipsDocument6 pagesConstructing and Maintaining Appropriate Boundaries Within Clinical Supervision Relationshipsapi-626136134No ratings yet
- Resident-Self-Assessment 1Document4 pagesResident-Self-Assessment 1api-626136134No ratings yet
- Setting A Good Example Supervisors As Work-Life-Friendly Role Models Within The Context of Boundary ManagementDocument11 pagesSetting A Good Example Supervisors As Work-Life-Friendly Role Models Within The Context of Boundary Managementapi-626136134No ratings yet
- 8 DC 5 C 8 Cebfcaaf 6 C 380 CDocument9 pages8 DC 5 C 8 Cebfcaaf 6 C 380 Capi-626136134No ratings yet
- Final-Supervision-Contract 1Document2 pagesFinal-Supervision-Contract 1api-626497212No ratings yet
- Experiential Exposure To The Supervision Competency in Graduate EducationDocument4 pagesExperiential Exposure To The Supervision Competency in Graduate Educationapi-626136134No ratings yet
- Contracting For Group SupervisionDocument5 pagesContracting For Group Supervisionapi-626136134No ratings yet
- HTTP DXDocument17 pagesHTTP DXapi-626136134No ratings yet
- Competent Supervision-Emerging PracticesDocument17 pagesCompetent Supervision-Emerging Practicesapi-626136134No ratings yet
- Republic of The Philippines Congress of The Philippines Metro Manila Sixteenth Congress Third Regular SessionDocument8 pagesRepublic of The Philippines Congress of The Philippines Metro Manila Sixteenth Congress Third Regular SessionChristy Ledesma-NavarroNo ratings yet
- 2 AnticholinesterasesDocument55 pages2 AnticholinesterasesSudhakar LakavathNo ratings yet
- Modele Anglais - Convention Coordonnateur - Version 20220409Document36 pagesModele Anglais - Convention Coordonnateur - Version 20220409SchmoutNo ratings yet
- What Do We Know About The Food We Eat?: Teaching and Learning Activities, Including Assessment OpportunitiesDocument14 pagesWhat Do We Know About The Food We Eat?: Teaching and Learning Activities, Including Assessment OpportunitiesaravindyellowNo ratings yet
- Nursing Core Competencies For Quality LevelDocument5 pagesNursing Core Competencies For Quality Leveljava_biscocho1229No ratings yet
- Akapulko (Cassia Alata) Indication/s: Duration: Nursing ResponsibilitiesDocument16 pagesAkapulko (Cassia Alata) Indication/s: Duration: Nursing ResponsibilitiesEljay Lustria ReyesNo ratings yet
- Go Wyoming (Sept. 17, 2020)Document24 pagesGo Wyoming (Sept. 17, 2020)Watertown Daily TimesNo ratings yet
- Eye Drops and Dispensing Aids: A GuideDocument37 pagesEye Drops and Dispensing Aids: A GuideAamna ShahNo ratings yet
- Digi T Vigilance TestDocument6 pagesDigi T Vigilance TestJillianne FrancoNo ratings yet
- Static Equilibrium and It's Importance - Mulligan-2 PDFDocument14 pagesStatic Equilibrium and It's Importance - Mulligan-2 PDFdrzana78No ratings yet
- MVA ToolkitDocument89 pagesMVA ToolkitVishal RasalNo ratings yet
- Literature Review of Quantitative StudiesDocument5 pagesLiterature Review of Quantitative Studiesd0vidihujam3100% (1)
- Hostel Rules and RegulationsDocument11 pagesHostel Rules and RegulationsAkshet PatelNo ratings yet
- Activity 4 BSN 2 RLE - APGAR and Part2-Ella Nika FangonDocument5 pagesActivity 4 BSN 2 RLE - APGAR and Part2-Ella Nika FangonElla Nika FangonNo ratings yet
- Home Care Catalogue UK Edition 4 Web PDFDocument60 pagesHome Care Catalogue UK Edition 4 Web PDFmanuales tecnicosNo ratings yet
- Griffith, G. M., Totsika, V., Nash, S., & Hastings, R. P. (2011) - I Just Don"t Fit AnywhereDocument15 pagesGriffith, G. M., Totsika, V., Nash, S., & Hastings, R. P. (2011) - I Just Don"t Fit AnywhereTomislav CvrtnjakNo ratings yet
- Daftar PustakaDocument5 pagesDaftar PustakaR Handi BramantoNo ratings yet
- Angelina Hull Student - Heritagehs - Argumentative Essay - Student Name - Class Period - Spring 19 - H English 1Document5 pagesAngelina Hull Student - Heritagehs - Argumentative Essay - Student Name - Class Period - Spring 19 - H English 1api-461590822No ratings yet
- Scope of NursingDocument4 pagesScope of NursingIvy Jenica Mamuad100% (1)
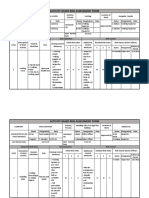
- Activity-Based Risk Assessment Form: Wearing InspectorDocument3 pagesActivity-Based Risk Assessment Form: Wearing InspectorSherly MagatNo ratings yet
- Dengue Fever 2Document5 pagesDengue Fever 2Gayitiri MenonNo ratings yet
- Perioperative Diabetes MXDocument18 pagesPerioperative Diabetes MXTravis SatnarineNo ratings yet
- Mindfulness and PTSDDocument19 pagesMindfulness and PTSDJosie VuckovichNo ratings yet
- Clean Air Act of 1999 Ra 8749Document47 pagesClean Air Act of 1999 Ra 8749Dimple VillaminNo ratings yet