You might also like
- Welding Capacity Analysis: Weld Is Adequate & Stress Ratio 0.86Document1 pageWelding Capacity Analysis: Weld Is Adequate & Stress Ratio 0.86Engr Benalito A Catap IIINo ratings yet
- Healing Lyme: Buhner Core Protocol (Unofficial) PDFDocument4 pagesHealing Lyme: Buhner Core Protocol (Unofficial) PDFSteluța DrâmbuNo ratings yet
- Ship Construction MMD DG SHIPPING Edrich Fernandes Phase I II Second 2nd MatesDocument78 pagesShip Construction MMD DG SHIPPING Edrich Fernandes Phase I II Second 2nd MatesGurjit Singh100% (2)
- Pipe Sizing Calculation SheetDocument14 pagesPipe Sizing Calculation SheetJayakrishnan RadhakrishnanNo ratings yet
- CT SizingDocument62 pagesCT SizingMohamed TalebNo ratings yet
- Lampiran I and J - Mqa 04 PDFDocument29 pagesLampiran I and J - Mqa 04 PDFPuteri Angreni QistinaNo ratings yet
- Turn Around Coordinator Job DescriptionDocument2 pagesTurn Around Coordinator Job DescriptionMikeNo ratings yet
- 70 Valves SolenoidDocument105 pages70 Valves SolenoidrizalNo ratings yet
- Excon2019 ShowPreview02122019 PDFDocument492 pagesExcon2019 ShowPreview02122019 PDFSanjay KherNo ratings yet
- Project - New Restuarant Management System The Grill HouseDocument24 pagesProject - New Restuarant Management System The Grill HouseMayank Mahajan100% (3)
- SGA President Goes To Washington: Jazz Band Lands Next Big Gig atDocument8 pagesSGA President Goes To Washington: Jazz Band Lands Next Big Gig atconnollymc1210No ratings yet
- Monergism Vs SynsergismDocument11 pagesMonergism Vs SynsergismPam AgtotoNo ratings yet
- SimovertDocument41 pagesSimovertRamez YassaNo ratings yet
- Letter Word Rec Error Analysis Form BDocument3 pagesLetter Word Rec Error Analysis Form BRoshni SondhiNo ratings yet
- Benevisión N15 Mindray Service ManualDocument123 pagesBenevisión N15 Mindray Service ManualSulay Avila LlanosNo ratings yet
- T2 Part A Q D BoundariesDocument3 pagesT2 Part A Q D BoundariesAxelNo ratings yet
- T2 - Part C - Q2 - Manage Scope ChangesDocument3 pagesT2 - Part C - Q2 - Manage Scope ChangesAxelNo ratings yet
- PingDocument15 pagesPingapi-3844182No ratings yet
- Weldability Chart MRW 01 2015Document1 pageWeldability Chart MRW 01 2015vui01No ratings yet
- Reading SWBSDocument1 pageReading SWBSMariana Panypani ContrerasNo ratings yet
- Mazal Tov!: King David Matrics!Document43 pagesMazal Tov!: King David Matrics!mphoNo ratings yet
- Carte Village Pietonnier TremblantDocument2 pagesCarte Village Pietonnier TremblantNNo ratings yet
- Long HillDocument1 pageLong HillmbrackenburyNo ratings yet
- Ikea Cheras Store LayoutDocument1 pageIkea Cheras Store LayoutMuhammad MuhaiminNo ratings yet
- Monroe Hinge BrochureDocument9 pagesMonroe Hinge BrochureYorche AlternoNo ratings yet
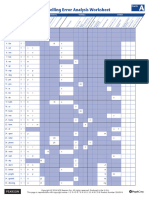
- Spelling Error Analysis Form BDocument2 pagesSpelling Error Analysis Form BRoshni SondhiNo ratings yet
- Liesing: Montag-Freitag (Schule) Montag-Freitag (Ferien) Samstag Sonn-Und FeiertagDocument28 pagesLiesing: Montag-Freitag (Schule) Montag-Freitag (Ferien) Samstag Sonn-Und FeiertagSamuel PuławskiNo ratings yet
- Acceleration Lanes ModelDocument1 pageAcceleration Lanes ModelMainge KihoriNo ratings yet
- Weld Is Adequate & Stress Ratio 0.51Document1 pageWeld Is Adequate & Stress Ratio 0.51eric escobarNo ratings yet
- Summer Fall Sped Internship Log TemplateDocument4 pagesSummer Fall Sped Internship Log Templateapi-339789222No ratings yet
- Jadwal Pgmi 3 2022-2023Document1 pageJadwal Pgmi 3 2022-2023Azizah Adelia RahmaNo ratings yet
- Live Dashboard - SummaryDocument1 pageLive Dashboard - Summarysyaza AtikahNo ratings yet
- SampleDocument13 pagesSampleLuiz FabricioNo ratings yet
- Exchange Releases ProductionDocument5 pagesExchange Releases ProductionVijayNo ratings yet
- RM 56Document1 pageRM 560034941No ratings yet
- 1: 1 0 0 Minec.: Nivel Cubierta de FuegoDocument1 page1: 1 0 0 Minec.: Nivel Cubierta de Fuegoanthony acuñaNo ratings yet
- Nonsense Word Error Analysis Form BDocument2 pagesNonsense Word Error Analysis Form BRoshni SondhiNo ratings yet
- Digimap RoamDocument1 pageDigimap RoamPaoloNo ratings yet
- Arket: Accomplished By: Submitted To: Date AccomplishedDocument2 pagesArket: Accomplished By: Submitted To: Date AccomplishedRon CatalanNo ratings yet
- 2021 - FORM 1099 - Check List Hoang BachDocument2 pages2021 - FORM 1099 - Check List Hoang BachHoang BachNo ratings yet
- BLKonBLK MagazineDocument122 pagesBLKonBLK Magazinearnoldg92No ratings yet
- Peta Dunia (Fizikal)Document2 pagesPeta Dunia (Fizikal)Oboi Mw Blajar UdaNo ratings yet
- Field MapDocument1 pageField MapkoolrunsNo ratings yet
- 1 Ankunft, Terminal 3 (Zugang) : Mazur ParkplatzDocument15 pages1 Ankunft, Terminal 3 (Zugang) : Mazur ParkplatzTijana SekulovNo ratings yet
- Assignment2 JohnsonmDocument11 pagesAssignment2 Johnsonmapi-643878757No ratings yet
- OLX (OLX Praca) : ProblemDocument1 pageOLX (OLX Praca) : ProblemjulkaluksaNo ratings yet
- Spelling Error Analysis Form ADocument2 pagesSpelling Error Analysis Form ARoshni SondhiNo ratings yet
- Modelo Services Agreement REV 07 31.01.22 FINAL Anexos-ManifestoDocument134 pagesModelo Services Agreement REV 07 31.01.22 FINAL Anexos-ManifestoLeandro BorjaNo ratings yet
- Petrified Forest National Park: Painted Desert Visitor CenterDocument1 pagePetrified Forest National Park: Painted Desert Visitor CenterNaaman TakidinNo ratings yet
- Rudrakshi SharmaDocument11 pagesRudrakshi SharmaPrashant A UNo ratings yet
- Theft From Motor Vehicle Maps For Aug. 19 To 25, 2019Document3 pagesTheft From Motor Vehicle Maps For Aug. 19 To 25, 2019Teresa VerencaNo ratings yet
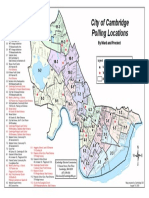
- Updated Map of Polling Places in Cambridge For 2020 PrimaryDocument1 pageUpdated Map of Polling Places in Cambridge For 2020 PrimaryAmyNo ratings yet
- Fastbind EliteXT SPDocument16 pagesFastbind EliteXT SPLidograf Used Printing MachinesNo ratings yet
- Unit 1 CHP 3Document3 pagesUnit 1 CHP 3kala1975No ratings yet
- Leyline Scam Printable SB GuideDocument1 pageLeyline Scam Printable SB GuideRockfist7No ratings yet
- Journal & Republican and Carthage Republican Tribune Progress Edition 2018Document160 pagesJournal & Republican and Carthage Republican Tribune Progress Edition 2018wdt_rpominvilleNo ratings yet
- GA-I (H) D 1000 Series ROBOTDocument1 pageGA-I (H) D 1000 Series ROBOTmfarrukhkNo ratings yet
- Buildings To Demolish PK3Document1 pageBuildings To Demolish PK3juancmuNo ratings yet
- Letter - Word - Rec - Error Analysis - Form - ADocument3 pagesLetter - Word - Rec - Error Analysis - Form - ARoshni SondhiNo ratings yet
- Seniority List of Provincial Public Management Assistant Service - Supra GradeDocument2 pagesSeniority List of Provincial Public Management Assistant Service - Supra Gradenpgovlk100% (2)
- SiwanDocument378 pagesSiwanAlok MishraNo ratings yet
- Beef Carcass 2019Document1 pageBeef Carcass 2019api-351952282No ratings yet
- NSU MapDocument1 pageNSU MapJeff ThompsonNo ratings yet
- TP - M019 - M020 Section - 14,15,16Document1 pageTP - M019 - M020 Section - 14,15,16ON ROADING CONTRACTING LLCNo ratings yet
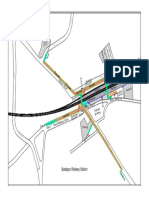
- Badlapur Railway Station1Document1 pageBadlapur Railway Station1Praveen Singh ChauhanNo ratings yet
- 2018 Yearly Trailer Check ListDocument2 pages2018 Yearly Trailer Check ListCogbillConstructionNo ratings yet
- Experimental Verification and Electromagnetic Analysis For Force Performance of Levitation and Guidance Electromagnet in Semi-High-Speed Maglev TrainDocument1 pageExperimental Verification and Electromagnetic Analysis For Force Performance of Levitation and Guidance Electromagnet in Semi-High-Speed Maglev TrainManuel DíazNo ratings yet
- 2.analysis and Control of Electromagnetic Coupling Effect of Levitation and Guidance Systems For Semi-High-Speed Maglev Train Considering Current DirectionDocument4 pages2.analysis and Control of Electromagnetic Coupling Effect of Levitation and Guidance Systems For Semi-High-Speed Maglev Train Considering Current DirectionManuel DíazNo ratings yet
- 1.an Advanced Control Strategy For Magnetic Levitation Train System Based On An Online Adaptive Pid ControllerDocument6 pages1.an Advanced Control Strategy For Magnetic Levitation Train System Based On An Online Adaptive Pid ControllerManuel DíazNo ratings yet
- A High-Efficiency Step-Up Current-Fed PushPull Quasi-Resonant Converter With Fewer Components For Fuel Cell ApplicationDocument10 pagesA High-Efficiency Step-Up Current-Fed PushPull Quasi-Resonant Converter With Fewer Components For Fuel Cell ApplicationManuel DíazNo ratings yet
- Strucure Design and Multi - Objective Optimization of A Novel NPR Bumber SystemDocument19 pagesStrucure Design and Multi - Objective Optimization of A Novel NPR Bumber System施元No ratings yet
- Rule 113 114Document7 pagesRule 113 114Shaila GonzalesNo ratings yet
- MGMT Audit Report WritingDocument28 pagesMGMT Audit Report WritingAndrei IulianNo ratings yet
- Residual Power Series Method For Obstacle Boundary Value ProblemsDocument5 pagesResidual Power Series Method For Obstacle Boundary Value ProblemsSayiqa JabeenNo ratings yet
- Costbenefit Analysis 2015Document459 pagesCostbenefit Analysis 2015TRÂM NGUYỄN THỊ BÍCHNo ratings yet
- IKEA SHANGHAI Case StudyDocument5 pagesIKEA SHANGHAI Case StudyXimo NetteNo ratings yet
- Partes de La Fascia Opteva Y MODULOSDocument182 pagesPartes de La Fascia Opteva Y MODULOSJuan De la RivaNo ratings yet
- Vendor Information Sheet - LFPR-F-002b Rev. 04Document6 pagesVendor Information Sheet - LFPR-F-002b Rev. 04Chelsea EsparagozaNo ratings yet
- Chapter 13 Exercises With AnswerDocument5 pagesChapter 13 Exercises With AnswerTabitha HowardNo ratings yet
- Test ScienceDocument2 pagesTest Sciencejam syNo ratings yet
- Career Essay 1Document2 pagesCareer Essay 1api-572592063No ratings yet
- PR KehumasanDocument14 pagesPR KehumasanImamNo ratings yet
- Recommendations For Students With High Functioning AutismDocument7 pagesRecommendations For Students With High Functioning AutismLucia SaizNo ratings yet
- Technology Management 1Document38 pagesTechnology Management 1Anu NileshNo ratings yet
- Fss Presentation Slide GoDocument13 pagesFss Presentation Slide GoReinoso GreiskaNo ratings yet
- Equivalent Fractions Activity PlanDocument6 pagesEquivalent Fractions Activity Planapi-439333272No ratings yet
- SHCDocument81 pagesSHCEng Mostafa ElsayedNo ratings yet
- Impact of Advertising On Consumers' Buying Behavior Through Persuasiveness, Brand Image, and Celebrity EndorsementDocument10 pagesImpact of Advertising On Consumers' Buying Behavior Through Persuasiveness, Brand Image, and Celebrity Endorsementvikram singhNo ratings yet
- Opc PPT FinalDocument22 pagesOpc PPT FinalnischalaNo ratings yet
- II 2022 06 Baena-Rojas CanoDocument11 pagesII 2022 06 Baena-Rojas CanoSebastian GaonaNo ratings yet
- Damodaram Sanjivayya National Law University Visakhapatnam, A.P., IndiaDocument25 pagesDamodaram Sanjivayya National Law University Visakhapatnam, A.P., IndiaSumanth RoxtaNo ratings yet
- Lecture 4 ENGR 243 DynamicsDocument45 pagesLecture 4 ENGR 243 DynamicsRobby RebolledoNo ratings yet