You might also like
- Community Health Nursing AssessmentDocument4 pagesCommunity Health Nursing AssessmentBasema HashhashNo ratings yet
- Family Health Assessment FormDocument12 pagesFamily Health Assessment Formshandy kyle barbadilloNo ratings yet
- Health Condition Form Questionnaire - FINALDocument2 pagesHealth Condition Form Questionnaire - FINALLeonardNo ratings yet
- Chronicle Diabetes Assessment FormDocument8 pagesChronicle Diabetes Assessment FormpriyaNo ratings yet
- San Antonio Metropolitan Health District 332 W. Commerce San Antonio, Texas 78205-2489Document5 pagesSan Antonio Metropolitan Health District 332 W. Commerce San Antonio, Texas 78205-2489Ng MharieNo ratings yet
- Health Literacy of Primary Care Givers of Young Children Common To All To Be InterviewedDocument2 pagesHealth Literacy of Primary Care Givers of Young Children Common To All To Be InterviewedAlbert CorderoNo ratings yet
- Individual Inventory FormDocument2 pagesIndividual Inventory FormALLAN PALATTAO100% (1)
- Case Study Questionnaire For Malnourished ChildrenDocument5 pagesCase Study Questionnaire For Malnourished ChildrenSta Cruz BacnotanNo ratings yet
- SCSIT Family-Assessment-GuideDocument5 pagesSCSIT Family-Assessment-GuideRS BuenavistaNo ratings yet
- Adolescent Intake FormDocument4 pagesAdolescent Intake FormEkaterina TrnblNo ratings yet
- Intake Form Childless 5 YoDocument7 pagesIntake Form Childless 5 Yoconnectsujata1No ratings yet
- Self Care QuizDocument4 pagesSelf Care QuizElizabeth Eckert100% (7)
- 23-24SY BCP AIA Physical Packet Final 1.26.23Document6 pages23-24SY BCP AIA Physical Packet Final 1.26.23Tuan LeNo ratings yet
- Diabetes Assessment FormDocument2 pagesDiabetes Assessment FormAhmad JamaluddinNo ratings yet
- CSI Reflection - Appendix III May 2012Document4 pagesCSI Reflection - Appendix III May 2012Biniam TezeraNo ratings yet
- Initial Patient Intake FormDocument5 pagesInitial Patient Intake Formjpalmes100% (1)
- Apta Eval-Fax Version Asapt 2007Document4 pagesApta Eval-Fax Version Asapt 2007Abdur RasyidNo ratings yet
- Family Health Problem (Common) / Abnormality: (E.g. Uncle)Document2 pagesFamily Health Problem (Common) / Abnormality: (E.g. Uncle)Evelyn Medina100% (1)
- Child or Adolescent Client FormsDocument7 pagesChild or Adolescent Client FormsSodfa EttafakshiNo ratings yet
- Demographic and Pregnancy Questions for Parents of Children with DisabilitiesDocument6 pagesDemographic and Pregnancy Questions for Parents of Children with DisabilitiesCynthia Ann Stephanie SapladNo ratings yet
- AH Form ChildrenDocument11 pagesAH Form ChildrenJosephNo ratings yet
- Daily Health ChecklistDocument1 pageDaily Health ChecklistHosiah-Jen MateoNo ratings yet
- Assessment Tool 2Document14 pagesAssessment Tool 2karenkaren09No ratings yet
- GordonsDocument2 pagesGordonsAngelica OctotNo ratings yet
- GettingtoknowyourinfantDocument1 pageGettingtoknowyourinfantJessica TaishaNo ratings yet
- Community Assessement ToolDocument9 pagesCommunity Assessement ToolAngeli CabalceNo ratings yet
- Background-Questionnaire For PsychiatricDocument7 pagesBackground-Questionnaire For PsychiatricSamuelNo ratings yet
- Psychology Clinic: Adult History FormDocument7 pagesPsychology Clinic: Adult History FormMelanieShiNo ratings yet
- Family Health Problem (Common) / Abnormality: (E.g. Uncle)Document2 pagesFamily Health Problem (Common) / Abnormality: (E.g. Uncle)joseph cyron solidumNo ratings yet
- Barangay Assisted Booking Form: CODE: D1ADocument4 pagesBarangay Assisted Booking Form: CODE: D1AChristine May CagaraNo ratings yet
- Adolescent Biopsychosocial AssessmentDocument10 pagesAdolescent Biopsychosocial AssessmentFar Sultan100% (2)
- NCDC-3 Child Nutritional Status Form A4Document4 pagesNCDC-3 Child Nutritional Status Form A4knock medinaNo ratings yet
- Initial Nutrition AssessmentDocument7 pagesInitial Nutrition Assessmenthabiba arifNo ratings yet
- Nursing Care Health Assessment FormDocument5 pagesNursing Care Health Assessment FormMelanie Bagasol SisonNo ratings yet
- ImmunizationDocument2 pagesImmunizationrajkamalNo ratings yet
- Child BioDocument3 pagesChild BioPammNo ratings yet
- Local Media8154377969260507143 1Document3 pagesLocal Media8154377969260507143 1Johanie Bolawan MamaNo ratings yet
- Registration 2016Document7 pagesRegistration 2016api-304462359No ratings yet
- CARDDocument5 pagesCARDSHAIRUZ DUGAYNo ratings yet
- Gordon's Functional Health Pattern Format and Guide QuestionsDocument5 pagesGordon's Functional Health Pattern Format and Guide QuestionsChristian Christopher Lopez100% (7)
- 04survey Form Urban 2022 EngDocument6 pages04survey Form Urban 2022 EngisahNo ratings yet
- Ped Nutr AssessDocument2 pagesPed Nutr AssessgilangNo ratings yet
- Today's Date: - Name: - Date of Birth - Phone Number: - Age: - Email AddressDocument2 pagesToday's Date: - Name: - Date of Birth - Phone Number: - Age: - Email Addressanedik40No ratings yet
- Indiana Birth WorksheetDocument12 pagesIndiana Birth WorksheettepesssamNo ratings yet
- Factors Influencing COVID-19 Booster Hesitancy in Nursing StudentsDocument8 pagesFactors Influencing COVID-19 Booster Hesitancy in Nursing StudentsChirber MalgapuNo ratings yet
- Nutritional Clinical History Pregnant WomanDocument13 pagesNutritional Clinical History Pregnant WomanScribdTranslationsNo ratings yet
- Assessment Guide ToddlerDocument2 pagesAssessment Guide ToddlerOla Anna GamutinNo ratings yet
- Community Profile: Name: Date: AddressDocument16 pagesCommunity Profile: Name: Date: AddressRoxzen Valera ColladoNo ratings yet
- Medical Information Form Camps Overseas ExcursionsDocument3 pagesMedical Information Form Camps Overseas Excursionskir0011No ratings yet
- Ob Assessment For B VDocument13 pagesOb Assessment For B Vapi-231899545No ratings yet
- Developmental History QuestionnaireDocument6 pagesDevelopmental History QuestionnaireMariana RzNo ratings yet
- T-Asi ENDocument22 pagesT-Asi ENslangevar04100% (1)
- Psychosocial Assessment Form JHS SHS CollegeDocument4 pagesPsychosocial Assessment Form JHS SHS CollegeAndrea InocNo ratings yet
- Parent/Baby Information SheetDocument7 pagesParent/Baby Information SheetJONABELL B YLAGANNo ratings yet
- SPD Patient Health HXDocument1 pageSPD Patient Health HXjosseinNo ratings yet
- Family Assessment GuideDocument4 pagesFamily Assessment Guidejpoti0% (1)
- New Patient RegistrationDocument2 pagesNew Patient Registrationnaveenmi2100% (1)
- Governmental Traumatizing Investigations: An Application to Get a New Toilet, Part IFrom EverandGovernmental Traumatizing Investigations: An Application to Get a New Toilet, Part INo ratings yet
- Nutritional Counselling. How To Motivate People To Correct Their Eating HabitsFrom EverandNutritional Counselling. How To Motivate People To Correct Their Eating HabitsNo ratings yet
- Revision FileDocument14 pagesRevision FileBasema HashhashNo ratings yet
- Journal-Of-18 MicuDocument1 pageJournal-Of-18 MicuBasema HashhashNo ratings yet
- Risperidone Drug StudyDocument2 pagesRisperidone Drug StudyBasema HashhashNo ratings yet
- Dosage and Nursing Responsibilities for OlanzapineDocument1 pageDosage and Nursing Responsibilities for OlanzapineBasema HashhashNo ratings yet
- Renal McqsDocument13 pagesRenal McqsShahabuddin Shaikh100% (1)
- Budgeting Your TimeDocument1 pageBudgeting Your TimeBasema HashhashNo ratings yet
- Depression, Bipolar Disorder Chronic Pain InsomniaDocument4 pagesDepression, Bipolar Disorder Chronic Pain InsomniaBasema HashhashNo ratings yet
- Processrecording EnglishDocument5 pagesProcessrecording EnglishBasema HashhashNo ratings yet
- Hashhash, Abtisam Review MoiveDocument2 pagesHashhash, Abtisam Review MoiveBasema HashhashNo ratings yet
- Alalag, Elsie: "The Impact of Access To Immunization Information On Vaccine Acceptance in Three Countries"Document4 pagesAlalag, Elsie: "The Impact of Access To Immunization Information On Vaccine Acceptance in Three Countries"Basema HashhashNo ratings yet
- B - Laroco James C.Document5 pagesB - Laroco James C.Basema HashhashNo ratings yet
- Fdar 22-24 2Document1 pageFdar 22-24 2Basema HashhashNo ratings yet
- BGH August 28 Oct1Document28 pagesBGH August 28 Oct1Basema HashhashNo ratings yet
- OR QuizDocument1 pageOR QuizBasema HashhashNo ratings yet
- Drug Study 1Document13 pagesDrug Study 1Basema HashhashNo ratings yet
- Journal-Of-18 MicuDocument1 pageJournal-Of-18 MicuBasema HashhashNo ratings yet
- JournalDocument32 pagesJournalBasema HashhashNo ratings yet
- HASHHASH, Journal CommunityDocument1 pageHASHHASH, Journal CommunityBasema HashhashNo ratings yet
- MidazolamDocument2 pagesMidazolamDesireemae Riosa-Candaroma100% (6)
- ED Nursing Management of Orthopedic FracturesDocument2 pagesED Nursing Management of Orthopedic FracturesBasema HashhashNo ratings yet
- Body Weakness NCPDocument1 pageBody Weakness NCPArnold Christian QuilonNo ratings yet
- Morphine pain relief side effectsDocument6 pagesMorphine pain relief side effectsBasema HashhashNo ratings yet
- NCP - BasemaDocument2 pagesNCP - BasemaBasema HashhashNo ratings yet
- Drug Study OmeprazoleDocument2 pagesDrug Study OmeprazoleGilianne Jimenea60% (5)
- NCP 1 HyperthermiaDocument3 pagesNCP 1 HyperthermiaBasema HashhashNo ratings yet
- Ncp-Potential-Fernandez Hashhash Navarro PaitDocument3 pagesNcp-Potential-Fernandez Hashhash Navarro PaitBasema HashhashNo ratings yet
- Med Ward JournalDocument2 pagesMed Ward JournalBasema HashhashNo ratings yet
- NCP Impaired Physical MobilityDocument6 pagesNCP Impaired Physical MobilityBasema HashhashNo ratings yet
- College Nursing Drug StudyDocument19 pagesCollege Nursing Drug StudyBasema HashhashNo ratings yet
- Journal Psych WardDocument2 pagesJournal Psych WardBasema HashhashNo ratings yet
- 100837-26 SentieroAdvanced SOH100360 April 2022 EN WebDocument12 pages100837-26 SentieroAdvanced SOH100360 April 2022 EN Webrodrigo rodriguez pachonNo ratings yet
- Medical Terminology: Thе Best Illustrated Guide for Health Care Students and Professionals to Learn and Improve Medical SkillsDocument200 pagesMedical Terminology: Thе Best Illustrated Guide for Health Care Students and Professionals to Learn and Improve Medical SkillsChristieBrownNo ratings yet
- 2nd Summative TestDocument4 pages2nd Summative TestMarie Antonette Aco BarbaNo ratings yet
- Brochogenic Cyst 2017.fullDocument5 pagesBrochogenic Cyst 2017.fullManok KumarNo ratings yet
- DCHDocument163 pagesDCHLuiza Radulescu100% (1)
- Medical Spa Embezzlement Employee Theft ScamsDocument40 pagesMedical Spa Embezzlement Employee Theft ScamsRamon MartuaNo ratings yet
- Haryana Review MARCH 2017Document60 pagesHaryana Review MARCH 2017Neeraj YadavNo ratings yet
- Акушерство Фукс англ 2019Document875 pagesАкушерство Фукс англ 2019ȜLaa AsHrafNo ratings yet
- 4th QTR ReportingDocument8 pages4th QTR ReportingMa. Liza Coralyn MundoNo ratings yet
- PhD Thesis AcknowledgementDocument3 pagesPhD Thesis AcknowledgementNeelamegam DevarasuNo ratings yet
- Notice 503943616Document2 pagesNotice 503943616abreu2021No ratings yet
- Safety of Topical Ibuprofen GelDocument1 pageSafety of Topical Ibuprofen GelNarongchai PongpanNo ratings yet
- Rapid Real-Time PCR for Diagnosing Tinea InfectionsDocument7 pagesRapid Real-Time PCR for Diagnosing Tinea InfectionsSiti Bellia Arafah XndNo ratings yet
- The Bonny Method of Guided Imagery and Music For Music Therapy Interns - A Survey of Effects On Professional and Personal GrowthDocument10 pagesThe Bonny Method of Guided Imagery and Music For Music Therapy Interns - A Survey of Effects On Professional and Personal GrowthJuan Luis Köstner MartinoNo ratings yet
- Addiction Treatment Center in HoustonDocument8 pagesAddiction Treatment Center in Houstonemma rebel100% (1)
- DMLCIIDocument2 pagesDMLCIIVu Tung LinhNo ratings yet
- MBC Maxwell Release 9-19-12Document2 pagesMBC Maxwell Release 9-19-12Sorin IordacheNo ratings yet
- Impact On LGBTQ IssuesDocument2 pagesImpact On LGBTQ IssuesAngel BirringNo ratings yet
- Hfi 360Document5 pagesHfi 360Emanuel John BangoNo ratings yet
- Multi-Disciplinary Vs Interprofessional EducationDocument25 pagesMulti-Disciplinary Vs Interprofessional EducationbruceNo ratings yet
- List of Herbs and PropertiesDocument21 pagesList of Herbs and PropertieswisnuNo ratings yet
- .Document544 pages.Bestiana SaraLiontina0% (1)
- Levels of Evidence Flow Chart Rev May 2019Document3 pagesLevels of Evidence Flow Chart Rev May 2019Karl RobleNo ratings yet
- Welcome To Lagos DocumentaryDocument6 pagesWelcome To Lagos DocumentaryDede SonntagNo ratings yet
- Muhs PHD PROCEDURE AND RULES GOVERNING AWARD OF Ph.D. DEGREE IN THE SUBJECTS OF HEALTH SCIENCESDocument124 pagesMuhs PHD PROCEDURE AND RULES GOVERNING AWARD OF Ph.D. DEGREE IN THE SUBJECTS OF HEALTH SCIENCESTruppti SononeNo ratings yet
- TMP 22091-The Scapegoat - LIGHT's HOUSE-1947787810Document6 pagesTMP 22091-The Scapegoat - LIGHT's HOUSE-1947787810fenamagNo ratings yet
- Chapter 2 General Conditions of ServiceDocument7 pagesChapter 2 General Conditions of ServiceAnand KrishnaNo ratings yet
- The Ugly Side of Beauty: Animals and CosmeticsDocument3 pagesThe Ugly Side of Beauty: Animals and CosmeticsGianpaolo TaroniNo ratings yet
- Noise PollutionDocument12 pagesNoise PollutionRosh SibalNo ratings yet
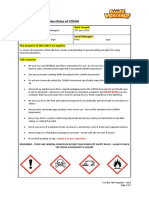
- 10 Golden COSHH RulesDocument2 pages10 Golden COSHH RulesKecskeméty BoriNo ratings yet