You might also like
- Serial KillersDocument25 pagesSerial KillersCarrie Davis Dellinger100% (1)
- Diagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaFrom EverandDiagnosis and Treatment of Neurogenic Oropharyngeal DysphagiaNo ratings yet
- (START HERE) 7 Day Feminine Transformation WorkbookDocument37 pages(START HERE) 7 Day Feminine Transformation Workbookt6w5g27n4qNo ratings yet
- Mirko Workout PDFDocument10 pagesMirko Workout PDFSirine Boussama100% (3)
- Nursing Care of The Older Adult in Wellness: Geriatric Nursing AssessmentDocument36 pagesNursing Care of The Older Adult in Wellness: Geriatric Nursing AssessmentRuby Corazon Ediza100% (6)
- Cookery1-SPECIALIZED-FINAL 1Document37 pagesCookery1-SPECIALIZED-FINAL 1Princess Aira Malveda100% (1)
- Dysphagia: Diagnosis and Treatment: January 2006Document9 pagesDysphagia: Diagnosis and Treatment: January 2006Psicólogo José LuizNo ratings yet
- Criterios Para Avaliacao Clinica Fonoaudiologica dDocument12 pagesCriterios Para Avaliacao Clinica Fonoaudiologica dAngélica GarcíaNo ratings yet
- 01.consistencia Clínica TraqueoDocument12 pages01.consistencia Clínica TraqueoCarlonchaCáceresNo ratings yet
- Tracheostomy Management by Speech Language Pathologists in SwedenDocument12 pagesTracheostomy Management by Speech Language Pathologists in SwedenCamila Andrea Barrera BlancoNo ratings yet
- Ni Hms 905286Document16 pagesNi Hms 905286bellavalaniNo ratings yet
- jcm-12-03605-v2Document14 pagesjcm-12-03605-v2IgnacioCortésFuentesNo ratings yet
- 08.screening Pacientes Con TQTDocument11 pages08.screening Pacientes Con TQTCarlonchaCáceresNo ratings yet
- Dysphagic Patients With Tracheotomies: A Multidisciplinary Approach To Treatment and Decannulation ManagementDocument11 pagesDysphagic Patients With Tracheotomies: A Multidisciplinary Approach To Treatment and Decannulation ManagementleslieNo ratings yet
- A Systematic Review of Patient and Caregiver Experiences With A TracheostomyDocument17 pagesA Systematic Review of Patient and Caregiver Experiences With A TracheostomySelfi SeptianingsiNo ratings yet
- Airway Clearance. Physiology, Pharmacology, Techniques, and Practice - Rubin, Hess 2007Document5 pagesAirway Clearance. Physiology, Pharmacology, Techniques, and Practice - Rubin, Hess 2007Maxi BoniniNo ratings yet
- Rme Efek AnakDocument10 pagesRme Efek AnakSiwi HadjarNo ratings yet
- Primary Versus Secondary Tracheoesophageal Puncture: Systematic Review and Meta-AnalysisDocument8 pagesPrimary Versus Secondary Tracheoesophageal Puncture: Systematic Review and Meta-AnalysisIsrael BlancoNo ratings yet
- Laryngeal DysplasiaDocument7 pagesLaryngeal DysplasiakarimahihdaNo ratings yet
- How Long Does Treatment With Fixed Orthodontic Appliances Last? A Systematic ReviewDocument11 pagesHow Long Does Treatment With Fixed Orthodontic Appliances Last? A Systematic ReviewSrishti SyalNo ratings yet
- Daniels Defining Dysphagia Ajslp2009Document9 pagesDaniels Defining Dysphagia Ajslp2009Ignacio AndresNo ratings yet
- Treacher Collins Syndrome: A Systematic Review of Evidence-Based Treatment and RecommendationsDocument14 pagesTreacher Collins Syndrome: A Systematic Review of Evidence-Based Treatment and RecommendationsSai KrupaNo ratings yet
- European Society of Neurogastroenterology and Motility Guidelines On Functional Constipation in AdultsDocument33 pagesEuropean Society of Neurogastroenterology and Motility Guidelines On Functional Constipation in AdultsOuerdia HATEMNo ratings yet
- Bronquiectasias Nuevas TerapiasDocument12 pagesBronquiectasias Nuevas TerapiasJuan ZamoraNo ratings yet
- Loop Vs DividedDocument8 pagesLoop Vs DividedNatalindah Jokiem Woecandra T. D.No ratings yet
- Transdisciplinary Approaches Enhance The Production of Translational KnowledgeDocument12 pagesTransdisciplinary Approaches Enhance The Production of Translational KnowledgereneNo ratings yet
- Costa 2017Document10 pagesCosta 2017Karam EidNo ratings yet
- European ConstipationDocument33 pagesEuropean ConstipationambulatNo ratings yet
- HHS Public Access: Practice Patterns of Sedation For ColonosDocument18 pagesHHS Public Access: Practice Patterns of Sedation For ColonosIulia CampanuNo ratings yet
- SepDocument7 pagesSepyuyuNo ratings yet
- Airway Clearance Physiology Pharmacology Techniques and Practice PDFDocument5 pagesAirway Clearance Physiology Pharmacology Techniques and Practice PDFPaoly PalmaNo ratings yet
- Septum Deviasi PDFDocument9 pagesSeptum Deviasi PDFErick DjuandaNo ratings yet
- Effectiveness of Myofunctional Therapy in Ankyloglossia: A Systematic ReviewDocument18 pagesEffectiveness of Myofunctional Therapy in Ankyloglossia: A Systematic Reviewmistic0No ratings yet
- Brachytherapy For The Palliation of Dysphagia Owing To Esop - 2017 - RadiotherapDocument8 pagesBrachytherapy For The Palliation of Dysphagia Owing To Esop - 2017 - RadiotherapFlorin AchimNo ratings yet
- Skoretz2020 Article ASystematicReviewOfTracheostomDocument13 pagesSkoretz2020 Article ASystematicReviewOfTracheostomDr. Huerta TorresNo ratings yet
- 2020 Pediatric Tracheostomy Decannulation Post Implementation of TQT Team and Decannulation ProtocolDocument9 pages2020 Pediatric Tracheostomy Decannulation Post Implementation of TQT Team and Decannulation ProtocolDavid Fabián Fernández CarmonaNo ratings yet
- Efeitos Da Frenotomia Lingual No Aleitamento Materno 2022Document6 pagesEfeitos Da Frenotomia Lingual No Aleitamento Materno 2022Paulina SandovalNo ratings yet
- 10 1016@j Ijporl 2020 110139Document28 pages10 1016@j Ijporl 2020 110139Gregoria choque floresNo ratings yet
- An Overview of Randomized Control Trials in OrthodonticsDocument10 pagesAn Overview of Randomized Control Trials in OrthodonticsHARITHA H.PNo ratings yet
- Complete Denture Occlusion An Evidence-Based ApproachDocument5 pagesComplete Denture Occlusion An Evidence-Based ApproachScribeNo ratings yet
- Journal Pone 0291803Document7 pagesJournal Pone 0291803Javiera BelenNo ratings yet
- Chan 2014Document6 pagesChan 2014canndy202No ratings yet
- Baumann 2001Document13 pagesBaumann 2001Dewi PutriNo ratings yet
- 1 s2.0 S0020748920302996 MainDocument13 pages1 s2.0 S0020748920302996 MainSri purwantiNo ratings yet
- 2018prospective Instrumental Evaluation of Swallowing Tongue Function and QOL Measures Following Transoral Robotic Surgery Alone Without Adjuvant Therapy - CompressedDocument7 pages2018prospective Instrumental Evaluation of Swallowing Tongue Function and QOL Measures Following Transoral Robotic Surgery Alone Without Adjuvant Therapy - CompressedYolanda Gómez LópezNo ratings yet
- 1 BernardesDocument14 pages1 Bernardescesia llancaoNo ratings yet
- Irrigantes IntracanalDocument14 pagesIrrigantes Intracanaljhon valdiviezoNo ratings yet
- The Surgical Management of Necrotizing Enterocolitis - July 2018Document4 pagesThe Surgical Management of Necrotizing Enterocolitis - July 2018Hengky TanNo ratings yet
- 10 1111@ans 15125Document7 pages10 1111@ans 15125Sahily MoralesNo ratings yet
- 10.1007@s00405 016 4015 4Document10 pages10.1007@s00405 016 4015 4Lorena PaulaNo ratings yet
- Defining and Measuring Dysphagia Following StrokeDocument8 pagesDefining and Measuring Dysphagia Following StrokeKerrie O' GradyNo ratings yet
- Weller 2010Document9 pagesWeller 2010brboyNo ratings yet
- Concepts, Controversies, 9-12 PDFDocument4 pagesConcepts, Controversies, 9-12 PDFSrivani PeriNo ratings yet
- Respirador BucalDocument8 pagesRespirador Bucalyessenia armijosNo ratings yet
- Transcutaneous Electrical Nerve Stimulation in Speech Therapy Rehabilitation ofDocument13 pagesTranscutaneous Electrical Nerve Stimulation in Speech Therapy Rehabilitation ofGabriel DefazNo ratings yet
- Pediatric Hydrocephalus: Systematic Literature Review and Evidence-Based Guidelines. Part 1: Introduction and MethodologyDocument5 pagesPediatric Hydrocephalus: Systematic Literature Review and Evidence-Based Guidelines. Part 1: Introduction and MethodologyagusNo ratings yet
- Colorectal Disease - 2021 - Christensen - Management Guidelines For Low Anterior Resection Syndrome The MANUEL ProjectDocument15 pagesColorectal Disease - 2021 - Christensen - Management Guidelines For Low Anterior Resection Syndrome The MANUEL ProjectRicardo QuinteiroNo ratings yet
- Meta 2 - Sofi AA - 2018Document9 pagesMeta 2 - Sofi AA - 2018matheus.verasNo ratings yet
- Clinical Practice Guideline CKDDocument66 pagesClinical Practice Guideline CKDjenna1213No ratings yet
- The Efficacy of Tracheostomy Tube Changes by Speech-Language Pathologists - A Retrospective ReviewDocument8 pagesThe Efficacy of Tracheostomy Tube Changes by Speech-Language Pathologists - A Retrospective ReviewÁnyela H. Merchán MendozaNo ratings yet
- Percutaneous Needle Aspiration Versus Catheter Drainage in Treating Hepatic AbscessDocument8 pagesPercutaneous Needle Aspiration Versus Catheter Drainage in Treating Hepatic AbscessRatna TriasnawatiNo ratings yet
- Dinis_Rhinology98_Psychosocial consequences of nasal aesthetic and functional surgeryDocument6 pagesDinis_Rhinology98_Psychosocial consequences of nasal aesthetic and functional surgeryallen.515No ratings yet
- Manejo de La Tos CronicaDocument6 pagesManejo de La Tos CronicaThomasMáximoMancinelliRinaldoNo ratings yet
- Da Cunha Pereira 2017Document7 pagesDa Cunha Pereira 2017Pablo Andrés Sánchez MonsalveNo ratings yet
- Efectos de La Terapia en Disfonia Musculotensional.2017Document7 pagesEfectos de La Terapia en Disfonia Musculotensional.2017Jenith Karem Paredes GonzalezNo ratings yet
- Module 2Document43 pagesModule 2jbg060595No ratings yet
- Semi-Detailed Lesson Plan in T.L.E FoodsDocument3 pagesSemi-Detailed Lesson Plan in T.L.E Foodsgracelyn riveraNo ratings yet
- The Nursing Process OverviewDocument26 pagesThe Nursing Process OverviewAYO NELSONNo ratings yet
- Johnson 2020 IOP Conf. Ser. Mater. Sci. Eng. 993 012022Document13 pagesJohnson 2020 IOP Conf. Ser. Mater. Sci. Eng. 993 012022astrid abigail blas sanchezNo ratings yet
- London International Model United Nations: Study Guide: UN Women CommitteeDocument40 pagesLondon International Model United Nations: Study Guide: UN Women CommitteeSarah SidaurukNo ratings yet
- The Movie "PK" AnalysisDocument2 pagesThe Movie "PK" AnalysisKerstmis “Scale” NataliaNo ratings yet
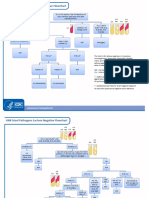
- GNR Stool Pathogens Lactose Negative FlowchartDocument2 pagesGNR Stool Pathogens Lactose Negative FlowchartKeithNo ratings yet
- Legalize ItDocument2 pagesLegalize Itaisar aisarNo ratings yet
- Mapeh 10 QuizDocument1 pageMapeh 10 QuizMichelle Dela RosaNo ratings yet
- SR No. District Name Address Contact NoDocument3 pagesSR No. District Name Address Contact Nochirag sabhayaNo ratings yet
- De-Escalation - Aggression Management TechniquesDocument14 pagesDe-Escalation - Aggression Management Techniquesparis emmaNo ratings yet
- Glucosamine PDFDocument6 pagesGlucosamine PDFChrist FarandyNo ratings yet
- Recruitment MSCDocument40 pagesRecruitment MSCViji MNo ratings yet
- ANA MAPEH S2017 Ans KeyDocument15 pagesANA MAPEH S2017 Ans KeyVan Errl Nicolai SantosNo ratings yet
- Declaration of James Sheldon2318Document7 pagesDeclaration of James Sheldon2318James Sheldon Jr.No ratings yet
- Physical Education and Health 2 - Grade 11 NotesDocument6 pagesPhysical Education and Health 2 - Grade 11 NotesPedro HampaslupaNo ratings yet
- Opscom AugustDocument19 pagesOpscom AugustMichelle Motin ToledoNo ratings yet
- ArmourDocument5 pagesArmourBiju_PottayilNo ratings yet
- Effects of A Capacitive-Resistive Electric Transfer Therapy OnDocument8 pagesEffects of A Capacitive-Resistive Electric Transfer Therapy OnAnna Lygia LunardiNo ratings yet
- Hospital departments, medical terms, and anatomyDocument18 pagesHospital departments, medical terms, and anatomyThanh ToànNo ratings yet
- UCT Postgraduate-Studies BrochureDocument27 pagesUCT Postgraduate-Studies BrochureUsman AhmedNo ratings yet
- Noncompliance Unilateral Maxillary Molar DistalizationDocument6 pagesNoncompliance Unilateral Maxillary Molar Distalizationaa bbNo ratings yet
- List of Allianz Efu Network (Panel) Hospitals: Hospital Name Address Telephone # KarachiDocument6 pagesList of Allianz Efu Network (Panel) Hospitals: Hospital Name Address Telephone # KarachiFaizan BasitNo ratings yet
- Aaron Choco de Guzman - BOSH LA 1Document3 pagesAaron Choco de Guzman - BOSH LA 1Aaron Choco De GuzmanNo ratings yet
- Nursing Leadership Roles ResponsibilitiesDocument2 pagesNursing Leadership Roles ResponsibilitiesDan Dan ManaoisNo ratings yet