You might also like
- Ent Assessment PDFDocument10 pagesEnt Assessment PDFvijayalakshmiNo ratings yet
- Nursing Care Plan for Tetralogy of FallotDocument17 pagesNursing Care Plan for Tetralogy of Fallotanamika sharmaNo ratings yet
- Meddical Care Study Part 1Document48 pagesMeddical Care Study Part 1christyNo ratings yet
- Nursing Careplan Lung CancerDocument16 pagesNursing Careplan Lung Canceranamika sharma100% (2)
- JG College of Nursing: Sub: Medical-Surgical NursingDocument33 pagesJG College of Nursing: Sub: Medical-Surgical NursingmilcahNo ratings yet
- COPDDocument22 pagesCOPDOM BAWNENo ratings yet
- Jaundice Case Study Nursing ManagementDocument30 pagesJaundice Case Study Nursing Managementkamini ChoudharyNo ratings yet
- Case Study On CopdDocument24 pagesCase Study On CopdPawan Batth67% (3)
- Diabetic NephropathyDocument49 pagesDiabetic NephropathyDhanya Raghu100% (1)
- Care Plan On OsteoarthritisDocument38 pagesCare Plan On OsteoarthritisPATEL NEHAKUMARI VIMALBHAINo ratings yet
- Oncology Health AssessmentDocument12 pagesOncology Health AssessmentHimani PatelNo ratings yet
- Patient Identification and Care PlanDocument8 pagesPatient Identification and Care Plananimesh panda100% (3)
- CARE PLAN FORMATDocument4 pagesCARE PLAN FORMATRoyster CabralNo ratings yet
- Process RecordingDocument9 pagesProcess RecordingShiva CharakNo ratings yet
- Patient Profile and History of Acute Coronary SyndromeDocument32 pagesPatient Profile and History of Acute Coronary SyndromenidhiNo ratings yet
- Practice Teaching ON Personality: Bhopal (M.P.)Document7 pagesPractice Teaching ON Personality: Bhopal (M.P.)amit100% (1)
- NCP On TuberculosisDocument23 pagesNCP On TuberculosisPreeti ChouhanNo ratings yet
- Health Assessment Peptic UlcerDocument13 pagesHealth Assessment Peptic UlcerHimani PatelNo ratings yet
- Observation Visit To NSDocument12 pagesObservation Visit To NSpriyaNo ratings yet
- Neurological AssessmentDocument5 pagesNeurological AssessmentVIDYANo ratings yet
- Introduction-:: Time Specific Objective Content Av AidsDocument7 pagesIntroduction-:: Time Specific Objective Content Av AidsDimpal ChoudharyNo ratings yet
- CARE PLAN On HyponatremiaDocument35 pagesCARE PLAN On Hyponatremia2020 MSc bhuvaneswari 05No ratings yet
- Case Presentation 1Document23 pagesCase Presentation 1Manisa ParidaNo ratings yet
- CASE STUDY ON CholelithiasisDocument20 pagesCASE STUDY ON CholelithiasisSimran ChauhanNo ratings yet
- Respiratory AssessmentDocument25 pagesRespiratory AssessmentchristyNo ratings yet
- Lesson Plan On Nursing Care of A Patient With Acute Renal FailureDocument17 pagesLesson Plan On Nursing Care of A Patient With Acute Renal FailurePriyanka NilewarNo ratings yet
- Care Plan Pneumonia CompressDocument18 pagesCare Plan Pneumonia CompressAahad AmeenNo ratings yet
- Observation Report CCU: Era University Era College of Nursing LucknowDocument7 pagesObservation Report CCU: Era University Era College of Nursing Lucknowarchana vermaNo ratings yet
- Unit Course MSC NursingDocument15 pagesUnit Course MSC NursingPriyanka JohnNo ratings yet
- Demostration of Wound DressingDocument10 pagesDemostration of Wound DressingDanish00rizviNo ratings yet
- B.Sc Nursing 2nd Year Medical Surgical Nursing I Question Paper DesignDocument2 pagesB.Sc Nursing 2nd Year Medical Surgical Nursing I Question Paper DesignS N K Kichha100% (1)
- Demographic and Medical History for 72Y Male Farmer with Bronchial AsthmaDocument26 pagesDemographic and Medical History for 72Y Male Farmer with Bronchial AsthmaKshayna 1234No ratings yet
- Prepared By: Athulya G Ii Year MSC Nursing Upasana College of Nursing KollamDocument25 pagesPrepared By: Athulya G Ii Year MSC Nursing Upasana College of Nursing KollamGayathri RNo ratings yet
- Nursing Management of Patients Occupational and Industrial DisordersDocument11 pagesNursing Management of Patients Occupational and Industrial DisordersNandini VermaNo ratings yet
- Drug StudyDocument10 pagesDrug StudyBandana RajpootNo ratings yet
- Teaching Practice on Malaria Diagnosis and ManagementDocument12 pagesTeaching Practice on Malaria Diagnosis and ManagementTopeshwar TpkNo ratings yet
- 8 Various Educational Committies FINALDocument12 pages8 Various Educational Committies FINALKALPANANo ratings yet
- Role of Regulatory Bodies: Major R Egulatory BodiesDocument9 pagesRole of Regulatory Bodies: Major R Egulatory BodiesSandhya s100% (1)
- Broncho Pnuemonia MEDICALDocument9 pagesBroncho Pnuemonia MEDICALArchana SahuNo ratings yet
- A Study To Evaluate Effectiveness of Cold Application and Magnesium Sulphate Application On Superficial Thrombophlebitis Among Patients Receiving Intravenous Therapy in Selected Hospitals Amritsar.Document25 pagesA Study To Evaluate Effectiveness of Cold Application and Magnesium Sulphate Application On Superficial Thrombophlebitis Among Patients Receiving Intravenous Therapy in Selected Hospitals Amritsar.Navjot Brar71% (14)
- Lesson Plan MSN 1Document14 pagesLesson Plan MSN 1SHREE SWAMINARAYAN NURSING COLLEGE CHIKHLINo ratings yet
- Case Study 1 AnginaDocument27 pagesCase Study 1 AnginaSantosh ChoudharyNo ratings yet
- Role Play and MicroteachingDocument25 pagesRole Play and MicroteachingPinki BarmanNo ratings yet
- Case Study On Transcardial RevascularizationDocument34 pagesCase Study On Transcardial RevascularizationAJ RAJANo ratings yet
- A Study On Knowledge and Perception Regarding Learning Disabilities in Children Among Primary School Teachers in Thiruvallur DistrictDocument5 pagesA Study On Knowledge and Perception Regarding Learning Disabilities in Children Among Primary School Teachers in Thiruvallur DistrictInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Demographic Data of The PatientDocument19 pagesDemographic Data of The Patientcharanjit kaurNo ratings yet
- Effectiveness of simulation-based CPR learning among studentsDocument29 pagesEffectiveness of simulation-based CPR learning among studentsenam professorNo ratings yet
- Procedure On Abdominal ParacentsisDocument22 pagesProcedure On Abdominal ParacentsisBhawna JoshiNo ratings yet
- LESSON PLAN ON INTRO TO AV AIDSDocument9 pagesLESSON PLAN ON INTRO TO AV AIDSAparna KinginiNo ratings yet
- Syllabus Auxiliary Nurse and Midwives: Indian Nursing CouncilDocument76 pagesSyllabus Auxiliary Nurse and Midwives: Indian Nursing CouncilDIVYA PATELNo ratings yet
- Syllabus BSC SemesterDocument238 pagesSyllabus BSC SemesterRAMZAAN EDUCATIONNo ratings yet
- Status Asthmaticus: Severe Persistent AsthmaDocument2 pagesStatus Asthmaticus: Severe Persistent Asthmahemaanandhy0% (1)
- Indira Gandhi School and College of Nursing Master Rotation Plan-2Nd Year GNM 2017-2018 (10Th Batch)Document4 pagesIndira Gandhi School and College of Nursing Master Rotation Plan-2Nd Year GNM 2017-2018 (10Th Batch)kuruvagadda sagar100% (1)
- Angina Pectoris Care PlanDocument18 pagesAngina Pectoris Care Planpslokesha84No ratings yet
- Complete Community Course Plan 2nd YearDocument6 pagesComplete Community Course Plan 2nd YearBabita DhruwNo ratings yet
- MSC Nursing Dissertation Synopsis: Era University LucknowDocument19 pagesMSC Nursing Dissertation Synopsis: Era University LucknowNazia GulzarNo ratings yet
- Assignment On Staffing Pattern of Nursing Education Sub: Nursing ManagementDocument6 pagesAssignment On Staffing Pattern of Nursing Education Sub: Nursing ManagementPrity DeviNo ratings yet
- Av Aids File - FINALDocument96 pagesAv Aids File - FINALNithya SannidhiNo ratings yet
- Betty Neuman'S Theory: Introduction About TheoristDocument11 pagesBetty Neuman'S Theory: Introduction About TheoristRenita ChrisNo ratings yet
- Tibial and Femur FactrueDocument25 pagesTibial and Femur Factruesingireddi1revathiNo ratings yet
- Tibial and Femur FactrueDocument25 pagesTibial and Femur Factruesingireddi1revathiNo ratings yet
- CommunicationDocument9 pagesCommunicationsingireddi1revathiNo ratings yet
- Course of Instruction Second Year B. SCDocument3 pagesCourse of Instruction Second Year B. SCsingireddi1revathiNo ratings yet
- Community Health Nursing ConceptsDocument14 pagesCommunity Health Nursing Conceptssingireddi1revathi100% (2)
- Medical Surgical NursingDocument31 pagesMedical Surgical Nursingsingireddi1revathi100% (3)
- VNSGU BSc Nursing program overviewDocument9 pagesVNSGU BSc Nursing program overviewsingireddi1revathiNo ratings yet
- SociologyDocument5 pagesSociologyRAJUNo ratings yet
- Pharmacology Course for Nursing StudentsDocument15 pagesPharmacology Course for Nursing Studentssingireddi1revathi100% (2)
- Pathology and GeneticsDocument11 pagesPathology and Geneticssingireddi1revathiNo ratings yet
- Final Infection Contro AssignementDocument24 pagesFinal Infection Contro Assignementsingireddi1revathiNo ratings yet
- SociologyDocument5 pagesSociologyRAJUNo ratings yet
- SociologyDocument5 pagesSociologyRAJUNo ratings yet
- Counseling 2Document39 pagesCounseling 2singireddi1revathiNo ratings yet
- Pathology and GeneticsDocument11 pagesPathology and Geneticssingireddi1revathi33% (3)
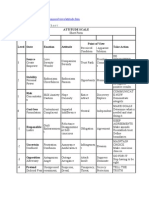
- Attitude ScaleDocument51 pagesAttitude Scalesingireddi1revathi100% (3)
- Acute Kidney Failure OverviewDocument13 pagesAcute Kidney Failure Overviewsingireddi1revathiNo ratings yet
- An Introduction To Alternative and Complementary MedicineDocument13 pagesAn Introduction To Alternative and Complementary Medicinesingireddi1revathiNo ratings yet
- LP Science WeatheringDocument4 pagesLP Science WeatheringHazel L Ibarra100% (1)
- Standard JKR Spec For Bridge LoadingDocument5 pagesStandard JKR Spec For Bridge LoadingHong Rui ChongNo ratings yet
- AllareDocument16 pagesAllareGyaniNo ratings yet
- Multicolor Fluorochrome Laser Chart PDFDocument1 pageMulticolor Fluorochrome Laser Chart PDFSathish KumarNo ratings yet
- Basic Electronic ComponentsDocument28 pagesBasic Electronic ComponentsJafar ShaikhNo ratings yet
- wizBRAINeng20 2Document4 pageswizBRAINeng20 2Deepika AgrawalNo ratings yet
- ANNEX III-Site Components Drawings SetDocument96 pagesANNEX III-Site Components Drawings SetDenice Erika ManzanoNo ratings yet
- Template Project Approach QuestionnaireDocument1 pageTemplate Project Approach QuestionnaireSara AliNo ratings yet
- Semiconductor Optical AmplifierDocument40 pagesSemiconductor Optical AmplifierVikas ThakurNo ratings yet
- Database AwsDocument15 pagesDatabase AwsHareesha N GNo ratings yet
- IM PS Fashion-Business-Digital-Communication-And-Media 3Y Course Pathway MI 04Document7 pagesIM PS Fashion-Business-Digital-Communication-And-Media 3Y Course Pathway MI 04oliwia bujalskaNo ratings yet
- XII Class Assignment Programs 2023-24Document8 pagesXII Class Assignment Programs 2023-24Sudhir KumarNo ratings yet
- Challenges Faced by Irregular StudentsDocument13 pagesChallenges Faced by Irregular StudentsTicag Teo80% (5)
- Omega: Mahdi Alinaghian, Nadia ShokouhiDocument15 pagesOmega: Mahdi Alinaghian, Nadia ShokouhiMohcine ES-SADQINo ratings yet
- SHSHA Report PresentationDocument27 pagesSHSHA Report PresentationPatrick JohnsonNo ratings yet
- Art for Ages 1-3 Focuses on DevelopmentDocument3 pagesArt for Ages 1-3 Focuses on DevelopmentPresley AbrauNo ratings yet
- Boston Globe Article - Jonnie Williams & Frank O'DonnellDocument3 pagesBoston Globe Article - Jonnie Williams & Frank O'DonnellFuzzy PandaNo ratings yet
- The Neuroscience of Autism Spectrum DisordersDocument10 pagesThe Neuroscience of Autism Spectrum DisorderssouciNo ratings yet
- Filipino Nationalism LessonDocument24 pagesFilipino Nationalism LessonIan Jay TumulakNo ratings yet
- 1675.does Concrete Lighten or Change Color As It DriesDocument5 pages1675.does Concrete Lighten or Change Color As It DriestvrNo ratings yet
- My Demo DemoDocument19 pagesMy Demo DemoAlex LopezNo ratings yet
- Jurnal Mira FixDocument16 pagesJurnal Mira Fixarisanto micoNo ratings yet
- 1 Catalyst FundamentalsDocument17 pages1 Catalyst FundamentalsSam AnuNo ratings yet
- STAR GLASS - D66f5e - PDFDocument126 pagesSTAR GLASS - D66f5e - PDFJessie O.BechaydaNo ratings yet
- New Balance Case StudyDocument3 pagesNew Balance Case StudyDimas AdityaNo ratings yet
- Asc2104b-T I enDocument21 pagesAsc2104b-T I enELOUNDOU EVARISTE OHANDJANo ratings yet
- R4850G2 Rectifier Data Sheet 05Document2 pagesR4850G2 Rectifier Data Sheet 05PP CharlyNo ratings yet
- Agile Spotify - Team - HomeworkDocument8 pagesAgile Spotify - Team - Homeworksp76rjm7dhNo ratings yet
- Segmentation: NIVEA Sun Case Study Summary Downloaded From The Times 100 Edition 11Document2 pagesSegmentation: NIVEA Sun Case Study Summary Downloaded From The Times 100 Edition 11Boon-Pin NgNo ratings yet