You might also like
- Anticoagulant Pocket GuideDocument8 pagesAnticoagulant Pocket GuideDrew John Minardi100% (2)
- Anticoagulation Protocol For PostDocument8 pagesAnticoagulation Protocol For PostMohammed IbrahimNo ratings yet
- Farma StrokeDocument37 pagesFarma StrokeDAHLIANo ratings yet
- NOAC ChartDocument2 pagesNOAC Chartsgod34No ratings yet
- Venous Thromboembolism With Blanks ResidentsDocument9 pagesVenous Thromboembolism With Blanks Residentsapi-648714317No ratings yet
- Newer Oral Anticoagulant: DR Shivaom Chaurasia Resident Internal MedicineDocument57 pagesNewer Oral Anticoagulant: DR Shivaom Chaurasia Resident Internal MedicineMuhammad Reza FirdausNo ratings yet
- Deep Vein ThrombosisDocument4 pagesDeep Vein ThrombosisStefania CristinaNo ratings yet
- VTE_prophylaxis_PROTOCOL _V1.1_with Forms_07_Dec_2023Document20 pagesVTE_prophylaxis_PROTOCOL _V1.1_with Forms_07_Dec_2023hatem newishyNo ratings yet
- VTE_prophylaxis_PROTOCOL_V1.2_withForms_31_Dec_2023Document19 pagesVTE_prophylaxis_PROTOCOL_V1.2_withForms_31_Dec_2023hatem newishyNo ratings yet
- Enoxaparin Guideline for Prescribing, Administration and MonitoringDocument6 pagesEnoxaparin Guideline for Prescribing, Administration and MonitoringFaheem AlsabriaNo ratings yet
- Enoxaparin Info SheetDocument7 pagesEnoxaparin Info SheetjafarkassimNo ratings yet
- Afib Flowchart 1-21 SLWDocument3 pagesAfib Flowchart 1-21 SLWIndra WijayaNo ratings yet
- Anticoagulatio N Asra Guidelines: Sravya VemuriDocument62 pagesAnticoagulatio N Asra Guidelines: Sravya VemuriSiva Prasad AspNo ratings yet
- Anticoagulants:: Acenocumarol (Sintrom)Document5 pagesAnticoagulants:: Acenocumarol (Sintrom)gocosmaNo ratings yet
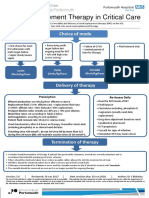
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Vancomycin Dosing and Monitoring in AdultsDocument1 pageVancomycin Dosing and Monitoring in AdultsjulialeoNo ratings yet
- Pro TaminaDocument2 pagesPro TaminaArcenciel26No ratings yet
- Diagnose CKD:: ACE inhibitor/ARB UseDocument2 pagesDiagnose CKD:: ACE inhibitor/ARB UseAman AmanNo ratings yet
- Most of Cardiac Care Unit (C.C.U) DrugsDocument57 pagesMost of Cardiac Care Unit (C.C.U) DrugsOsama OmarNo ratings yet
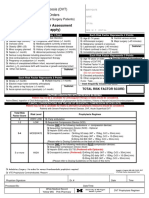
- Thrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersDocument2 pagesThrombosis Risk Factor Assessment (Choose All That Apply) : Deep Vein Thrombosis (DVT) Prophylaxis OrdersPutu Gizha Satrya GautamaNo ratings yet
- Anti CoagulantsDocument37 pagesAnti CoagulantsMaria khurshidNo ratings yet
- Thrombolytic TherapyDocument16 pagesThrombolytic TherapyAnonymous nrZXFwNo ratings yet
- VTE-Prophylaxis-Protocol - MOHDocument13 pagesVTE-Prophylaxis-Protocol - MOHreham ONo ratings yet
- FAQ - DOAC in CKD update - finalDocument4 pagesFAQ - DOAC in CKD update - finalraea.dobsonNo ratings yet
- Hodgkin's Lymphoma Treatment ProtocolDocument3 pagesHodgkin's Lymphoma Treatment ProtocolSindu SankarNo ratings yet
- Ribociclib Protocol CRP13 B034 v1.0Document4 pagesRibociclib Protocol CRP13 B034 v1.0Joana JohnNo ratings yet
- Critical Care Dr. Valerie Zarza GeronDocument88 pagesCritical Care Dr. Valerie Zarza GeronDivine Grace FernandezNo ratings yet
- ANTICOAGULANTS: Oral vs ParenteralDocument103 pagesANTICOAGULANTS: Oral vs Parenteralabhilashreddy45100% (1)
- Enoxaparin Sodium Injection I.PDocument15 pagesEnoxaparin Sodium Injection I.PSuhailansariNo ratings yet
- Hypertension: Classification, Treatment and Special PopulationsDocument21 pagesHypertension: Classification, Treatment and Special PopulationsRawabi SalehNo ratings yet
- Anticoagulation Dosing Recommendations COVID 19 PatientsDocument1 pageAnticoagulation Dosing Recommendations COVID 19 PatientsChalwe HowardNo ratings yet
- Am Iog Lyco SidesDocument2 pagesAm Iog Lyco Sidesthemega1111No ratings yet
- Anticoagulation Monitoring Hand-OutDocument69 pagesAnticoagulation Monitoring Hand-OutApril OcampoNo ratings yet
- Chad Pressors HandoutDocument12 pagesChad Pressors HandoutquelspectacleNo ratings yet
- New Oral New Oral Anticoagulants G: RB H TT MD Rebecca Hanratty, MD Denver Health April 12, 2011Document55 pagesNew Oral New Oral Anticoagulants G: RB H TT MD Rebecca Hanratty, MD Denver Health April 12, 2011andresrgomezNo ratings yet
- Management and Complications of AscitesDocument26 pagesManagement and Complications of Ascitessravan thatiNo ratings yet
- Atrial Fibrillation: Anish DhakalDocument33 pagesAtrial Fibrillation: Anish DhakalDrjawadhussain HussainNo ratings yet
- Nilotinib V4 4.13Document2 pagesNilotinib V4 4.13GabrielNo ratings yet
- Rule Using NOACDocument4 pagesRule Using NOACHarie CiptaNo ratings yet
- Ventura County Medical Center: Mi Thrombolysis, Management ofDocument3 pagesVentura County Medical Center: Mi Thrombolysis, Management ofblackcat657No ratings yet
- Anticoagulants Preoperative InstructionsDocument3 pagesAnticoagulants Preoperative InstructionsDevaki VisvalingamNo ratings yet
- (April 2020) : Is The Indication Appropriate For A Doac?Document1 page(April 2020) : Is The Indication Appropriate For A Doac?SNo ratings yet
- Guide To Drug Dose Adjustment in Renal Impairment: (Based On Cockcroft-Gault Equation, Adapted From BNF)Document2 pagesGuide To Drug Dose Adjustment in Renal Impairment: (Based On Cockcroft-Gault Equation, Adapted From BNF)vi_wiviaNo ratings yet
- Anticoagulation strategies for COVID-19 patients at BMCDocument1 pageAnticoagulation strategies for COVID-19 patients at BMCAvinash KumbharNo ratings yet
- Primary Use of Heparin Is To Prevent Venous Thrombosis,: HeparinsDocument2 pagesPrimary Use of Heparin Is To Prevent Venous Thrombosis,: HeparinsJanna Vivien Prigo BaldioNo ratings yet
- Hosp Ops II Week 2 Questions 1Document3 pagesHosp Ops II Week 2 Questions 1api-650133203No ratings yet
- Cardene IV quick referenceDocument1 pageCardene IV quick referenceLisa Trisnawati ChaniagoNo ratings yet
- Direct Oral Anticoagulants (DOACs) for treatment of DVTDocument11 pagesDirect Oral Anticoagulants (DOACs) for treatment of DVTLuana MNo ratings yet
- Tishk International University: ApixabanDocument4 pagesTishk International University: ApixabanDyar MzafarNo ratings yet
- Switching From Various AnticoagulantsDocument3 pagesSwitching From Various AnticoagulantsKhadejah StewartNo ratings yet
- Calcium Channel BlockersDocument15 pagesCalcium Channel Blockersfarmasi_hm100% (2)
- Enoxaparin - Safe Prescribing - Check It Out 1Document3 pagesEnoxaparin - Safe Prescribing - Check It Out 1Zaid DewachiNo ratings yet
- Hypertensive Urgency EmergencyDocument5 pagesHypertensive Urgency Emergencydamondouglas100% (3)
- Receiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyDocument272 pagesReceiving Concurrent Moderate CYP3A4 Inhibitors (Erythromycin, Saquinavir, Verapamil, Fluconazole) - 25 MG Once Daily InitiallyFatima Doran PandaogNo ratings yet
- Carboplatin PaclitaxelDocument6 pagesCarboplatin PaclitaxelNida Auliya RahmahNo ratings yet
- Medicine RotatationbookletDocument20 pagesMedicine RotatationbookletJanelle JosephsNo ratings yet
- Mini Warfarin GuidelinesDocument2 pagesMini Warfarin GuidelinesPeunn NattaphatNo ratings yet
- Venous Thromboembolism (Vte) : Abdullah Al Dahbali, Mpharm, PHDDocument23 pagesVenous Thromboembolism (Vte) : Abdullah Al Dahbali, Mpharm, PHDعزالدين الطيارNo ratings yet
- Lewy Body DementiaDocument6 pagesLewy Body DementiaMuhammad Reza FirdausNo ratings yet
- Screenshot 2022-10-10 at 10.55.11Document10 pagesScreenshot 2022-10-10 at 10.55.11Muhammad Reza FirdausNo ratings yet
- Ceftriaxone Therapy Attenuates Brain Trauma in Rats by Affecting Glutamate Transporters and Neuroinflammation and Not by Its Antibacterial EffectsDocument14 pagesCeftriaxone Therapy Attenuates Brain Trauma in Rats by Affecting Glutamate Transporters and Neuroinflammation and Not by Its Antibacterial EffectsMuhammad Reza FirdausNo ratings yet
- Screenshot 2022-12-01 at 21.26.47Document1 pageScreenshot 2022-12-01 at 21.26.47Muhammad Reza FirdausNo ratings yet
- Dementiawithlewybodies0619 190610153624Document15 pagesDementiawithlewybodies0619 190610153624Muhammad Reza FirdausNo ratings yet
- Screenshot 2022-12-01 at 21.26.47Document1 pageScreenshot 2022-12-01 at 21.26.47Muhammad Reza FirdausNo ratings yet
- Strokeaha 119 025997Document7 pagesStrokeaha 119 025997Muhammad Reza FirdausNo ratings yet
- 1 s2.0 S0014299921000522 MainDocument9 pages1 s2.0 S0014299921000522 MainMuhammad Reza FirdausNo ratings yet
- Cerebellar Stroke in A COVID-19 Infected Patient. A Case ReportDocument6 pagesCerebellar Stroke in A COVID-19 Infected Patient. A Case ReportMuhammad Reza FirdausNo ratings yet
- Other FeaturesDocument1 pageOther FeaturesMuhammad Reza FirdausNo ratings yet
- Newer Oral Anticoagulant: DR Shivaom Chaurasia Resident Internal MedicineDocument57 pagesNewer Oral Anticoagulant: DR Shivaom Chaurasia Resident Internal MedicineMuhammad Reza FirdausNo ratings yet
- 1 s2.0 S0014299921000509 MainDocument8 pages1 s2.0 S0014299921000509 MainMuhammad Reza FirdausNo ratings yet
- 1 s2.0 S0014299921000492 MainDocument10 pages1 s2.0 S0014299921000492 MainMuhammad Reza FirdausNo ratings yet
- 2Document1 page2Muhammad Reza FirdausNo ratings yet
- Mapping Bedah Saraf SeninDocument6 pagesMapping Bedah Saraf SeninMuhammad Reza FirdausNo ratings yet
- CamScanner 10-29-2021 16.45Document1 pageCamScanner 10-29-2021 16.45Muhammad Reza FirdausNo ratings yet
- 2 CompressedDocument1 page2 CompressedMuhammad Reza FirdausNo ratings yet
- BEDAH SARAF PASIEN MAPPINGDocument7 pagesBEDAH SARAF PASIEN MAPPINGMuhammad Reza FirdausNo ratings yet
- Mapping Bedah Saraf SelasaDocument7 pagesMapping Bedah Saraf SelasaMuhammad Reza FirdausNo ratings yet
- Mapping Bedah Saraf JumatDocument6 pagesMapping Bedah Saraf JumatMuhammad Reza FirdausNo ratings yet
- Answer Key in AnaphyDocument16 pagesAnswer Key in AnaphyDE LEON ALLIANA MARIE100% (1)
- Histology, Lecture 12, The Lymphatic System (LEcture Notes)Document6 pagesHistology, Lecture 12, The Lymphatic System (LEcture Notes)Ali Al-QudsiNo ratings yet
- Risk - Factors - For - Surgical - Site - Infection20160808 22525 14yjbrc With Cover Page v2Document7 pagesRisk - Factors - For - Surgical - Site - Infection20160808 22525 14yjbrc With Cover Page v2Ana MîndrilăNo ratings yet
- Comparing The Efficacy of Scaling With Root Planing and Modified Widman Flap in Patients With Chronic PeriodontitisDocument7 pagesComparing The Efficacy of Scaling With Root Planing and Modified Widman Flap in Patients With Chronic PeriodontitisZana Salsabila ChobitaNo ratings yet
- Auto PeepDocument6 pagesAuto PeepVadelain GaldamesNo ratings yet
- DR - Ziauddin A Kashmiri - Chest Tube Drainage-UpdatedDocument9 pagesDR - Ziauddin A Kashmiri - Chest Tube Drainage-UpdatedAli AftabNo ratings yet
- 2nd Preparatory Course OMFSDocument2 pages2nd Preparatory Course OMFSkhurramnadeemNo ratings yet
- Chalazion: Patient Information-AdnexalDocument3 pagesChalazion: Patient Information-Adnexalgek yoshiNo ratings yet
- Post-op patient assessmentDocument1 pagePost-op patient assessmentStephany Dela CruzNo ratings yet
- Basic Guide To Dental Procedures - (Glossary of Terms)Document4 pagesBasic Guide To Dental Procedures - (Glossary of Terms)ofentsemphotlharipeNo ratings yet
- Introduction To ECMODocument35 pagesIntroduction To ECMOEko SarwowibowoNo ratings yet
- HELDMANN 1999 The Association of Propofol Usage With Posoperatve Wound Infection Rate in Clean Wounds PDFDocument4 pagesHELDMANN 1999 The Association of Propofol Usage With Posoperatve Wound Infection Rate in Clean Wounds PDFAntonio PG´sNo ratings yet
- International Journal of Surgery Case Reports: Anita Nur Charisma, Arief BakhtiarDocument4 pagesInternational Journal of Surgery Case Reports: Anita Nur Charisma, Arief BakhtiarNurwinda AgnesiaNo ratings yet
- ISPNO 2022 - Impact of The COVID-19 Pandemic On 30-Day Mortality and Unplanned Reoperation Rates For Pediatric Central Nervous System TumorsDocument2 pagesISPNO 2022 - Impact of The COVID-19 Pandemic On 30-Day Mortality and Unplanned Reoperation Rates For Pediatric Central Nervous System TumorsDiana SanchezNo ratings yet
- Duties or NurseDocument10 pagesDuties or NursehailleyannNo ratings yet
- Heart Valve SurgeryDocument16 pagesHeart Valve SurgeryMundhir Al-KhusaibiNo ratings yet
- Miltex General Instruments BrochureDocument5 pagesMiltex General Instruments BrochureMichael Angelo Detalla MacolorNo ratings yet
- Argumentative Essay Plastic SurgeryDocument3 pagesArgumentative Essay Plastic SurgeryCatherine BaniquedNo ratings yet
- Maternal NursingDocument48 pagesMaternal NursingMarwa DaghNo ratings yet
- NBME 7 - Answers & Explanations (SP)Document70 pagesNBME 7 - Answers & Explanations (SP)JUAN CHAVEZNo ratings yet
- Compre MCNDocument21 pagesCompre MCNMary Ann G. CorsanesNo ratings yet
- Micro-Needling Post Treatment InstructionsDocument1 pageMicro-Needling Post Treatment InstructionsMarian YuqueNo ratings yet
- Mechanical Ventilator GuideDocument3 pagesMechanical Ventilator GuideDivine Mercy De JulianNo ratings yet
- Hospital procedural charges guideDocument5 pagesHospital procedural charges guideSyed RuksarNo ratings yet
- Qbase Anaesthesia, Vol 5 MCQ S For The Final.76Document2 pagesQbase Anaesthesia, Vol 5 MCQ S For The Final.76Maged Raafat0% (1)
- Thoracic Veins and Arteries.Document14 pagesThoracic Veins and Arteries.Shimmering MoonNo ratings yet
- Assessment Algorithm For Sedated Adult ICU Patients: No YesDocument18 pagesAssessment Algorithm For Sedated Adult ICU Patients: No Yesbambang aryanto100% (3)
- Biology NMAT Notes AnatomyCirculatory and RespiratoryDocument13 pagesBiology NMAT Notes AnatomyCirculatory and RespiratoryMa. Teresa M. AbainzaNo ratings yet
- DR - Kavita Priya Iicm 1Document68 pagesDR - Kavita Priya Iicm 1Kavita PriyaNo ratings yet
- Abdominal TBDocument53 pagesAbdominal TBnaveen kumar kushwahaNo ratings yet