You might also like
- Detecting Diagnostic Error in Psychiatry: James PhillipsDocument4 pagesDetecting Diagnostic Error in Psychiatry: James PhillipsVilma HernandezNo ratings yet
- A Universal Model of Diagnostic Reasoning.14Document7 pagesA Universal Model of Diagnostic Reasoning.14Emília SantocheNo ratings yet
- Centre For Addiction Mental Health - SkinnerDocument8 pagesCentre For Addiction Mental Health - SkinnerAmelia NewtonNo ratings yet
- Cognitive DebiasingDocument7 pagesCognitive DebiasingJefferson ChavesNo ratings yet
- Clinical Decision Making-The Danger of Confirmation Bias: EditorialDocument3 pagesClinical Decision Making-The Danger of Confirmation Bias: EditorialRachmat_Chusnu_6072No ratings yet
- Evidence-Based Treatment in The Field of Child andDocument2 pagesEvidence-Based Treatment in The Field of Child andRayén F. HuenchunaoNo ratings yet
- Chapter 5Document42 pagesChapter 5peachypeachyNo ratings yet
- Filipino Family Physician 2022 60 Pages 23 29Document7 pagesFilipino Family Physician 2022 60 Pages 23 29Pia PalaciosNo ratings yet
- 2019 - NATURE - Recommendations and Future Directions For Supervised Machine Learning in PsychiatryDocument12 pages2019 - NATURE - Recommendations and Future Directions For Supervised Machine Learning in PsychiatryPriya KumariNo ratings yet
- McEvoy 2015 MCT Group For GADDocument9 pagesMcEvoy 2015 MCT Group For GADmarggiNo ratings yet
- Description of The Patient & Instructions To SimulatorDocument9 pagesDescription of The Patient & Instructions To SimulatorsarfirazNo ratings yet
- Introduction To Psychological Assessment and PsychodiagnosisDocument75 pagesIntroduction To Psychological Assessment and PsychodiagnosisNishesh AcharyaNo ratings yet
- Patient Instructions: Name of Patient: MR Lur PakDocument7 pagesPatient Instructions: Name of Patient: MR Lur PaksarfirazNo ratings yet
- Running Head: Complete Psychiatric Examination On An Adult Patient 1Document5 pagesRunning Head: Complete Psychiatric Examination On An Adult Patient 1Sharon DikirrNo ratings yet
- 2017 Embracing Uncertainty To Advance Diagnosis inDocument2 pages2017 Embracing Uncertainty To Advance Diagnosis inpainfree888No ratings yet
- Psychological Assessment in Different Setting - PsychologicalDocument7 pagesPsychological Assessment in Different Setting - PsychologicalKian LaNo ratings yet
- Effective Psychological Interventions For RelapseDocument2 pagesEffective Psychological Interventions For RelapseRicardo EscNo ratings yet
- Introduction To Special Section On Pseudoscience in PsychiatryDocument3 pagesIntroduction To Special Section On Pseudoscience in PsychiatrysashasalinyNo ratings yet
- Pertemuan 7 - Clinical Assessment and DiagnosisDocument25 pagesPertemuan 7 - Clinical Assessment and DiagnosisRullita Aristya MNo ratings yet
- Clinical Vs Actuarial Judgment Original ArticleDocument7 pagesClinical Vs Actuarial Judgment Original ArticlepaengerzieNo ratings yet
- 2011 Detection of Depression and Anxiety Disorders in Primary Care Friendly)Document9 pages2011 Detection of Depression and Anxiety Disorders in Primary Care Friendly)rocksurNo ratings yet
- Personalized Psychiatry: Many Questions, Fewer Answers: EditorialDocument3 pagesPersonalized Psychiatry: Many Questions, Fewer Answers: EditorialJeronim H'gharNo ratings yet
- Clinical Versus Actuarial Judgment: Methods of Judgment and Means of ComparisonDocument19 pagesClinical Versus Actuarial Judgment: Methods of Judgment and Means of ComparisonanguschandlerNo ratings yet
- Clinical Interview and ObservationDocument47 pagesClinical Interview and Observationmlssmnn100% (1)
- The Clinical Characterization of The Adult Patient With Depression Aimed at Personalization of ManagementDocument25 pagesThe Clinical Characterization of The Adult Patient With Depression Aimed at Personalization of ManagementDavidNo ratings yet
- A 7 Minute Neurocognitive Screening Battery Highly Sensitive To Alzheimer's DiseaseDocument7 pagesA 7 Minute Neurocognitive Screening Battery Highly Sensitive To Alzheimer's DiseaseRealidades InfinitasNo ratings yet
- TDAH AdultosDocument5 pagesTDAH AdultosIsaac Daniel Carrero RoseroNo ratings yet
- DiagnosticDocument22 pagesDiagnosticBudi RahardjoNo ratings yet
- Kuhn 2016Document8 pagesKuhn 2016gabrielaNo ratings yet
- 10 1080@13854046 2019 1696409Document35 pages10 1080@13854046 2019 1696409AnaArantesNo ratings yet
- Martino, D. (2023) - Treatment Failure in Persisten Tic Disorders...Document15 pagesMartino, D. (2023) - Treatment Failure in Persisten Tic Disorders...cuautzinNo ratings yet
- Van Scoyoc, S. (2017) - The Use and Misuse of Psychometrics in Clinical Settings. in B. Cripps (Ed.)Document17 pagesVan Scoyoc, S. (2017) - The Use and Misuse of Psychometrics in Clinical Settings. in B. Cripps (Ed.)susanvanscoyoc9870No ratings yet
- 34test To Diagnose Attention Deficit Disorder (Add), Prevalence and Risk FactorsDocument9 pages34test To Diagnose Attention Deficit Disorder (Add), Prevalence and Risk FactorsIJAR JOURNALNo ratings yet
- Diagnosis and AssessmentDocument10 pagesDiagnosis and AssessmentcynthiasenNo ratings yet
- Schizophr Bull 2009 Carpenter 841 3Document3 pagesSchizophr Bull 2009 Carpenter 841 3András SzabóNo ratings yet
- Enseñanza AnestesioDocument14 pagesEnseñanza AnestesioRaúl MartínezNo ratings yet
- Psychology Assessment - I - M2Document53 pagesPsychology Assessment - I - M2Brinda ChughNo ratings yet
- Neuropsychological Assessment: Principles, Pearls and PerilsDocument8 pagesNeuropsychological Assessment: Principles, Pearls and Perilsnellianeth orozco garciaNo ratings yet
- A Systematic Scoping Review of Psychological Therapies For Psychosis Within Acute Psychiatric In-Patient Settings.Document8 pagesA Systematic Scoping Review of Psychological Therapies For Psychosis Within Acute Psychiatric In-Patient Settings.Eric KatškovskiNo ratings yet
- Genetic Evaluation ReferalsDocument6 pagesGenetic Evaluation Referalsviviana84No ratings yet
- The Prevalence of Depression and The Accuracy of Depression Screening Tools in Migraine PatientsDocument7 pagesThe Prevalence of Depression and The Accuracy of Depression Screening Tools in Migraine PatientsAnonymous PS9efzoNo ratings yet
- Ease of Screening For Depression and DeliriumDocument6 pagesEase of Screening For Depression and DeliriumThaísa NogueiraNo ratings yet
- Consultation - Liaison Psychiatry: Prof. Dr. Dr. M Syamsulhadi, SPKJ (K)Document46 pagesConsultation - Liaison Psychiatry: Prof. Dr. Dr. M Syamsulhadi, SPKJ (K)Sani Widya FirnandaNo ratings yet
- Unit 2 Different Stages in Psychodiagnostics: RuctureDocument16 pagesUnit 2 Different Stages in Psychodiagnostics: RuctureZainab100% (1)
- Articulo 14Document3 pagesArticulo 14Vilma HernandezNo ratings yet
- Behavioral Management Guide: Essential Treatment Strategies for Adult PsychotherapyFrom EverandBehavioral Management Guide: Essential Treatment Strategies for Adult PsychotherapyNo ratings yet
- Goodman D2010 The Black Bookof ADHDDocument19 pagesGoodman D2010 The Black Bookof ADHDRadja Er GaniNo ratings yet
- Clinical Assessment Psychodiagnostic Decision MakingDocument158 pagesClinical Assessment Psychodiagnostic Decision MakingKilana LichterfeldNo ratings yet
- 2012 Article 2129Document9 pages2012 Article 2129RodrigoSachiFreitasNo ratings yet
- Who Is Suitable For Cognitive Behavioural TherapyDocument8 pagesWho Is Suitable For Cognitive Behavioural TherapyPentheus214No ratings yet
- Qualitative Method VS Quantitative MethodDocument9 pagesQualitative Method VS Quantitative Methodreyhanehhosseiny2000No ratings yet
- Psychiatric Evaluation of The Agitated Patient - Consensus Statement of The American Association For Emergency Psychiatry Project BETA Psychiatric Evaluation Workgroup - PMCDocument9 pagesPsychiatric Evaluation of The Agitated Patient - Consensus Statement of The American Association For Emergency Psychiatry Project BETA Psychiatric Evaluation Workgroup - PMCKaren C. ManoodNo ratings yet
- Effectiveness of Counselling To Increase The Family of Soul Patients About Drug ComplianceDocument4 pagesEffectiveness of Counselling To Increase The Family of Soul Patients About Drug ComplianceMarlisa LionoNo ratings yet
- Decision Making in General PracticeDocument3 pagesDecision Making in General Practiceأحمد خيري التميميNo ratings yet
- Feighner Et Al (1972) - Diagnostic Criteria For Use in Psychiatric ResearchDocument7 pagesFeighner Et Al (1972) - Diagnostic Criteria For Use in Psychiatric ResearchEmily RedmanNo ratings yet
- Counselling Approaches in Office SettingsDocument8 pagesCounselling Approaches in Office SettingsDrAmeen1976No ratings yet
- Depression and TelepsychiatryDocument6 pagesDepression and TelepsychiatryMaria Von ShaftNo ratings yet
- Diffrential DiagnosisDocument8 pagesDiffrential DiagnosisArya AgrahariNo ratings yet
- Audit of Mental Capacity Assessment by Primary Care Physicians Versus Consultation-Liaison PsychiatristsDocument7 pagesAudit of Mental Capacity Assessment by Primary Care Physicians Versus Consultation-Liaison PsychiatristsmelissaNo ratings yet
- Branch Cashier-Sec Evaluation FormDocument7 pagesBranch Cashier-Sec Evaluation FormAling Kinai100% (1)
- Sri Sai Institute of Technology and Science/s. Asfiya 18f71e0005/traning & Development Big Bazaar/05Document8 pagesSri Sai Institute of Technology and Science/s. Asfiya 18f71e0005/traning & Development Big Bazaar/05Inthiyaz KothapalleNo ratings yet
- Mental and Emotional Manipulation Secrets of Persuasion For Professional and Personal SuccessDocument30 pagesMental and Emotional Manipulation Secrets of Persuasion For Professional and Personal Successwalter self publishingNo ratings yet
- C1 Advanced Writing Part 1: Teacher's NotesDocument8 pagesC1 Advanced Writing Part 1: Teacher's NotesOlha Sen'kivNo ratings yet
- Bailey Et Al. 2016. Using A Narrative Approach To Understand Place AttachmentsDocument12 pagesBailey Et Al. 2016. Using A Narrative Approach To Understand Place AttachmentsNatalia MolinaNo ratings yet
- 2021 (July) Practical Training Rating SheetDocument1 page2021 (July) Practical Training Rating SheetRitik agarwalNo ratings yet
- 1 Performance Output: 80% 81-87% 88-94% 95-100% Points Subject Knowledge and Coverage OrganizationDocument4 pages1 Performance Output: 80% 81-87% 88-94% 95-100% Points Subject Knowledge and Coverage OrganizationJuvelyn SajoniaNo ratings yet
- Desmos House Graphic CalculatorDocument8 pagesDesmos House Graphic CalculatorNayel SeghrouchniNo ratings yet
- Descriptive Essay Rubric 1 1Document2 pagesDescriptive Essay Rubric 1 1api-642177053No ratings yet
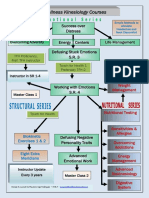
- Wellness Kinesiology Courses: Success Over Distress S.R. 1 & 2Document1 pageWellness Kinesiology Courses: Success Over Distress S.R. 1 & 2Naomi MarieNo ratings yet
- Developing VirtueDocument26 pagesDeveloping VirtueTulungan Para sa Modular at Online ClassesNo ratings yet
- MPeskin Leadership EssayDocument8 pagesMPeskin Leadership EssayMax PeskinNo ratings yet
- Ge 211 Student Enter Exit Survey 372 BlueDocument1 pageGe 211 Student Enter Exit Survey 372 BlueDanialNo ratings yet
- 6 Facets of UnderstandingDocument1 page6 Facets of UnderstandingEmmi M. RoldanNo ratings yet
- Module 1 Cog PsyDocument39 pagesModule 1 Cog PsySandra LacanariaNo ratings yet
- Grade9 Week2 Arts DLL FormatDocument1 pageGrade9 Week2 Arts DLL FormatRod ManNo ratings yet
- Research Methods: CausalityDocument17 pagesResearch Methods: CausalityBeytullah ErdoğanNo ratings yet
- Mat Rempit EditedDocument21 pagesMat Rempit Editedadle_267% (3)
- Behavioral Interviewing: More Than A Gut FeelingDocument31 pagesBehavioral Interviewing: More Than A Gut FeelingSuharto, S. Pd., M.T. PSPNo ratings yet
- CNF 4th Q First Activity LessonDocument4 pagesCNF 4th Q First Activity LessonDarwin CortunaNo ratings yet
- Mba International Business Project ReportDocument17 pagesMba International Business Project Reportgscentury2769370% (2)
- Two LinersDocument2 pagesTwo LinersjoinsyedNo ratings yet
- JLL Coworking Trends ReportDocument12 pagesJLL Coworking Trends ReportKunal dalviNo ratings yet
- Grading and ReportingDocument35 pagesGrading and ReportingJean Laurel75% (4)
- Do You Truly Know Yourself?: Activity # 1Document3 pagesDo You Truly Know Yourself?: Activity # 1ladygangster08No ratings yet
- Ministry of Health and Social WelfareDocument21 pagesMinistry of Health and Social WelfareNicole TaylorNo ratings yet
- Genesis Training ExercisesDocument6 pagesGenesis Training ExercisesdwerylNo ratings yet
- Tung Similarity-Preserving Knowledge Distillation ICCV 2019 PaperDocument10 pagesTung Similarity-Preserving Knowledge Distillation ICCV 2019 Paperraniahamizi006No ratings yet
- Infants and ToddlersDocument14 pagesInfants and ToddlersJosias Smith100% (1)
- Efficacy of Attachment-Based Family Therapy Compared To Treatment As Usual For Suicidal Ideation in Adolescents With MDDDocument11 pagesEfficacy of Attachment-Based Family Therapy Compared To Treatment As Usual For Suicidal Ideation in Adolescents With MDDGabriela MoralesNo ratings yet