You might also like
- @anesthesia - Books 2015 Basic Physiology For Anaesthetists PDFDocument455 pages@anesthesia - Books 2015 Basic Physiology For Anaesthetists PDFovi67% (3)
- Ob Nursing Care Plan For Maternal Database Maternal and NewbornDocument2 pagesOb Nursing Care Plan For Maternal Database Maternal and Newbornapi-403051801No ratings yet
- Assessments of NewbornDocument8 pagesAssessments of NewbornYashoda SatputeNo ratings yet
- Overview Next Week WorkoutsDocument26 pagesOverview Next Week WorkoutsAngel TaverasNo ratings yet
- Kode Icd 10 Kasus BedahDocument6 pagesKode Icd 10 Kasus BedahYeye'sNo ratings yet
- Case Presentation On Pharyngitis2Document10 pagesCase Presentation On Pharyngitis2kamini ChoudharyNo ratings yet
- Delhi Nursing CouncilDocument13 pagesDelhi Nursing CouncilYASHA singhNo ratings yet
- Jaundice Case Study Nursing ManagementDocument30 pagesJaundice Case Study Nursing Managementkamini ChoudharyNo ratings yet
- Era University / Era College of Nursing: Lesson Plan On-Breast GynecomastiaDocument8 pagesEra University / Era College of Nursing: Lesson Plan On-Breast GynecomastiaShreya SinhaNo ratings yet
- ANTENATAL CARE Translate GooglingDocument26 pagesANTENATAL CARE Translate GooglingLutfi ari206100% (2)
- Hyperthermia NCPDocument1 pageHyperthermia NCPVenus Glaze VerzolaNo ratings yet
- N Research 06.05.2020 Graphical Representation of DataDocument50 pagesN Research 06.05.2020 Graphical Representation of DataBalasakthiNo ratings yet
- JG College of Nursing: Sub: Medical-Surgical NursingDocument33 pagesJG College of Nursing: Sub: Medical-Surgical NursingmilcahNo ratings yet
- Varicose VainsDocument28 pagesVaricose Vainssingireddi1revathi100% (1)
- Lesson Plan EbpDocument12 pagesLesson Plan EbpSwati Sharma100% (2)
- Care Plan On: Submitted To: Submitted byDocument38 pagesCare Plan On: Submitted To: Submitted byMoonNo ratings yet
- A Study To Evaluate The Effectiveness of Massaging of Foot On The Level of Pain Among Post-Operative Patient at Selected Hospital of BadamiDocument4 pagesA Study To Evaluate The Effectiveness of Massaging of Foot On The Level of Pain Among Post-Operative Patient at Selected Hospital of BadamiInternational Journal of Innovative Science and Research TechnologyNo ratings yet
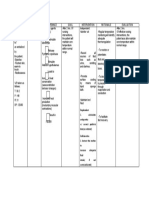
- Nursing care plan assessment, diagnosis, planning, implementation and evaluationDocument7 pagesNursing care plan assessment, diagnosis, planning, implementation and evaluationshweta singhNo ratings yet
- Pooja FinalDocument35 pagesPooja FinalSagar ChiplunkarNo ratings yet
- Newborn Osce Checklist: A. For StudentsDocument2 pagesNewborn Osce Checklist: A. For Studentsshubham vermaNo ratings yet
- Process RecordingDocument9 pagesProcess RecordingShiva CharakNo ratings yet
- Case Study of Renal FailurDocument15 pagesCase Study of Renal FailurYousef Jafar0% (1)
- Breast Exam Checklist UCC School of MedicineDocument2 pagesBreast Exam Checklist UCC School of Medicinehector100% (1)
- Nursing Care Plan for Tetralogy of FallotDocument17 pagesNursing Care Plan for Tetralogy of Fallotanamika sharmaNo ratings yet
- Final Hernioplasty Compilation RevisedDocument58 pagesFinal Hernioplasty Compilation RevisedRaidis PangilinanNo ratings yet
- Enteric FeverDocument30 pagesEnteric FeverShivam MalikNo ratings yet
- Oxygen TherapyDocument3 pagesOxygen TherapyKristina PingolNo ratings yet
- Syllabus BSC SemesterDocument238 pagesSyllabus BSC SemesterRAMZAAN EDUCATIONNo ratings yet
- Liceo de Cagayan University College of NursingDocument44 pagesLiceo de Cagayan University College of NursingMary SengNo ratings yet
- Lesson Plan On Nursing Care of A Patient With Acute Renal FailureDocument17 pagesLesson Plan On Nursing Care of A Patient With Acute Renal FailurePriyanka NilewarNo ratings yet
- ChemotherapyDocument11 pagesChemotherapyRekha G.No ratings yet
- lESSONPLAN FOR RETURN DEMODocument6 pageslESSONPLAN FOR RETURN DEMOJay PaulNo ratings yet
- Cholecystectomy Nursing Care Plan: Risk For InfectionDocument1 pageCholecystectomy Nursing Care Plan: Risk For InfectionBesael BaccolNo ratings yet
- Typhoid Fever 2010Document28 pagesTyphoid Fever 2010Earl John Natividad100% (3)
- A Study To Assess The Effectiveness of Foot Massage On The Level of Pain Among Post-Operative Patients at Dhanush Hospital BagalkotDocument7 pagesA Study To Assess The Effectiveness of Foot Massage On The Level of Pain Among Post-Operative Patients at Dhanush Hospital BagalkotInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- CataractDocument24 pagesCataractNeela Kandan100% (1)
- Diarrhea CPDocument8 pagesDiarrhea CPAsma SaleemNo ratings yet
- COPDDocument22 pagesCOPDOM BAWNENo ratings yet
- Prakash Institute of Physiotherapy Rehabilitation & Alllied Medical Sciences Master Rotation PlanDocument5 pagesPrakash Institute of Physiotherapy Rehabilitation & Alllied Medical Sciences Master Rotation Planvaishali TMU studentNo ratings yet
- Dengue Health TalkDocument20 pagesDengue Health TalkAnnamalai MNo ratings yet
- Medical Surgical Nursing Course PlanDocument10 pagesMedical Surgical Nursing Course PlanRanjana SharmaNo ratings yet
- Prepared By: Athulya G Ii Year MSC Nursing Upasana College of Nursing KollamDocument25 pagesPrepared By: Athulya G Ii Year MSC Nursing Upasana College of Nursing KollamGayathri RNo ratings yet
- Microteaching Education-1Document13 pagesMicroteaching Education-1Topeshwar TpkNo ratings yet
- Patient Case StudyDocument26 pagesPatient Case StudyDinesh BanerjeeNo ratings yet
- A Descriptive Study To Assess The Knowledge Regarding Substance Abuse and Ill Effects Among P.U. Students in The Selected P.U. College of BagalkotDocument3 pagesA Descriptive Study To Assess The Knowledge Regarding Substance Abuse and Ill Effects Among P.U. Students in The Selected P.U. College of BagalkotInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- National Anaemia Prophylaxis Programme Reduces Maternal MortalityDocument15 pagesNational Anaemia Prophylaxis Programme Reduces Maternal MortalityAnkit TalujaNo ratings yet
- Cloudy Eyes and Blurred VisionDocument18 pagesCloudy Eyes and Blurred VisionJustin Faye VibarNo ratings yet
- Cardiac Rehab After CABGDocument31 pagesCardiac Rehab After CABGShefali SharmaNo ratings yet
- MHN, I (U), 6Document51 pagesMHN, I (U), 6akilaNo ratings yet
- St. Paul University Nursing Care PlansDocument6 pagesSt. Paul University Nursing Care PlansRoxanne MariÑas Delvo0% (1)
- Assignment On Pharamcological Aspects - BY KAMINI2Document9 pagesAssignment On Pharamcological Aspects - BY KAMINI2kamini ChoudharyNo ratings yet
- Puerperium Q ADocument2 pagesPuerperium Q AMae Rose Charlene MendozaNo ratings yet
- Danger Signs in NewbornDocument22 pagesDanger Signs in NewbornAbhirup BoseNo ratings yet
- Diarrhea: DefinitionDocument13 pagesDiarrhea: Definitionudaybujji100% (1)
- Pathophysiology On ArrhythmiaDocument34 pagesPathophysiology On ArrhythmiaYhr Yh100% (1)
- Diabetic NephropathyDocument49 pagesDiabetic NephropathyDhanya Raghu100% (1)
- Lesson Plan On CholelithiasisDocument12 pagesLesson Plan On CholelithiasisKaka SalvatoreNo ratings yet
- Assignment ON Educational Preparation For NursesDocument6 pagesAssignment ON Educational Preparation For NursesPoonam ThakurNo ratings yet
- Case Presentation On Parkinsonism 4th YearDocument27 pagesCase Presentation On Parkinsonism 4th YearArchanaNo ratings yet
- Complete Community Course Plan 2nd YearDocument6 pagesComplete Community Course Plan 2nd YearBabita DhruwNo ratings yet
- ALTERED BODY TEMPERATUREDocument10 pagesALTERED BODY TEMPERATUREMelvin VrNo ratings yet
- Angina Pectoris Care PlanDocument18 pagesAngina Pectoris Care Planpslokesha84No ratings yet
- Internal Medicine Cases PresentationsDocument68 pagesInternal Medicine Cases PresentationsEliudi Kituma100% (2)
- The BloodDocument24 pagesThe BloodKicki AnderssonNo ratings yet
- Unit 4Document38 pagesUnit 4Preeti ChouhanNo ratings yet
- Respiratory SystemDocument5 pagesRespiratory SystemPreeti ChouhanNo ratings yet
- Case Presentation 1 CopdDocument48 pagesCase Presentation 1 CopdPreeti ChouhanNo ratings yet
- Oral HygieneDocument2 pagesOral HygienePreeti ChouhanNo ratings yet
- Unit IXDocument10 pagesUnit IXPreeti ChouhanNo ratings yet
- Lesson Plan - OCDDocument6 pagesLesson Plan - OCDPreeti ChouhanNo ratings yet
- EpidemiologyDocument29 pagesEpidemiologyPreeti ChouhanNo ratings yet
- Unit 4Document38 pagesUnit 4Preeti ChouhanNo ratings yet
- Saras Dairy Visit ReportDocument12 pagesSaras Dairy Visit ReportPreeti ChouhanNo ratings yet
- Attitude-Scale-for-Mental-Illness-Pat ShermanDocument7 pagesAttitude-Scale-for-Mental-Illness-Pat ShermanPreeti ChouhanNo ratings yet
- A Study To Assess Knowledge and Attitude Towards Organ Donation Among Undergraduate Students From Selected Departments in North Campus ofDocument9 pagesA Study To Assess Knowledge and Attitude Towards Organ Donation Among Undergraduate Students From Selected Departments in North Campus ofDrPreeti Thakur ChouhanNo ratings yet
- College Rules and DisciplineDocument2 pagesCollege Rules and DisciplinePreeti ChouhanNo ratings yet
- UntitledDocument8 pagesUntitledPreeti ChouhanNo ratings yet
- Student Nurses Association (SNA) UnitDocument1 pageStudent Nurses Association (SNA) UnitPreeti ChouhanNo ratings yet
- Programme Outcome B.Sc. Nursing CourseDocument7 pagesProgramme Outcome B.Sc. Nursing CoursePreeti ChouhanNo ratings yet
- Midwifery & Obstetrical Nursing Assignment On: Submitted To-Submitted byDocument1 pageMidwifery & Obstetrical Nursing Assignment On: Submitted To-Submitted byPreeti ChouhanNo ratings yet
- ANC ModuleDocument103 pagesANC ModulePreeti ChouhanNo ratings yet
- Comfort DevicesDocument42 pagesComfort DevicesPreeti ChouhanNo ratings yet
- Admintrationofmedications1 Copy 181202173921Document186 pagesAdmintrationofmedications1 Copy 181202173921Karl RobleNo ratings yet
- About The CourseDocument3 pagesAbout The CoursePreeti ChouhanNo ratings yet
- Midwifery & Obstetrical Nursing Case Presentation ON: Submitted To-Submitted byDocument1 pageMidwifery & Obstetrical Nursing Case Presentation ON: Submitted To-Submitted byPreeti ChouhanNo ratings yet
- Midwifery & Obstetrical Nursing Demonstration ON: Submitted To-Submitted byDocument1 pageMidwifery & Obstetrical Nursing Demonstration ON: Submitted To-Submitted byPreeti ChouhanNo ratings yet
- Midwifery & obstetrical nursing demonstrationDocument1 pageMidwifery & obstetrical nursing demonstrationPreeti ChouhanNo ratings yet
- Nursing faculty boarding points and contactsDocument2 pagesNursing faculty boarding points and contactsPreeti ChouhanNo ratings yet
- List of Non-Stationary Requirments For Open House 2 Non StstionaryDocument1 pageList of Non-Stationary Requirments For Open House 2 Non StstionaryPreeti ChouhanNo ratings yet
- Perioperative Nursing Care for PatientsDocument50 pagesPerioperative Nursing Care for PatientsPreeti ChouhanNo ratings yet
- Medipulse Clinical Rotation Plan - B.SC (N) I - 2019Document1 pageMedipulse Clinical Rotation Plan - B.SC (N) I - 2019Preeti ChouhanNo ratings yet
- List of PublicationsDocument1 pageList of PublicationsPreeti ChouhanNo ratings yet
- Names of Individual TeethDocument6 pagesNames of Individual TeethLorena Rodríguez RodríguezNo ratings yet
- Thyroid Stimulating Hormone, SerumDocument1 pageThyroid Stimulating Hormone, SerumSATHISHKUMAR RNo ratings yet
- Case Management Physiotherapy Ischialgia Due to Lumbar Spondylosis L4 – L5Document15 pagesCase Management Physiotherapy Ischialgia Due to Lumbar Spondylosis L4 – L5Pantas SiburianNo ratings yet
- Quiz - Development of Human Cardiovascular SystemDocument7 pagesQuiz - Development of Human Cardiovascular Systemlucky mbaselaNo ratings yet
- Worksheet RULADocument1 pageWorksheet RULAAndrea Murillo0% (1)
- HISTOLO Lecture 4 - Histology of The Digestive SystemDocument37 pagesHISTOLO Lecture 4 - Histology of The Digestive SystemResty De Guzman SoteloNo ratings yet
- Structural Organization in Animals - Cell Organelle, Tissues, Organ System ADocument7 pagesStructural Organization in Animals - Cell Organelle, Tissues, Organ System AMohammad Ali Sikder RamimNo ratings yet
- The Skull3Document10 pagesThe Skull3Mokhtar SinanNo ratings yet
- Brachial PlexusDocument6 pagesBrachial PlexusMuhamad SdeqNo ratings yet
- G&DDocument20 pagesG&Dahead1234No ratings yet
- Physiology Essay 11: Sympathetic Nervous System in Stress ResponseDocument2 pagesPhysiology Essay 11: Sympathetic Nervous System in Stress ResponseNektarios TsakalosNo ratings yet
- Case Study Onhead InjuryDocument32 pagesCase Study Onhead InjurySaroj Kumar BeheraNo ratings yet
- Exercises For Peripheral Neuropathy: Patient EducationDocument6 pagesExercises For Peripheral Neuropathy: Patient EducationDerison MarsinovaNo ratings yet
- 8 Week In-Gym Training Program (9 Pages)Document9 pages8 Week In-Gym Training Program (9 Pages)Kristina HelmesNo ratings yet
- OrthodonticsDocument66 pagesOrthodonticsHady SpinNo ratings yet
- Physiology of HearingDocument30 pagesPhysiology of HearingDr Sravya M VNo ratings yet
- Abdominal Positioning in RadiographyDocument23 pagesAbdominal Positioning in RadiographykarehmanNo ratings yet
- Tutorial Presentation: Artika Mala (s170201) Week 2Document22 pagesTutorial Presentation: Artika Mala (s170201) Week 2Artika MalaNo ratings yet
- Anatomy and Physiology of Farm AnimalsDocument169 pagesAnatomy and Physiology of Farm AnimalsKRIZZAPEARL VER100% (1)
- Anatomy Physiology Pre Final ExamDocument4 pagesAnatomy Physiology Pre Final ExamFatima AsisNo ratings yet
- Ear Anatomy: OtolaryngologyDocument18 pagesEar Anatomy: OtolaryngologysafitriNo ratings yet
- Congenital Auricular Malformation: Dr. R. Isma Nurul A'IniDocument47 pagesCongenital Auricular Malformation: Dr. R. Isma Nurul A'Inithtkl irpNo ratings yet
- ICD 9 ProcedureDocument102 pagesICD 9 ProcedureChandra FerdianNo ratings yet
- Trigeminal Nerve: Nikita Sebastian Mds I Department of Conservative Dentistry and Endodontics JSSDCHDocument63 pagesTrigeminal Nerve: Nikita Sebastian Mds I Department of Conservative Dentistry and Endodontics JSSDCHNikita SebastianNo ratings yet
- Observations On: TibiaDocument5 pagesObservations On: TibiaJuned LabbaiNo ratings yet
- The Articulatory SystemDocument4 pagesThe Articulatory SystemDianne MaeNo ratings yet