You might also like
- Peer CA Intrinsic Factors Kelompok 2Document21 pagesPeer CA Intrinsic Factors Kelompok 2Azik MubarakNo ratings yet
- Colbert Getz2013Document5 pagesColbert Getz2013NurrahmasiaNo ratings yet
- 3694 PDFDocument5 pages3694 PDFLouiseNo ratings yet
- Test Anxiety Gender and Academic Achievements PDFDocument6 pagesTest Anxiety Gender and Academic Achievements PDFNasir AhmadNo ratings yet
- 152-Article Text-996-5-10-20210329Document8 pages152-Article Text-996-5-10-20210329Ageng Catur WicaksonoNo ratings yet
- 224 412 1 SMDocument10 pages224 412 1 SMjanani a/p ayaooNo ratings yet
- Medical Education - 2002 - LievensDocument7 pagesMedical Education - 2002 - LievensziyshangNo ratings yet
- Performance of The Final Year Medical Students in Universiti Malaysia Sabah in The End Surgical Senior Posting (SSP) ExaminationDocument6 pagesPerformance of The Final Year Medical Students in Universiti Malaysia Sabah in The End Surgical Senior Posting (SSP) Examinationbalraj kaurNo ratings yet
- Multiple Rubric-Based Assessments of Student CaseDocument8 pagesMultiple Rubric-Based Assessments of Student CaseRehab weridaNo ratings yet
- Training Metacognition in The Classroom: The Influence of Incentives and Feedback On Exam PredictionsDocument12 pagesTraining Metacognition in The Classroom: The Influence of Incentives and Feedback On Exam PredictionsEduardo reyesNo ratings yet
- Self-Assessment or Self Deception? A Lack of Association Between Nursing Students' Self-Assessment and PerformanceDocument9 pagesSelf-Assessment or Self Deception? A Lack of Association Between Nursing Students' Self-Assessment and PerformancejangnoesaNo ratings yet
- Factors Associated With Medical Student Test Anxiety in Objective Structured Clinical Examinations: A Preliminary StudyDocument4 pagesFactors Associated With Medical Student Test Anxiety in Objective Structured Clinical Examinations: A Preliminary Studyrahmasia limaNo ratings yet
- tct0010 0399Document6 pagestct0010 0399chevalier176No ratings yet
- 8 03 Lin Y.MDocument6 pages8 03 Lin Y.MAnda SmarandaNo ratings yet
- BMATs Predictive Validity For Medical School Perf 230919 225056Document13 pagesBMATs Predictive Validity For Medical School Perf 230919 225056Thakoon TtsNo ratings yet
- Instrumento de Inteligencia EmocionalDocument5 pagesInstrumento de Inteligencia EmocionalMabel Zamora MarinNo ratings yet
- Roop Et Al Effect of Clinical TeachingDocument5 pagesRoop Et Al Effect of Clinical Teachingapi-264671444No ratings yet
- Use of Mini-Cex As An Effective ToolDocument4 pagesUse of Mini-Cex As An Effective ToolDr Mohan JoshiNo ratings yet
- SPSS FileDocument28 pagesSPSS Filehumna ahmedNo ratings yet
- Is There A Relationship Between Attending 24Document3 pagesIs There A Relationship Between Attending 24api-264671444No ratings yet
- Pharmacy Students' Perceptions of Assessment and Its Impact OnDocument9 pagesPharmacy Students' Perceptions of Assessment and Its Impact OnCarolina MoralesNo ratings yet
- Learning in PracticeDocument6 pagesLearning in PracticeanataeusNo ratings yet
- Benefiting From Clinical Experience TheDocument5 pagesBenefiting From Clinical Experience TheSarah Joy BorguetaNo ratings yet
- Self Confidence Foreign StudiesDocument5 pagesSelf Confidence Foreign Studiesjosekin75% (4)
- Adaptation and Stress For The First Year University StudentsDocument5 pagesAdaptation and Stress For The First Year University Studentsale_pisiqtzaNo ratings yet
- Ospe Article 1Document7 pagesOspe Article 1Tejas KulkarniNo ratings yet
- Predictive Validity of OSCEDocument8 pagesPredictive Validity of OSCEmagdy balahaNo ratings yet
- Nursing JournalsDocument4 pagesNursing JournalsSheij MarquezNo ratings yet
- JMPCR - Volume 5 - Issue 12 - Pages 1204-1216Document13 pagesJMPCR - Volume 5 - Issue 12 - Pages 1204-1216mani arasiNo ratings yet
- Research Proposal2Document9 pagesResearch Proposal2Veronica DadalNo ratings yet
- 6.debriefing As Formative Assessment Closing Performance Gaps in Medical EducationDocument9 pages6.debriefing As Formative Assessment Closing Performance Gaps in Medical EducationHerrero MiliNo ratings yet
- Correlating Self-Esteem and Academic OutcomeDocument5 pagesCorrelating Self-Esteem and Academic OutcomeMae BalacanaoNo ratings yet
- Self-Regulation and Research Writing Competencies of Senior High School StudentsDocument11 pagesSelf-Regulation and Research Writing Competencies of Senior High School StudentsPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Rabinowitz 1987Document5 pagesRabinowitz 1987Max ZuhaediNo ratings yet
- Educ 106 Module-3Document31 pagesEduc 106 Module-3Roderick Viloria MiloNo ratings yet
- Running Head: Reliability and Validity 1Document10 pagesRunning Head: Reliability and Validity 1Lomialagi TauiliiliNo ratings yet
- January 27, 2021: Textbook Reading Notes Taking Memory Test Preparation Concentration Time Management Age Sex Year LevelDocument4 pagesJanuary 27, 2021: Textbook Reading Notes Taking Memory Test Preparation Concentration Time Management Age Sex Year LevelDominic PolancosNo ratings yet
- Research Forum Abstracts: 68, No. 4s: October 2016 Annals of Emergency MedicineDocument1 pageResearch Forum Abstracts: 68, No. 4s: October 2016 Annals of Emergency Medicinetri1994No ratings yet
- 8 03 Lin Y.MDocument6 pages8 03 Lin Y.MJohnjohn MateoNo ratings yet
- Psychometric Properties of The Learning Approach Inventory A Confirmatory Factor AnalysisDocument11 pagesPsychometric Properties of The Learning Approach Inventory A Confirmatory Factor Analysisrik.paul.iimt2330No ratings yet
- Mastery CriteriaDocument8 pagesMastery Criteriaalexsandra.christNo ratings yet
- 10546-Article Text-30304-1-10-20180227Document12 pages10546-Article Text-30304-1-10-20180227Sheda BondNo ratings yet
- LU 4 Methods of Reliability Testing ConceptsDocument23 pagesLU 4 Methods of Reliability Testing ConceptsKristhel Jane Roxas NicdaoNo ratings yet
- Hartman: Bruce W. Dale FuquaDocument6 pagesHartman: Bruce W. Dale FuquaBich Thuy Tran PhungNo ratings yet
- The Utility of Letters of Recommendation in Predicting Resident Success: Can The ACGME Competencies Help?Document4 pagesThe Utility of Letters of Recommendation in Predicting Resident Success: Can The ACGME Competencies Help?UmaNo ratings yet
- Thesis Body Nursing ResearchDocument46 pagesThesis Body Nursing Researchwuxia1803No ratings yet
- Samuel Merritt University Nursing Program Pediatric Nursing Clinical EvaluationDocument14 pagesSamuel Merritt University Nursing Program Pediatric Nursing Clinical EvaluationSerbanNo ratings yet
- Medical Education Effect of Stress On Academic Performance in Medical Students - A Cross Sectional StudyDocument6 pagesMedical Education Effect of Stress On Academic Performance in Medical Students - A Cross Sectional Studyjamella.arbiol094No ratings yet
- Improving MetacognitionDocument21 pagesImproving MetacognitionJulie HolmesNo ratings yet
- Nihms 854664Document15 pagesNihms 854664ANo ratings yet
- Psychology (7th EdDocument8 pagesPsychology (7th EdgabbieNo ratings yet
- Test Anxiety and Academic Performance in Chiropractic StudentsDocument8 pagesTest Anxiety and Academic Performance in Chiropractic StudentsFranco Evale YumulNo ratings yet
- MODULE 3-Essential Measuring, Validation of Instruments and Suggestions in Writing Test.Document16 pagesMODULE 3-Essential Measuring, Validation of Instruments and Suggestions in Writing Test.Erika CulabanNo ratings yet
- M3 Group2Document5 pagesM3 Group2oroyan1920843No ratings yet
- Development of A Scale For Assessing Academic Stress: A Preliminary ReportDocument8 pagesDevelopment of A Scale For Assessing Academic Stress: A Preliminary ReportRenz Idelbert Subol0% (1)
- Characteristics of A Good Test: Validity and Reliability Criteria of Assessment and Rubric of ScoringDocument6 pagesCharacteristics of A Good Test: Validity and Reliability Criteria of Assessment and Rubric of Scoringyakub ismailNo ratings yet
- Self-Directed Learning Medical StudentsDocument4 pagesSelf-Directed Learning Medical StudentssooyoungNo ratings yet
- 8602 Assignment No 2Document24 pages8602 Assignment No 2Fatima YousafNo ratings yet
- Makalah Assesment and EvaluationDocument14 pagesMakalah Assesment and EvaluationAdil WarsitoNo ratings yet
- Playful Testing: Designing a Formative Assessment Game for Data ScienceFrom EverandPlayful Testing: Designing a Formative Assessment Game for Data ScienceNo ratings yet
- Potential Clinical and Economic Impact Of.6Document12 pagesPotential Clinical and Economic Impact Of.6Erza GenatrikaNo ratings yet
- R - Observational Study On Knowledge and EatingDocument8 pagesR - Observational Study On Knowledge and EatingErza GenatrikaNo ratings yet
- R - Assessment of Knowledge of Staff Nurses Regarding Aseptic Techniques at Selected HospitalDocument6 pagesR - Assessment of Knowledge of Staff Nurses Regarding Aseptic Techniques at Selected HospitalErza GenatrikaNo ratings yet
- R - The Relationship of Socio-Demographic Characteristics and KnowledgeDocument14 pagesR - The Relationship of Socio-Demographic Characteristics and KnowledgeErza GenatrikaNo ratings yet
- The Sociocultural Contribution To Learning Why Did My Students Fail To Learn Aseptic Non-Touch Technique Multidimensional Factors Involved Inmedical Students' Failure To Learn This SkillDocument14 pagesThe Sociocultural Contribution To Learning Why Did My Students Fail To Learn Aseptic Non-Touch Technique Multidimensional Factors Involved Inmedical Students' Failure To Learn This SkillErza GenatrikaNo ratings yet
- Thematic Analysis Sebagai Metode Menganalisa Data Untuk Penelitian KualitatifDocument9 pagesThematic Analysis Sebagai Metode Menganalisa Data Untuk Penelitian KualitatifGalih RespatiNo ratings yet
- GERIATRIDocument7 pagesGERIATRIErza GenatrikaNo ratings yet
- dc55 PDFDocument9 pagesdc55 PDFHelfina MaharaniNo ratings yet
- Low Dose Naltrexone (LDN)Document11 pagesLow Dose Naltrexone (LDN)Erza GenatrikaNo ratings yet
- Berita Terkini Penggunaan LDNDocument24 pagesBerita Terkini Penggunaan LDNdimbrutNo ratings yet
- R - Ratka - Dasar Kuesioner - The Effect of Prior Experience With Aseptic Techniques On Learning OutcomeDocument10 pagesR - Ratka - Dasar Kuesioner - The Effect of Prior Experience With Aseptic Techniques On Learning OutcomeErza GenatrikaNo ratings yet
- Guidelines For The Management of Community - Acquired Pneumonia in ChildrenDocument14 pagesGuidelines For The Management of Community - Acquired Pneumonia in ChildrenMohammad Izza Naufal FikriNo ratings yet
- Clinical Tials On LDNDocument11 pagesClinical Tials On LDNErza GenatrikaNo ratings yet
- IndikatorDocument200 pagesIndikatorErza GenatrikaNo ratings yet
- Patient Counseling by PharmacistDocument8 pagesPatient Counseling by Pharmacistnoname19191No ratings yet
- Current Clinical Strategies, Physicians' Drug Resource (2005) BM OCR 7.0-2.5Document107 pagesCurrent Clinical Strategies, Physicians' Drug Resource (2005) BM OCR 7.0-2.5Kamlesh SharmaNo ratings yet
- IFOSFAMIDEDocument4 pagesIFOSFAMIDEErza GenatrikaNo ratings yet
- Tamoxifen PDFDocument5 pagesTamoxifen PDFErza GenatrikaNo ratings yet
- ONDANSENTRONDocument2 pagesONDANSENTRONErza GenatrikaNo ratings yet
- Siklopospamide IvDocument5 pagesSiklopospamide IvErza GenatrikaNo ratings yet
- Staying Healty PDFDocument99 pagesStaying Healty PDFErza GenatrikaNo ratings yet
- Patient Guide PDFDocument4 pagesPatient Guide PDFErza GenatrikaNo ratings yet
- THIOGUANINEDocument3 pagesTHIOGUANINEErza GenatrikaNo ratings yet
- OCREOTIDEDocument4 pagesOCREOTIDEErza GenatrikaNo ratings yet
- IFOSFAMIDEDocument4 pagesIFOSFAMIDEErza GenatrikaNo ratings yet
- MTX It PDFDocument3 pagesMTX It PDFErza GenatrikaNo ratings yet
- VINCRISTINEDocument3 pagesVINCRISTINEErza GenatrikaNo ratings yet
- Vinblastin PDFDocument3 pagesVinblastin PDFErza GenatrikaNo ratings yet
- MERCAPTOPURINEDocument4 pagesMERCAPTOPURINEErza GenatrikaNo ratings yet
- Effect of The Bacteria On The Porosity and Permeability On Self Healing ConcreteDocument11 pagesEffect of The Bacteria On The Porosity and Permeability On Self Healing ConcreteChinmay DayNo ratings yet
- Keyop Functions 9F3715Document114 pagesKeyop Functions 9F3715Art MessickNo ratings yet
- Basic Calculus Module 4Document26 pagesBasic Calculus Module 4Settei Hainah AmpuanNo ratings yet
- LIS2sl - 0911 - en SIEMENS SLDocument456 pagesLIS2sl - 0911 - en SIEMENS SLAntonio VazquezNo ratings yet
- Lipid Analysis: Melisa Intan BarlianaDocument38 pagesLipid Analysis: Melisa Intan BarlianaChantique Maharani0% (1)
- Pen-Channel Flow: When You Finish Reading This Chapter, You Should Be Able ToDocument68 pagesPen-Channel Flow: When You Finish Reading This Chapter, You Should Be Able To李建道No ratings yet
- Fleishman AP 1975 - Towards A Taxonomy of Human PerformanceDocument23 pagesFleishman AP 1975 - Towards A Taxonomy of Human PerformanceCatalina Elena100% (2)
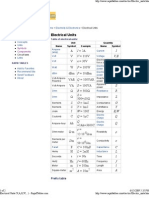
- Electrical UnitsDocument2 pagesElectrical Unitsevtoma100% (1)
- Department of Civil Engineering Lakshmi Narain College of Technology BHOPAL-462021 (INDIA)Document48 pagesDepartment of Civil Engineering Lakshmi Narain College of Technology BHOPAL-462021 (INDIA)Vikash SinghNo ratings yet
- 17.11.1501 - Andhy Panca SaputraDocument10 pages17.11.1501 - Andhy Panca SaputraRiyan pandusadewoNo ratings yet
- Design Characteristics and Development of A Nozzle For Coaxial Laser CladdingDocument10 pagesDesign Characteristics and Development of A Nozzle For Coaxial Laser CladdingEduardo MendezNo ratings yet
- Network Device Monitoring Report Templet-Dec, 08-2021Document3 pagesNetwork Device Monitoring Report Templet-Dec, 08-2021Habtamu AsaytoNo ratings yet
- Calculating Index Values and PerformanceDocument5 pagesCalculating Index Values and Performancemuneebmateen01No ratings yet
- Unit-1 (Cse 245)Document58 pagesUnit-1 (Cse 245)Harsh DubeyNo ratings yet
- Usp31nf26s1 - c731, General Chapters - 731 - LOSS ON DRYINGDocument1 pageUsp31nf26s1 - c731, General Chapters - 731 - LOSS ON DRYINGEfsha KhanNo ratings yet
- 6242 01 Rms 20060616Document10 pages6242 01 Rms 20060616UncleBulgariaNo ratings yet
- Quantum Optical Memory For Entanglement DistributionDocument22 pagesQuantum Optical Memory For Entanglement DistributionJay-R Notorio PallegaNo ratings yet
- 001-03 - Hydraulic Charge Pressure Switch Shorted To High SourceDocument6 pages001-03 - Hydraulic Charge Pressure Switch Shorted To High Sourceكؤمپيوته رى ديارىNo ratings yet
- Biochem Laboratory ReviewerDocument6 pagesBiochem Laboratory Reviewer202370092No ratings yet
- Adaptive-Fuzzy Logic Control of Robot Manipulators S. Commuri and F.L. LewisDocument6 pagesAdaptive-Fuzzy Logic Control of Robot Manipulators S. Commuri and F.L. LewisNguyễn Thanh TùngNo ratings yet
- Xenon LampDocument25 pagesXenon LampJamaica Peñaloza NatuelNo ratings yet
- Physical Science Module 3Document22 pagesPhysical Science Module 3Florence-j Pelayo Tupaz100% (1)
- Invariant and MonovariantDocument3 pagesInvariant and MonovariantQuốc ĐạtNo ratings yet
- Poster Presentation 3Document1 pagePoster Presentation 3Julien FaureNo ratings yet
- Module 1.MMWDocument20 pagesModule 1.MMWJimmy DegayNo ratings yet
- Introduction To IoT With Machine Learning and Image Processing Using Raspberry Pi (Shrirang Ambaji Kulkarni, Varadrah P. Gurupur Etc.) (Z-Library)Document167 pagesIntroduction To IoT With Machine Learning and Image Processing Using Raspberry Pi (Shrirang Ambaji Kulkarni, Varadrah P. Gurupur Etc.) (Z-Library)Siddhant RawatNo ratings yet
- The Mathematical Gazette Volume 86 Issue 507 2002 (Doi 10.2307 - 3621155) Nick Lord - 86.76 Maths Bite - Sides of Regular PolygonsDocument3 pagesThe Mathematical Gazette Volume 86 Issue 507 2002 (Doi 10.2307 - 3621155) Nick Lord - 86.76 Maths Bite - Sides of Regular PolygonsEduardo CostaNo ratings yet
- Ca 3241Document1 pageCa 3241Tien LamNo ratings yet
- Bioresource Technology: Oscar Pardo-Planas, Hasan K. Atiyeh, John R. Phillips, Clint P. Aichele, Sayeed MohammadDocument8 pagesBioresource Technology: Oscar Pardo-Planas, Hasan K. Atiyeh, John R. Phillips, Clint P. Aichele, Sayeed Mohammadmohsen ranjbarNo ratings yet
- BalancesDocument8 pagesBalancescchauling6841No ratings yet