You might also like
- Endometriosis (Complete)Document71 pagesEndometriosis (Complete)Justin Ng SincoNo ratings yet
- Necrotizing Fasciitis, (Flesh Eating Disease) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandNecrotizing Fasciitis, (Flesh Eating Disease) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
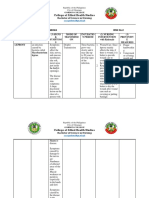
- Ii. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Document4 pagesIi. NCP: Black, Et - Al. (2005) .Me Dical Surgical Nursing. 7 Edition - Elsevie R Pte LTD.P 927Lecery Sophia Wong75% (4)
- Value of Observations in Homoeopathic PracticeDocument6 pagesValue of Observations in Homoeopathic PracticeHomoeopathic Pulse100% (2)
- Table of Communicable Diseases PDFDocument12 pagesTable of Communicable Diseases PDFkayekristine2001No ratings yet
- 6 Diabetic FootDocument28 pages6 Diabetic FootPraneetha NouduriNo ratings yet
- Gallstone Pancreatitis - CST PDFDocument5 pagesGallstone Pancreatitis - CST PDFDaniel Rosero CadenaNo ratings yet
- Interference Fields: in Healing Chronic IllnessDocument7 pagesInterference Fields: in Healing Chronic IllnessPoorni ShivaramNo ratings yet
- PEDIA - Drug Study & NCPDocument24 pagesPEDIA - Drug Study & NCPCzarina Mae Lomboy100% (1)
- DRUG STUDY - MetronidazoleDocument1 pageDRUG STUDY - MetronidazoleKristine AsuncionNo ratings yet
- Empowering Young Women For Community Development ProposalDocument13 pagesEmpowering Young Women For Community Development ProposalSana MahmoodNo ratings yet
- Opath Lab. Pulp Periapical Diseases CompleteDocument3 pagesOpath Lab. Pulp Periapical Diseases CompleteJaira LaguidaoNo ratings yet
- Endodontic Emergency (Dr. Imran)Document2 pagesEndodontic Emergency (Dr. Imran)aelessyaNo ratings yet
- Disabilties and Deformities in Leprosy Seminar14!4!2017Document21 pagesDisabilties and Deformities in Leprosy Seminar14!4!2017Rohit GuptaNo ratings yet
- Terrorism Information ChartDocument15 pagesTerrorism Information ChartAsad Imran100% (1)
- NCP 1Document2 pagesNCP 1SienaNo ratings yet
- Monkeypox Atlas With Some Differential Diagnosis: Aids Healthcare FoundationDocument20 pagesMonkeypox Atlas With Some Differential Diagnosis: Aids Healthcare FoundationCaio LimaNo ratings yet
- Clinical: Management of Frey Syndrome Using Botulinum Neurotoxin: A Case ReportDocument4 pagesClinical: Management of Frey Syndrome Using Botulinum Neurotoxin: A Case Reportaulia nurNo ratings yet
- Ulcer DiabeticsDocument3 pagesUlcer DiabeticsHaeruddinHasyimPasingariNo ratings yet
- Acute Unilateral Facial Nerve Palsy: Case StudyDocument3 pagesAcute Unilateral Facial Nerve Palsy: Case StudyPutri Zeahan Ramadhini YedismanNo ratings yet
- Latina 2010 04 MistakenIdentityDocument2 pagesLatina 2010 04 MistakenIdentityDorkys RamosNo ratings yet
- Vulva Scientific PaperDocument4 pagesVulva Scientific PaperChibiNo ratings yet
- Medicine and SurgeryDocument25 pagesMedicine and SurgerysripriyakrishnaNo ratings yet
- Recognition and Interpretation of Skin 1Document6 pagesRecognition and Interpretation of Skin 1Veterinarios de ArgentinaNo ratings yet
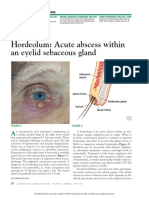
- Hordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureDocument3 pagesHordeolum: Acute Abscess Within An Eyelid Sebaceous Gland: The Clinical PictureCamNo ratings yet
- Concept Map Leukemia PDFDocument7 pagesConcept Map Leukemia PDFDiane AbanillaNo ratings yet
- Concept Map Leukemia PDFDocument7 pagesConcept Map Leukemia PDFMichael AmandyNo ratings yet
- Osce Special Sense LuminanceDocument3 pagesOsce Special Sense Luminancehajidah hassanalNo ratings yet
- Musculoskeletal Assessment Assessment Subjective:-: Behaviour of Pain SuggestionsDocument20 pagesMusculoskeletal Assessment Assessment Subjective:-: Behaviour of Pain SuggestionsFatima JamalNo ratings yet
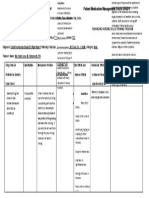
- Patient 1 Drug Study 1Document1 pagePatient 1 Drug Study 1Memcom SolutionNo ratings yet
- Derm Pathology PDFDocument21 pagesDerm Pathology PDFMara MitrutNo ratings yet
- McAlinden Hordeolum PDFDocument3 pagesMcAlinden Hordeolum PDFNur Rakhma AkmaliaNo ratings yet
- Gyne - Case 11 Lower Genital UTI PDFDocument2 pagesGyne - Case 11 Lower Genital UTI PDFcbac1990No ratings yet
- Itchy Eyes Case Study: Eye Series - 17Document2 pagesItchy Eyes Case Study: Eye Series - 17nicoNo ratings yet
- The Acute Painful Red Eye: History of Presenting Complaint - The Time and Speed of OnsetDocument4 pagesThe Acute Painful Red Eye: History of Presenting Complaint - The Time and Speed of Onsetleigh_zaliNo ratings yet
- Ears Day 1Document3 pagesEars Day 1Rue Cheng MaNo ratings yet
- Group 2 - Case Study of Mrs. Miller 1 Y2 8Document17 pagesGroup 2 - Case Study of Mrs. Miller 1 Y2 8Chesca DomingoNo ratings yet
- PainDocument93 pagesPainAurthi ElamparithiNo ratings yet
- Acupuncture For Carpal Tunnel Syndrome: Jonathan FreedmanDocument3 pagesAcupuncture For Carpal Tunnel Syndrome: Jonathan FreedmanGENIONo ratings yet
- Nursing Care Plan Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationDocument7 pagesNursing Care Plan Nursing Diagnosis Analysis Goal Intervention Rationale EvaluationHanz Abbigail Roco100% (1)
- Differential Diagnosis: Aureus Is The CommonestDocument5 pagesDifferential Diagnosis: Aureus Is The CommonestHestia Nur AnnisaNo ratings yet
- The Differential of Chronic Ulcer of The Leg: DiagnosisDocument8 pagesThe Differential of Chronic Ulcer of The Leg: DiagnosisJulioNo ratings yet
- Herpes Z Oster Clinical PresentationDocument50 pagesHerpes Z Oster Clinical PresentationS KkNo ratings yet
- Alinsangao, Nashwa N. BSN 3B - SIC (Pathogenesis & Life Threatening Pathways)Document5 pagesAlinsangao, Nashwa N. BSN 3B - SIC (Pathogenesis & Life Threatening Pathways)NASHWA NASLUN. ALINSANGAONo ratings yet
- AnnexIII DifferentialDiagnosis FromNLEP India PDFDocument3 pagesAnnexIII DifferentialDiagnosis FromNLEP India PDFAegirine RafilahNo ratings yet
- Emailing 50 - Examination of Joints - FinalDocument6 pagesEmailing 50 - Examination of Joints - FinalProsenjit BhowalNo ratings yet
- The Case of The Recurrent Chalazion: Morning RoundsDocument2 pagesThe Case of The Recurrent Chalazion: Morning RoundsAnanda WulandariNo ratings yet
- Name: Fadly Saban CLASS: 9-12 HOMEWORK (Disorder of Nerve System)Document3 pagesName: Fadly Saban CLASS: 9-12 HOMEWORK (Disorder of Nerve System)Fadly SabanNo ratings yet
- Practical Approach To A Person With Low Backache: Pradeep Kumar Maheshwari, Anjana Pandey, Rosmy JoseDocument5 pagesPractical Approach To A Person With Low Backache: Pradeep Kumar Maheshwari, Anjana Pandey, Rosmy Joseed jireh nangcaNo ratings yet
- Cepheus Journal Issue 012Document52 pagesCepheus Journal Issue 012Scott TayNo ratings yet
- PottDocument2 pagesPottkimNo ratings yet
- NAJOM 3 Mar 1995Document67 pagesNAJOM 3 Mar 1995Juan Manuel AguiarNo ratings yet
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A ReviewDocument6 pagesStevens-Johnson Syndrome and Toxic Epidermal Necrolysis: A Reviewイアン リムホト ザナガNo ratings yet
- Leprosy Type 1 Reaction (Formerly Reversal Reaction) : Bernard Naafs, MD, PHD, Colette L.M. Van Hees, MDDocument14 pagesLeprosy Type 1 Reaction (Formerly Reversal Reaction) : Bernard Naafs, MD, PHD, Colette L.M. Van Hees, MDAdrianus KevinNo ratings yet
- Afp2010 Generalized Rash Diagnostic ApproachDocument5 pagesAfp2010 Generalized Rash Diagnostic ApproachTony NgNo ratings yet
- Nursing DiagnosisDocument3 pagesNursing DiagnosisBadsbabzNo ratings yet
- ACUTE INFLAMMATION VS CHRONIC INFLAMMATION Assignment #2 (CU-1774-2020)Document17 pagesACUTE INFLAMMATION VS CHRONIC INFLAMMATION Assignment #2 (CU-1774-2020)Ali Aasam KhanNo ratings yet
- PREOP3 1 DocxDocument1 pagePREOP3 1 DocxCamille Joy BaliliNo ratings yet
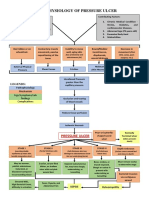
- Pathophysiology of Pressure UlcerDocument1 pagePathophysiology of Pressure UlcerSTORAGE FILENo ratings yet
- Port Folio Camp Andee AstDocument28 pagesPort Folio Camp Andee AstSergi Lee OrateNo ratings yet
- Skin Rashes in ChildrenDocument11 pagesSkin Rashes in ChildrenwiladamanikNo ratings yet
- Oral Medicine 8Document8 pagesOral Medicine 8abdulrazaqNo ratings yet
- Maria Angeline Mendoza BSN 3a2 - Communicable Disease StudyDocument17 pagesMaria Angeline Mendoza BSN 3a2 - Communicable Disease StudyAiram Enilegna AzodnemNo ratings yet
- Examples for Sheets (1) باطنةDocument17 pagesExamples for Sheets (1) باطنةzizoNo ratings yet
- د.جمال المشوليAcute diarrhoea&dehydratin 81085Document9 pagesد.جمال المشوليAcute diarrhoea&dehydratin 81085zizoNo ratings yet
- Lung FibrosisDocument4 pagesLung FibrosiszizoNo ratings yet
- Lung AbscessDocument4 pagesLung AbscesszizoNo ratings yet
- Impacts of Coronavirus On The Mental Health of The Senior High School StudentsDocument3 pagesImpacts of Coronavirus On The Mental Health of The Senior High School StudentsJohn Eirhene Intia BarreteNo ratings yet
- Test Bank For Radiographic Pathology For Technologists 5th Edition KowalczykDocument28 pagesTest Bank For Radiographic Pathology For Technologists 5th Edition Kowalczykgysenickelico85b100% (43)
- 14 Natural Ways To Improve Your Insulin SensitivityDocument8 pages14 Natural Ways To Improve Your Insulin Sensitivitytuto aprikaNo ratings yet
- Final Scientific Goa Masterclass 2020Document5 pagesFinal Scientific Goa Masterclass 2020Abcdef100% (1)
- DPI PPE For Schools COVID VersionDocument43 pagesDPI PPE For Schools COVID VersionJitesh ThakurNo ratings yet
- Irritable Bowel Syndrome H I CH NG Ru T Kích ThíchDocument3 pagesIrritable Bowel Syndrome H I CH NG Ru T Kích Thíchto van quyenNo ratings yet
- Palliative Care Perspectives James L Hallenbeck Full ChapterDocument67 pagesPalliative Care Perspectives James L Hallenbeck Full Chaptermary.kelly334100% (2)
- JaypeeDigital - Ebook ReaderDocument40 pagesJaypeeDigital - Ebook ReaderHanin AbukhiaraNo ratings yet
- Vitamin D FracturesDocument11 pagesVitamin D FracturesHolger LundstromNo ratings yet
- Tobacco Regulation Act of 2003Document2 pagesTobacco Regulation Act of 2003Jarvin SantosNo ratings yet
- Home Visit Bag TechniqueDocument56 pagesHome Visit Bag Techniquekristelaaa guevarraNo ratings yet
- Food Mbio II AssighnmentDocument10 pagesFood Mbio II AssighnmentRazia UrmiNo ratings yet
- SLE and PregnancyDocument10 pagesSLE and PregnancySergio CerpaNo ratings yet
- Narasi Refatar TNF ADocument3 pagesNarasi Refatar TNF APinaufal Ahmad FNo ratings yet
- Project Research Article 8 - AnthuriumDocument16 pagesProject Research Article 8 - AnthuriumErving Lester MagtajasNo ratings yet
- Journal Club Presentation RPGN-1Document53 pagesJournal Club Presentation RPGN-1sagor9364No ratings yet
- CESU ORD DRAFT EDITED Sent To Dr. AlfieDocument7 pagesCESU ORD DRAFT EDITED Sent To Dr. AlfieDulce TomotorgoNo ratings yet
- From PMS To MenopauseDocument196 pagesFrom PMS To MenopauseWeemizo تNo ratings yet
- Covid Care FacilityDocument5 pagesCovid Care FacilityNDTVNo ratings yet
- Health Policy and Planning in IndiaDocument10 pagesHealth Policy and Planning in IndiaShubhaDavalgiNo ratings yet
- Pediatric Health Nursing Unit-Iii Pharmacological Care Aspects While Dealing With Pediatric PatientsDocument107 pagesPediatric Health Nursing Unit-Iii Pharmacological Care Aspects While Dealing With Pediatric PatientsPriya bhatti0% (1)
- Package Leaflet: Information For The User Tamsulosin Hydrochloride 400 Micrograms, Modified-Release Capsule, HardDocument7 pagesPackage Leaflet: Information For The User Tamsulosin Hydrochloride 400 Micrograms, Modified-Release Capsule, HardKahmNo ratings yet
- BIO100 Exam 3 Review SheetDocument8 pagesBIO100 Exam 3 Review SheetSeanNo ratings yet
- Class 2 Cavity Designs For AmalgamDocument10 pagesClass 2 Cavity Designs For AmalgamEpic MonologueNo ratings yet
- MAXICARE Proposal - Wen Parker Logistics Phils.Document18 pagesMAXICARE Proposal - Wen Parker Logistics Phils.Alvin Dela CruzNo ratings yet
- New Mock 1-2022Document29 pagesNew Mock 1-2022nemalijyothsna3No ratings yet