You might also like
- Abortion and Sterilization: Medical and Social AspectsFrom EverandAbortion and Sterilization: Medical and Social AspectsJane E. HodgsonNo ratings yet
- 2023 OB/GYN Coding Manual: Components of Correct CodingFrom Everand2023 OB/GYN Coding Manual: Components of Correct CodingNo ratings yet
- (Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDocument10 pages(Gyne) 2.1 PCOS, Hyperandrogenism & Hyperprolactenemia (OnaCruz) - WiniDexter IanNo ratings yet
- Total Abdominal HysterectomyDocument19 pagesTotal Abdominal HysterectomyMeidina Rachma Amanda100% (1)
- Pelvic Inflammatory Disease by SlidesgoDocument51 pagesPelvic Inflammatory Disease by SlidesgoGina MorenoNo ratings yet
- Obstetric Anal Sphincter Injury (OASIS) - UpToDateDocument39 pagesObstetric Anal Sphincter Injury (OASIS) - UpToDateErickNo ratings yet
- Presented by DR - Shahbaz Ahmad Professor of Community MedicineDocument76 pagesPresented by DR - Shahbaz Ahmad Professor of Community MedicinePriya bhattiNo ratings yet
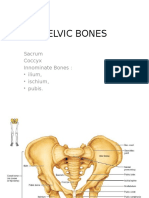
- Pelvic BoneDocument15 pagesPelvic BoneYoanneveline TanakNo ratings yet
- Cardiac Disease in PregnancyDocument28 pagesCardiac Disease in PregnancyviharadewiNo ratings yet
- Claire Maevelle A. Laxamana BSP - 3ADocument10 pagesClaire Maevelle A. Laxamana BSP - 3ACLaire Maevelle Angeles LaxamanaNo ratings yet
- Surgery - Data Show (All-In-One Collections)Document399 pagesSurgery - Data Show (All-In-One Collections)anmar alkhudhriNo ratings yet
- Benign and Malignant Ovarian Tumors: Case 1Document14 pagesBenign and Malignant Ovarian Tumors: Case 1Charrie RagadiNo ratings yet
- Rapid Review of Hematology (Aug 31, 2013) - (9350909618) - (Jaypee Brothers Medical Pub)Document149 pagesRapid Review of Hematology (Aug 31, 2013) - (9350909618) - (Jaypee Brothers Medical Pub)Dana AhmedNo ratings yet
- PulseDocument43 pagesPulseAngelo LacisteNo ratings yet
- GEN GallBladderInstrumentsADocument10 pagesGEN GallBladderInstrumentsANeo Rodriguez AlvaradoNo ratings yet
- Evaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusDocument7 pagesEvaluation of Right Side Foetal Myocardial Performance Index in Pregestational and Gestational Diabetes MellitusGabyliz Gonzalez CastilloNo ratings yet
- Disorder of Sex DevelopmentDocument40 pagesDisorder of Sex DevelopmentAndi AdityaNo ratings yet
- ANATOMY OF FEMALE InternalDocument49 pagesANATOMY OF FEMALE InternalJohaifha CompaniaNo ratings yet
- Ob-Gyn Review Part 3Document101 pagesOb-Gyn Review Part 3filchibuffNo ratings yet
- Foreign Body in Pharynx, Larynx, Trachea & Tracheobronchial TreeDocument26 pagesForeign Body in Pharynx, Larynx, Trachea & Tracheobronchial TreehashyNo ratings yet
- Normal Conduct of LaborDocument62 pagesNormal Conduct of LaborFaye Cabotaje LinganNo ratings yet
- Conduct of LaborDocument8 pagesConduct of LaborChristine Evan HoNo ratings yet
- Pregnancy and Labor at Fetal Malpresentations and Abnormal PelvisDocument40 pagesPregnancy and Labor at Fetal Malpresentations and Abnormal PelvisCoral Srinivasa Ramalu100% (1)
- Hepatitis B in PregnancyDocument17 pagesHepatitis B in PregnancysnazzyNo ratings yet
- Breast Cancer - McMaster Pathophysiology Review PDFDocument8 pagesBreast Cancer - McMaster Pathophysiology Review PDFAprilla Ayu W.No ratings yet
- Breast MassDocument38 pagesBreast MassLester Paul SivilaNo ratings yet
- Mass in Epigastrium-2Document37 pagesMass in Epigastrium-2brown_chocolate87643100% (1)
- Ultrasound-Guided Invasive Procedures in ObstetricsDocument18 pagesUltrasound-Guided Invasive Procedures in ObstetricsariNo ratings yet
- Obs History Taking FormatDocument24 pagesObs History Taking FormatBibek PandeyNo ratings yet
- Procedural ReportDocument14 pagesProcedural ReportiamcharraeNo ratings yet
- د.عبد الزهره THE GYNAECOLOGICAL EXAMINATION-1 (Muhadharaty)Document29 pagesد.عبد الزهره THE GYNAECOLOGICAL EXAMINATION-1 (Muhadharaty)MohammedNo ratings yet
- Gyne ReflectionDocument18 pagesGyne ReflectionKC Dela RosaNo ratings yet
- Second Trimester Complications 2015Document64 pagesSecond Trimester Complications 2015gibreilNo ratings yet
- Cervical CancerDocument6 pagesCervical CancerCnette S. LumboNo ratings yet
- Urodynamics: Committee 7Document56 pagesUrodynamics: Committee 7Coral Garcia RiveraNo ratings yet
- FIGO Cancer Report 2018 PDFDocument128 pagesFIGO Cancer Report 2018 PDFAndi Tiara S. AdamNo ratings yet
- Obstetrics and Gynecological InstrumentsDocument31 pagesObstetrics and Gynecological InstrumentsGAYATHRI RAKESHNo ratings yet
- Endometriosis With Salpingitis Simulating Acute AppendicitisDocument20 pagesEndometriosis With Salpingitis Simulating Acute AppendicitisWyendae CliquersNo ratings yet
- Care of A Client With: Neonatal Pneumonia: University of Southern Philippines Foundation Salinas Drive, Lahug, Cebu CityDocument22 pagesCare of A Client With: Neonatal Pneumonia: University of Southern Philippines Foundation Salinas Drive, Lahug, Cebu CityAsterlyn ConiendoNo ratings yet
- Tog Journal 2016Document61 pagesTog Journal 2016thevijay007100% (1)
- AUVARD Vaginal SpeculaDocument24 pagesAUVARD Vaginal SpeculaRoy SandiNo ratings yet
- Congenital Anomelies of Reproductive OrgansDocument47 pagesCongenital Anomelies of Reproductive Organsdr_shamimrNo ratings yet
- CPG Uterine InversionDocument3 pagesCPG Uterine InversionRahmayanti YuliaNo ratings yet
- CTT InsertionDocument18 pagesCTT InsertionRen-Ren NazarenoNo ratings yet
- The Management of Asherman Syndrome: A Review of LiteratureDocument11 pagesThe Management of Asherman Syndrome: A Review of LiteratureEuphra Adellheid100% (1)
- Malaria in Pregnancy 4Document35 pagesMalaria in Pregnancy 4api-3705046No ratings yet
- Endoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and ComplicationsDocument16 pagesEndoscopy - Hysteroscopy and Laparoscopy Indications, Contraindications and Complicationsselatur100% (1)
- Table 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationDocument111 pagesTable 4.1 AFS Classifi Cation System (: The Embryological-Clinical Classifi CationArya Syafaromania RachmaNo ratings yet
- RISE REVIEW - Female Reproductive SystemDocument9 pagesRISE REVIEW - Female Reproductive SystemGerben Villanueva100% (1)
- Acog Practice Bulletin Summary: Pregestational Diabetes MellitusDocument3 pagesAcog Practice Bulletin Summary: Pregestational Diabetes MellitusMaría Fernanda Palma AcostaNo ratings yet
- Harare Obs N GynDocument96 pagesHarare Obs N GynRobert L G MabongaNo ratings yet
- 002 Intrapartum Fetal Heart Rate Monitoring 3a - ACOG Bulletin 106 PDFDocument11 pages002 Intrapartum Fetal Heart Rate Monitoring 3a - ACOG Bulletin 106 PDFale_fearNo ratings yet
- Medical History Taking Study GuideDocument6 pagesMedical History Taking Study GuideSarra Mood ImanNo ratings yet
- Obstetrics, Gynaecology-Textbook of Obstetrics and Gynaecology For Medical Students, 2nd Edition-Akin Agboola-2006Document559 pagesObstetrics, Gynaecology-Textbook of Obstetrics and Gynaecology For Medical Students, 2nd Edition-Akin Agboola-2006fagiy51113No ratings yet
- Module E Shock, MODS Roy Model-Oxygenation-Perfusion Required Readings (See Syllabus For Detailed Reading)Document7 pagesModule E Shock, MODS Roy Model-Oxygenation-Perfusion Required Readings (See Syllabus For Detailed Reading)Jeff ZhouNo ratings yet
- Uterine FibroidsDocument21 pagesUterine FibroidsPrasun BiswasNo ratings yet
- Pulmonary Disorders in PregnancyDocument49 pagesPulmonary Disorders in PregnancyMara Medina - BorleoNo ratings yet
- Management of CA Vulva 2Document33 pagesManagement of CA Vulva 2api-3705046No ratings yet
- Kelenjar LakrimalDocument44 pagesKelenjar LakrimalNurfanida Natasya MNo ratings yet
- Problem-based Approach to Gastroenterology and HepatologyFrom EverandProblem-based Approach to Gastroenterology and HepatologyJohn N. PlevrisNo ratings yet
- Pussy Pedia 2008Document47 pagesPussy Pedia 2008LCLibrary40% (153)
- Health-Asessment-Finals 2Document92 pagesHealth-Asessment-Finals 2Ebun Rosa100% (1)
- Hotpantz: Herbal GynecologyDocument28 pagesHotpantz: Herbal GynecologyMandy M.100% (20)
- Aesthetic Labia Minora and Clitoral Hood Reduction Using Extended Central Wedge ResectionDocument10 pagesAesthetic Labia Minora and Clitoral Hood Reduction Using Extended Central Wedge ResectionHazel Vivian Soliz AlconzNo ratings yet
- Shendi Obs OsceDocument35 pagesShendi Obs OsceYassin Jamal67% (3)
- The Vulva - Structure - Innervation - TeachMeAnatomyDocument3 pagesThe Vulva - Structure - Innervation - TeachMeAnatomywzt2001No ratings yet
- Procedure 28-18 Assessing The Female Genitals and Inguinal AreaDocument2 pagesProcedure 28-18 Assessing The Female Genitals and Inguinal Areakirsten galletaNo ratings yet
- Resolution-Rape (Final)Document7 pagesResolution-Rape (Final)HadjieLimNo ratings yet
- LaparosDocument3 pagesLaparosMurtaz BokhuaNo ratings yet
- Background and Precancerous Diseases of Female Genital Organs.Document43 pagesBackground and Precancerous Diseases of Female Genital Organs.Dae Shim100% (1)
- Chapter 2 Maternal Anatomy WilliamsDocument60 pagesChapter 2 Maternal Anatomy WilliamsDiskaAstariniNo ratings yet
- Bartholin's Gland Cyst MarsupializationDocument3 pagesBartholin's Gland Cyst MarsupializationAde Churie Tanjaya50% (2)
- 1a. Reproductive OrgansDocument60 pages1a. Reproductive OrgansJerrald Meyer L. BayaniNo ratings yet
- MARTINEZ PEREZ Labia Minora Elongation As Understood byDocument15 pagesMARTINEZ PEREZ Labia Minora Elongation As Understood byGuillermoMartinezPerezNo ratings yet
- A Brief Materia Medica of Some Lesser-Known NosodesDocument103 pagesA Brief Materia Medica of Some Lesser-Known NosodesnitkolNo ratings yet
- Instructional Module in Understanding The Self: School of Teacher EducationDocument5 pagesInstructional Module in Understanding The Self: School of Teacher EducationAlyanna MagkalasNo ratings yet
- Prolapse in CattleDocument2 pagesProlapse in Cattleirma safitriNo ratings yet
- Case Study 3D FinaaaalDocument34 pagesCase Study 3D FinaaaalPaul AnteNo ratings yet
- Perineum - The Anatomy of The PerineumDocument6 pagesPerineum - The Anatomy of The PerineumimvavNo ratings yet
- Suturing Perineal LacerationsDocument49 pagesSuturing Perineal LacerationsOfel Santillan100% (2)
- Anaphy Finals ReviewerDocument193 pagesAnaphy Finals Reviewerxuxi dulNo ratings yet
- Phantom ObgynDocument4 pagesPhantom ObgynHengki HaryandaNo ratings yet
- Pochette Imp. Vagino AngDocument26 pagesPochette Imp. Vagino AngMontrealthrowaway19No ratings yet
- Obstetrics LacerationsDocument15 pagesObstetrics LacerationsMauricio CorreaNo ratings yet
- Meat Curtains - Google SearchDocument1 pageMeat Curtains - Google SearchMr. BeddingfieldNo ratings yet
- Jurnal Kuda 1Document21 pagesJurnal Kuda 1Yulistia FadhilahNo ratings yet
- A Review On Yoni DhupanaDocument3 pagesA Review On Yoni DhupanaResearch Park0% (1)
- MCHN OutlineDocument15 pagesMCHN OutlineAngel Strauss KmpsnNo ratings yet
- Toygasms! - Sadie AllisonDocument161 pagesToygasms! - Sadie Allisonmtine40% (5)
- KKPMT IV Genito Uri N60 - N99Document170 pagesKKPMT IV Genito Uri N60 - N99Clarains FriskaNo ratings yet