Professional Documents
Culture Documents
Hepcidin and Ferritin Predict Microbial Etiology in Cap
Uploaded by
Youtube MaliaCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Hepcidin and Ferritin Predict Microbial Etiology in Cap
Uploaded by
Youtube MaliaCopyright:
Available Formats
Open Forum Infectious Diseases
Major Article
Hepcidin and Ferritin Predict Microbial Etiology in
Community-Acquired Pneumonia
Kjersti Oppen,1,2,3, Thor Ueland,2,3,4 William Ward Siljan,5 Øyvind Skadberg,6 Cato Brede,6,7 Trine Lauritzen,1 Pål Aukrust,2,3,4,8, Trude Steinsvik,1
Einar Husebye,10 Annika E Michelsen,2,3 Jan Cato Holter,3,9 and Lars Heggelund10,11
1
Department of Laboratory Medicine, Drammen Hospital, Vestre Viken Hospital Trust, Drammen, Norway, 2Research Institute of Internal Medicine, Oslo University Hospital Rikshospitalet, Oslo, Norway,
3
Institute of Clinical Medicine, University of Oslo, Oslo, Norway, 4Faculty of Health Sciences, K.G. Jebsen TREC, University of Tromsø, Tromsø, Norway, 5Division of Medicine, Akershus University Hospital,
Lørenskog, Norway, 6Department of Medical Biochemistry, Stavanger University Hospital, Stavanger, Norway, 7Department of Chemistry, Bioscience and Environmental Engineering, University of Stavanger,
Stavanger, Norway, 8Section of Clinical Immunology and Infectious Diseases, Oslo University Hospital Rikshospitalet, Oslo, Norway, 9Department of Microbiology, Oslo University Hospital, Oslo, Norway,
10
Department of Internal Medicine, Drammen Hospital, Vestre Viken Hospital Trust, Drammen, Norway, 11Department of Clinical Science, Bergen Integrated Diagnostic Stewardship Cluster, Faculty of
Medicine, University of Bergen, Bergen, Norway
Background. Iron is crucial for survival and growth of microbes. Consequently, limiting iron availability is a human antimicro-
bial defense mechanism. We explored iron and iron-related proteins as potential biomarkers in community-acquired pneumonia
and hypothesized that infection-induced changes in these potential biomarkers differ between groups of pathogens and could pre-
dict microbial etiology.
Methods. Blood samples from a prospective cohort of 267 patients with community-acquired pneumonia were analyzed for
hepcidin, ferritin, iron, transferrin, and soluble transferrin receptor at admission, clinical stabilization, and a 6-week follow-up.
A total of 111 patients with an established microbiological diagnosis confined to 1 microbial group (atypical bacterial, typical bacte-
rial, or viral) were included in predictive analyses.
Results. High admission levels of ferritin predicted atypical bacterial versus typical bacterial etiology (odds ratio [OR], 2.26;
95% confidence interval [CI], 1.18–4.32; P = .014). Furthermore, hepcidin and ferritin predicted atypical bacterial versus viral eti-
ology (hepcidin: OR = 3.12, 95% CI = 1.34–7.28, P = .008; ferritin: OR = 2.38, 95% CI = 1.28–4.45, P = .006). The findings were
independent of C-reactive protein and procalcitonin.
Conclusions. Hepcidin and ferritin are potential biomarkers of microbial etiology in community-acquired pneumonia.
Keywords: biomarkers; ferritin; hepcidin; iron; pneumonia.
Almost all organisms depend on iron to thrive, and the amount rapidly increase in response to inflammatory cytokines, partic-
of iron available to microbes affects survival and growth and, ularly interleukin 6 (IL-6) [4]. Still, how these opposing and
thus, their pathogenic potential [1]. The human immune converging signals are integrated to regulate hepcidin expres-
system has evolved various defense mechanisms to limit iron sion and maintain iron homeostasis is incompletely understood
availability, resulting in an evolutionary battle for iron between [3].
microbes and host. Systemic iron homeostasis is predominantly Hepcidin acts by inducing degradation of the ferroportin
orchestrated by hepcidin, a peptide hormone mainly produced iron transporter, causing iron entrapment intracellularly and
in the liver [2]. Production of hepcidin changes rapidly and restricting access of iron to various microbes [5]. This may
over a wide dynamic range in response to multiple stimuli [3]. inhibit replication of typical extracellular bacteria, but it may
Hepcidin is suppressed in response to increased physiological also provide a nutritional advantage for atypical bacteria with
iron requirements and, conversely, induced by increased iron intracellular growth [6]. Induction of hepcidin has also been
levels to prevent iron accumulation. In addition, as part of the demonstrated in viral infections, although the contribution to
inflammatory response to invading microbes, the hepcidin level pathogenesis is largely unknown [5]. Knowledge of the var-
ious mechanisms involved and the interplay between pathogen
and host is emerging, yet a comprehensive overview of the iron
Received 3 December 2020; editorial decision 10 February 2021; accepted 15 February 2021. metabolism during infections is lacking. Specific differences in
Correspondence: Kjersti Oppen, MD, Vestre Viken Hospital Trust, Dronninggata 28, 3004
Drammen, Norway (kjeopp@vestreviken.no).
host responses to pathogens need to be explored both on indi-
Open Forum Infectious Diseases®2021 vidual and group levels, including intracellular versus extracel-
© The Author(s) 2021. Published by Oxford University Press on behalf of Infectious Diseases lular pathogens [7].
Society of America. This is an Open Access article distributed under the terms of the Creative
Commons Attribution-NonCommercial-NoDerivs licence (http://creativecommons.org/licenses/
Whereas hepcidin is a key iron regulator in plasma, fer-
by-nc-nd/4.0/), which permits non-commercial reproduction and distribution of the work, in any ritin is the major iron storage protein and transferrin the
medium, provided the original work is not altered or transformed in any way, and that the
main iron transport protein. As transferrin in plasma ex-
work is properly cited. For commercial re-use, please contact journals.permissions@oup.com
DOI: 10.1093/ofid/ofab082 ceeds its iron binding capacity (assessed by transferrin
Iron and Microbial Etiology • ofid • 1
saturation; s-iron/s-total iron binding capacity), iron binds Patient Consent Statement
to citrate, other organic acids, and albumin, collectively All patients signed an informed consent form. The study was
termed nontransferrin-bound iron (NTBI) [8]. Cellular up- approved by the Regional Committee for Medical and Health
take of transferrin-bound iron is mediated by transferrin Research Ethics in South-Eastern Norway (reference number
receptor 1 via endocytosis according to cellular iron require- S-06266a) and registered in ClinicalTrials.gov (NCT01563315).
ments [9]. Serum levels of the soluble form (s-transferrin
receptor) are correlated to erytropoietic activity and tissue Data Collection and Definitions
iron content [10]. Clinical information was recorded on paper case records
During inflammation, various cytokines induce synthesis forms and extracted from medical records. All chest x-rays
of ferritin, particularly in macrophages [7, 11]. Increased were re-examined by an experienced study radiologist
iron storage as ferritin in these cells reduces the labile iron blinded to the clinical data. Microbial etiology was estab-
pool intracellularly, which is believed to reduce the growth lished through an extensive microbiological investigation
of intracellular pathogens. However, some pathogens have as described elsewhere [14] and categorized as pure typical
evolved strategies to overcome this defense mechanism [12]. bacterial, pure atypical bacterial, pure viral, mixed, or no es-
In addition, ferritin has been hypothesized to leak from tablished etiology. Pure etiology was defined as 1 or more
damaged cells during the inflammatory process, leading to pathogens identified within a particular group. Severity of ill-
higher systemic levels. Thus, it may serve as a marker of cel- ness was assessed by the clinical scoring tool CURB-65 (con-
lular damage [13]. fusion, urea, respiratory rate, blood pressure, age ≥65 years)
Because infections induce changes in levels of iron and iron- [15] and by intensive care unit (ICU) admissions during the
related proteins that may differ among groups of pathogens, we hospital stay. A CURB-65 score ≤2 was defined as low risk,
explored the ability of these potential biomarkers to predict mi- and a score ≥3 was defined as high risk. Further details are
crobial etiology as well as their temporal dynamics in a cohort available in previous publications [14, 16].
of hospitalized adult community-acquired pneumonia (CAP)
Sample Collection and Analysis
patients.
Blood samples were collected at admission (within 48 hours),
clinical stabilization, and 6-week follow-up. Serum was allowed
MATERIALS AND METHODS
to clot for at least 30 minutes, and further preparation of serum
In this prospective cohort, adults (≥18 years) with suspected and plasma was carried out within 60 minutes after sampling by
CAP admitted to Drammen hospital (Vestre Viken Hospital refrigerated centrifugation at 2000 ×g for 12 minutes. Several
Trust, Norway) were recruited over a 3-year period (January 1, aliquots were stored at −80°C.
2008–January 31, 2011). Analysis were performed on all samples given sufficient mate-
rial. Analysis of plasma hepcidin was performed by liquid chro-
Patient Selection and Design matography coupled with tandem mass spectrometry, which
Community-acquired pneumonia diagnosis was established selectively measures the biological active isoform of hepcidin,
based on the following criteria within the first 48 hours of ad- hepcidin-25. This method has been validated for clinical appli-
mission: (1) identification of a new pulmonary infiltrate on cations at Stavanger University Hospital (Stavanger, Norway)
chest x-ray, (2) rectal temperature ≥38.0°C, and (3) at least 1 according to Eurachem guidelines [17] and later revalidated
of the following: productive or nonproductive cough, dyspnea, as part of work in the Working Group on Clinical Quantitative
respiratory chest pain, crackles, or reduced respiratory sounds. Mass Spectrometry Proteomics of the International Federation
Discharge from hospital within 2 weeks before admission or of Clinical Chemistry. Samples used for hepcidin analysis had
x-ray findings of other noninfectious pulmonary disease led been through 1 freeze-thaw cycle before analysis. All samples
to exclusion. were handled equally, and differences in serum hepcidin over
Criteria for clinical stabilization were evaluated daily for the 4 freeze-thaw cycles have been reported to be of minor impor-
first 12 days upon admission. C-reactive protein (CRP) and tance [18]. An international standard for hepcidin is not yet
leucocytes were measured every second day. Clinical stabiliza- universally applied [19], hence comparisons between groups are
tion was defined by at least 3 of the following 4 criteria: (1) un- more relevant than the absolute values. Levels of CRP, ferritin,
changed antibiotic treatment the last 2 days, (2) improvement iron, and transferrin were all analyzed in serum on Architect
of general condition, (3) morning rectal temperature <38°C, ci16200 (Abbott Diagnostics, Abbott Park, IL). Serum soluble
and (4) >25% decrease in CRP levels or leucocyte count. The transferrin receptor was analyzed on BN ProSpec (Siemens
participants were invited to a 6-week follow-up including blood Healthineers, Marburg, Germany). Serum procalcitonin ([PCT]
sampling and a renewed chest x-ray. BRAHMS; Thermo Fisher Scientific, Hennigsdorf, Germany)
2 • ofid • Oppen et al
was analyzed on ADVIA Centaur (Siemens Healthineers, (ORs) with 95% confidence intervals (CIs). A 2-sided signifi-
Tarrytown, NY). C-reactive protein and PCT analysis are pre- cance level of 0.05 was used in all analysis. Statistical analysis was
viously reported [20]. HFE gene variants were detected by pol- performed using SPSS (version 25; IBM, Chicago, IL).
ymerase chain reaction amplification and melt curve analysis
on Lightcycler 480 (Roche Diagnostics, Oslo, Norway) using in RESULTS
vitro diagnostics kit from TIB MOLBIOL (Berlin, Germany).
A total of 267 patients ≥18 years admitted to hospital with sus-
pected CAP were included out of 320 screened patients as detailed
Data Analysis previously [14]. Median time from admission to clinical stabiliza-
Categorical data are presented as n (%). Normally distributed tion was 4 days (range, 1–72). Among the survivors at the 6-week
continuous variables are presented as mean (standard deviation), follow-up, 90% attended. For biomarker assessment, there were at
whereas skewed data are presented as median (25–75 percentile). the most 35, 61, and 43 missing values at admission, clinical stabi-
Multiple group comparisons were performed using one-way lization, and 6-week follow-up (missing due to deaths included).
analysis of variance for normally distributed continuous vari-
ables. Multiple groups of categorical data were compared (1) by Baseline Characteristics
Pearson χ 2 or (2) by Fisher’s exact test if the expected count was Baseline characteristics are presented according to microbial
<5 in >20% of the cells. Wilcoxon signed-rank test was used to etiology in Table 1, and an overview of the identified mi-
compare levels at admission and 6-week follow-up. In statistical crobes is provided in Supplementary Table 1. An etiological
analysis predicting microbial etiology, patients with unknown diagnosis was established in 167 patients (63%) in which 69
microbial etiology or copathogens across etiological groups were patients (41%) had more than 1 detected microbe, as previ-
excluded. Ln-transformation was applied to achieve normally ously published [14]. A total of 111 patients had 1 etiolog-
distributed variables for logistic regression analysis. Predictive ical diagnosis only, either pure typical bacterial, pure atypical
analysis was performed using bivariate logistic regression of the bacterial, or pure viral. Within the typical bacterial group,
ln-transformed, standardized variables to estimate odds ratios Streptococcus pneumoniae was detected in a majority of the
Table 1. Baseline Characteristics According to Microbial Etiology
All Patients Pure Typical Pure Atypical Pure Viral Mixedb No Established P
Characteristicsa (n = 267) Bacterial (n = 51) Bacterial (n = 19) (n = 41) (n = 56) Etiology (n = 100) Value
Demographics
Age in years, mean (SD) 64.4 (17.6) 64.7 (19.0) 55.5 (20.3) 66.5 (17.2) 63.3 (16.0) 63.6 (17.9) .18
Female gender, n (%) 127 (47.6) 26 (51.0) 8 (42.1) 20 (48.8) 24 (42.9) 49 (49.0) .90
Active smoker, n (%) 65 (24.4) 16 (32.0) 3 (15.8) 7 (17.1) 18 (32.1) 21 (21.0) .20
Nursing home resident, n (%) 4 (1.5) 1 (2.0) 0 2 (4.9) 0 1 (1.0) .34
Comorbid Conditions, n (%) 172 (64.4) 32 (62.7) 6 (31.6) 31 (75.6) 39 (69.6) 64 (64.0) .018
Cardiovascular diseasec 74 (27.7) 16 (31.4) 5 (26.3) 11 (26.8) 16 (28.6) 26 (26.0) .97
COPD 60 (22.5) 14 (27.5) 3 (15.8) 10 (24.4) 12 (21.4) 21 (21.0) .83
Immunocompromisedd 48 (18.0) 10 (19.6) 2 (10.5) 8 (19.5) 9 (16.1) 19 (19.0) .90
Autoimmune diseasee 34 (12.7) 10 (19.6) 0 4 (9.8) 7 (12.5) 13 (13.0) .26
Diabetes mellitus 33 (12.4) 6 (11.8) 1 (5.3) 7 (17.1) 9 (16.1) 10 (10.0) .56
Renal disease 32 (12.0) 6 (11.8) 2 (10.5) 4 (9.8) 11 (19.6) 9 (9.0) .42
Neurological diseasef 19 (7.1) 1 (2.0) 0 4 (9.8) 2 (3.6) 12 (12.0) .087
Dementia 15 (5.6) 4 (7.8) 2 (10.5) 2 (4.9) 1 (1.8) 6 (6.0) .47
Liver disease 4 (1.5) 1 (2.0) 0 0 1 (1.8) 2 (2.0) 1.00
Severity of Illness, n (%)
CURB-65 ≥3 97 (37.9) 17 (34.7) 8 (42.1) 14 (35.9) 24 (44.4) 34 (35.8) .81
ICU admission 48 (18.0) 7 (13.7) 5 (26.3) 7 (17.1) 9 (16.1) 20 (20.0) .74
Abbreviations: COPD, chronic obstructive pulmonary disease; CURB-65, confusion, urea, respiratory rate, blood pressure, age ≥65 years; ICU, intensive care unit; SD, standard deviation.
a
<5% missing data.
b
Mix of at least 2 of the groups: typical bacterial, atypical bacterial, and viral.
c
Heart failure, coronary heart disease, cerebrovascular disease, peripheral artery disease.
d
Primary or secondary immunodeficiency, active malignancy, immunosuppressive drugs.
e
Rheumatoid arthritis, systemic lupus erythematosus, inflammatory bowel disease, autoimmune hepatitis, Sjogren’s disease, psoriasis.
f
Central nervous disease, neuromuscular disease.
NOTE: Bold indicates P < .05.
Iron and Microbial Etiology • ofid • 3
patients (82%). The only significant difference between the ferritin: OR = 2.24, 95% CI = 1.29–3.89, P = .004) and a lower
etiological groups in baseline characteristics was the overall risk of viral etiology (hepcidin: OR = 0.53, 95% CI = 0.33–0.85,
count of comorbid conditions, with the lowest proportion in P = .009; ferritin: OR = 0.62, 95% CI = 0.39–0.97, P = .035).
the atypical bacterial group. We further explored predictive comparisons between single
etiological groups (Table 2). Ferritin had the ability to discrim-
Dynamics of Iron and Iron-Related Proteins During the Course of inate atypical bacterial from both typical bacterial and viral
Community-Acquired Pneumonia
etiology but not typical bacterial from viral etiology. Hepcidin
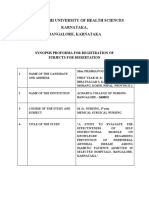
All potential biomarkers showed statistically significant differences
discriminated both atypical bacterial and typical bacterial eti-
in the acute-phase compared with the 6-week follow-up (Figure
ology from viral etiology but not between the 2 bacterial groups.
1). Whereas serum levels of iron, transferrin, transferrin satura-
In contrast, iron, transferrin saturation, and soluble transferrin
tion, and soluble transferrin receptor increased during follow-up,
receptor were not, or only modestly, associated with microbial
serum levels of hepcidin and ferritin were highest at admission
etiology of CAP.
(6.3- and 3.9-fold change compared with the 6-week follow-up).
Multivariate analysis with adjustment for CRP and PCT was
included, because these are the most studied biomarkers in clin-
Association Between the Potential Biomarkers and Microbial Etiology
ical use for this purpose [21]. Our main findings were largely
Comparing the 2 bacterial groups, admission levels of fer-
unchanged after adjustment for CRP and PCT in the logistic re-
ritin were significantly higher in patients with atypical bacte-
gression analysis (Table 2). However, the borderline significant
rial etiology (Figure 2). Both hepcidin and ferritin levels were
ability of hepcidin to discriminate between typical bacterial and
significantly higher in patients with atypical bacterial etiology
viral microbial etiology in univariate analysis did not sustain.
compared with viral etiology. Hepcidin levels were also higher
in typical bacterial etiology compared with viral etiology.
The ability of hepcidin and ferritin to predict microbial eti- Association Between the Potential Biomarkers and HFE Genotype
ology is displayed in Figure 3 by comparing 1 etiological group Because genetic variation in the HFE gene may influence
to the 2 other groups combined. High levels of both hepcidin levels of hepcidin and ferritin, we also analyzed 2 single-
and ferritin were associated with a higher risk of atypical bacte- nucleotide variants in the HFE gene, Cys282Tyr (C282Y)
rial etiology (hepcidin: OR = 2.12, 95% CI = 1.08–4.18, P = .030; and His63Asp (H63D), to assess the ability of the potential
A B C
150 800 20
***
Hepcidin, ng/L
600 15
Ferritin, μg/L
Iron, μmol/L
100
400 10
50
200 *** 5
***
Admission Clinical 6-week Admission Clinical 6-week Admission Clinical 6-week
stabilization follow-up stabilization follow-up stabilization follow-up
D E F
3 *** 30 2.0
Transferrin saturation, %
S-transferrin receptor,
***
***
Transferrin, g/L
1.5
2 20
mg/L
1.0
1 10
0.5
Admission Clinical 6-week Admission Clinical 6-week Admission Clinical 6-week
stabilization follow-up stabilization follow-up stabilization follow-up
Figure 1. Levels of iron and iron-related proteins during the course of pneumonia. Data are shown as median and 25–75 percentiles. Comparison of level at admission and
6-week follow-up by Wilcoxon signed-rank test. ***, P < .001. Reference ranges in parenthesis: (A) hepcidin (morning levels; women, <0.3–32 ng/mL; men, 0.9–34 ng/mL);
(B) ferritin (women, 15–200 μg/L; men, 30–400 μg/L); (C) iron (9–34 µmol/L); (D) transferrin (2.0–3.3 g/L); (E) transferrin saturation (women 18–49 years, 10%–50%; women
≥50 years, 15%–50%; men, 15%–57%); (F) soluble transferrin receptor (0.76–1.76 mg/L).
4 • ofid • Oppen et al
A 300 Typical bacterial vs. viral* B 2000 * **
**
Hepcidin, ng/mL
1500
Ferritin, μg/L
200
1000
100
500
0 0
Typical Atypical Viral Typical Atypical Viral
bacterial bacterial bacterial bacterial
Figure 2. Levels of iron and iron-related proteins at admission according to microbial etiology. Data are displayed as median and 25–75 percentile. Two-group comparison
by Mann-Whitney U test. *, P < .05; **, P < .01. (A) Hepcidin; (B) ferritin.
biomarkers to predict HFE genotype during acute-phase ferritin showed predictive power of atypical bacterial versus
pneumonia (Supplementary Table 2). Increased levels of viral etiology.
serum iron and transferrin saturation were associated with The battle for iron between microbes and host is multifac-
the 7 cases of potential disease-related genotypes: C282Y/ eted, and on an individual level, microbes utilize different strat-
C282Y and C282Y/H63D. However, we did not find any as- egies to extract iron [22]. The host strategies for withholding
sociation between hepcidin or ferritin levels and the most iron and their effect also vary depending on the intra- or extra-
common heterozygous HFE genotypes, C282Y/WT and cellular location of the microbes. The increased levels of ferritin
H63D/WT. and hepcidin in atypical bacterial pneumonia in our study are
novel observations, supporting diverse mechanisms of iron reg-
ulation depending on pathogen category.
DISCUSSION
Increased levels of hepcidin is theoretically an indirect
All potential biomarkers changed profoundly during the course measure of intracellular iron entrapment, which has been
of acute-phase pneumonia, reflecting a high degree of systemic shown to promote intracellular pathogen survival and growth
inflammation. As expected, serum iron and transferrin satu- in vitro [6], a finding supported by studies of cultured macro-
ration were low in the acute phase compared with the 6-week phages [23]. On the other hand, mice studies indicate a
follow-up, and they were far below the lower reference limits. pathogen-induced downregulation of ferroportin expression
These findings are consistent with, and probably due to, the independent of hepcidin and iron levels [24], and that ele-
increase of the main iron regulatory hormone hepcidin [2]. vated hepcidin levels may not promote intracellular infections
Indeed, both hepcidin and ferritin showed an opposite pattern [25]. Possible explanations of such hepcidin-independent in-
with the highest levels at admission. volvement are specific microbe-induced iron regulation, or a
A major finding of this explorative study was that admis- compartmentalization of iron within the macrophages, thus
sion levels of ferritin predicted atypical bacterial versus typical restricting iron access to intracellular pathogens [8]. Although
bacterial etiology. Furthermore, levels of both hepcidin and hepcidin is mainly produced in the liver, mice studies suggest
ferritin were particularly higher in atypical bacterial etiology that infection can induce a peripheral hepcidin production by
compared with viral etiology. Accordingly, both hepcidin and leukocytes, macrophages, and monocytes similar to ferritin that
A 0.53**
B 0.62*
Viral Viral
Typical bacterial Typical bacterial
2.12* 2.24**
Atypical bacterial Atypical bacterial
0.1 1 10 0.1 1 10
Hepcidin; OR (95% CI), log scale Ferritin; OR (95% CI), log scale
Figure 3. Forest plots; each etiological group is compared with the other 2 groups. Odds ratios (ORs) are calculated on basis of ln-transformed and standardized values. *,
P < .05; **, P < .01. (A) Hepcidin; (B) ferritin. CI, confidence interval.
Iron and Microbial Etiology • ofid • 5
may influence iron availability locally [26–28], but not neces-
0.97 (0.57–1.66), .91
0.88 (0.55–1.43), .62
0.92 (0.59–1.44), .71
1.16 (0.65–2.06), .62
1.03 (0.63–1.70), .90
1.07 (0.68–1.69), .76
sarily change systemic hepcidin levels and iron balance [29]. In
Multivariatea
general, local regulation may differ considerably from the sys-
NA
NA
temic effects assessed by measurement of biomarkers in serum
Typical Bacterial vs Viral [7]. Because iron is tightly bound to transferrin throughout the
OR (95% CI), P Value physiological concentration range, it has been argued that the
primary defense mechanism of hepcidin induction during in-
1.68 (1.01–2.77), .044
fection is mainly to prevent NTBI formation that may occur due
0.68 (0.44–1.05), .079
1.51 (1.01–2.24), .043
2.24 (1.41–3.56), .001
1.35 (0.84–2.17), .21
0.78 (0.51–1.21), .27
0.73 (0.48–1.10), .13
0.94 (0.62–1.42), .76
to infection-related destruction of tissue and erythrocytes [25].
Nontransferrin-bound iron comprises a heterogeneous group
Univariate
of iron species that may be more easily utilizable to pathogens
than transferrin-bound iron and may enhance growth of some
microbes [25]. Thus, in addition to withholding iron from
invading microbes, the hepcidin response during infection may
protect the host from toxic effects of NTBI [1]. Furthermore,
in vitro evidence of direct antimicrobial effects of hepcidin has
3.22 (1.20–8.64), .020
2.41 (1.15–5.02), .019
0.97 (0.51–1.85), .93
0.70 (0.35–1.38), .30
0.55 (0.26–1.17), .12
0.74 (0.35–1.56), .43
been demonstrated, but supporting evidence in vivo in humans
Multivariatea
are yet sparse [5]. Finally, we can only speculate whether the
NA
NA
hepcidin levels were elevated before or as a consequence of
atypical bacterial pneumonia. High baseline hepcidin levels
Atypical Bacterial vs Viral
OR (95% CI), P Value
may theoretically promote atypical bacterial infections.
Because hyperferritinemia may be cytokine-induced or related
to cellular damage [11, 13], the degree of cellular damage in pneu-
monia as well as the preferred intracellular or extracellular site of
3.12 (1.34–7.28), .008
2.38 (1.28–4.45), .006
0.50 (0.26–0.99), .045
0.86 (0.47–1.60), .64
0.79 (0.42–1.46), .45
1.39 (0.80–2.42), .25
1.04 (0.59–1.85), .89
0.62 (0.31–1.23), .17
infection may be important. Hypothetically, the higher level of fer-
Table 2. Prediction of Microbial Etiology by Logistic Regression of Admission Levels of Potential Biomarkers
Univariate
ritin in atypical bacterial infections could be related to a more pro-
found cellular damage in this group or be linked to its intracellular
location. Atypical bacterial infections also differ from other bac-
terial infections of the lung by the prevalence of extrapulmonary
manifestations [30], and ferritin leakage due to secondary organ
involvement may contribute to elevated ferritin levels.
NOTES: ORs are calculated on basis of ln-transformed and standardized values. Bold indicates P < .05.
It should be noted that the term atypical bacteria is not a
3.50 (1.42–8.61), .006
2.64 (0.99–7.02), .053
0.71 (0.34–1.48), .37
0.83 (0.44–1.57), .57
0.84 (0.44–1.57), .58
1.07 (0.59–1.93), .83
clearly defined entity [31–33]. The pathogens we included as
Abbreviations: CI, confidence interval; CRP, C-reactive protein; NA, not applicable; OR, odds ratio.
Multivariatea
atypical bacteria in this study are either predominantly intra-
Atypical Bacterial vs Typical Bacterial
NA
NA
cellular (Legionella pneumophila, Mycoplasma pneumoniae,
Chlamydia pneumoniae) [34] or there is evidence of some de-
OR (95% CI), P Value
gree of intracellular involvement (Bordetella pertussis) [35]. To
complicate this distinction, the most common CAP pathogen
S pneumoniae may also occasionally reside intracellularly [36].
2.26 (1.18–4.32), .014
0.46 (0.25–0.84), .011
Nevertheless, we believe that our categorization is sound, and
0.87 (0.50–1.52), .63
0.83 (0.48–1.45), .52
0.94 (0.54–1.65), .83
1.16 (0.67–1.98), .60
0.92 (0.59–1.45), .73
1.64 (0.82–3.28), .16
we hypothesize that a key point to the particularly increased
Univariate
levels of hepcidin and ferritin in atypical pneumonia is their
dominant intracellular pathophysiology. Viruses are obligate
intracellular, but, unlike atypical bacteria, their reproduction
relies entirely on the machinery of the host cells [37]. Although
Adjusted for CRP and procalcitonin.
the pathophysiological mechanisms resulting in the measured
levels of hepcidin and ferritin have yet to be detailed, the finding
S-Transferrin receptor
Transferrin saturation
of lower hepcidin and ferritin levels among patients with viral
Levels at Admission
pneumonia compared with atypical bacterial pneumonia sug-
Procalcitonin
gest that there are differences in the iron-related immune re-
Transferrin
Hepcidin
sponse between these intracellular pathogen groups that should
Ferritin
CRP
Iron
be further explored.
a
6 • ofid • Oppen et al
More importantly, the abilities of hepcidin and ferritin to in interpretation of the data. K. O. and L. H. drafted the manuscript. All
authors revised it critically for important intellectual content and approved
discriminate between atypical bacterial and viral pneumonia
the final version
were independent of CRP and PCT. Indeed, neither CRP nor Financial support. Siemens Healthineers provided reagent kits for
PCT discriminated between atypical bacterial and viral causes. s-transferrin receptor analysis.
However, as expected, CRP discriminated typical bacterial Potential conflicts of interest. All authors: No reported conflicts of in-
terest. All authors have submitted the ICMJE Form for Disclosure of
from viral etiology, although by a lower odds ratio than what Potential Conflicts of Interest.
we found for hepcidin and ferritin in predicting atypical bac-
terial etiology. Otherwise, CRP failed to separate the etiolog-
References
ical groups. Compared with CRP, PCT showed a better ability 1. Ganz T, Nemeth E. Iron homeostasis in host defence and inflammation. Nat Rev
to discriminate between viral and typical bacterial causes. The Immunol 2015; 15:500–10.
2. Sangkhae V, Nemeth E. Regulation of the iron homeostatic hormone hepcidin.
use of a combination of iron-related and traditional inflamma-
Adv Nutr 2017; 8:126–36.
tory biomarkers may be a future strategy to predict microbial 3. Sangkhae V, Nemeth E. To induce or not to induce: the fight over hepcidin regu-
etiology. Because there were no differences in CURB-65 or ICU lation. Haematologica 2019; 104:1093–5.
4. Girelli D, Nemeth E, Swinkels DW. Hepcidin in the diagnosis of iron disorders.
admissions between the etiological groups, we do not believe Blood 2016; 127:2809–13.
that the differences in biomarker levels between etiological 5. Michels K, Nemeth E, Ganz T, Mehrad B. Hepcidin and host defense against in-
fectious diseases. PLoS Pathog 2015; 11:e1004998.
groups were related to disease severity. 6. Paradkar PN, De Domenico I, Durchfort N, et al. Iron depletion limits intracel-
Although comparative analyses show significant differences, lular bacterial growth in macrophages. Blood 2008; 112:866–74.
7. Nairz M, Dichtl S, Schroll A, et al. Iron and innate antimicrobial immunity-
the number of patients with an atypical bacterial infection in depriving the pathogen, defending the host. J Trace Elem Med Biol 2018;
the present study is limited. In addition, being a single-center 48:118–33.
8. Ganz T. Iron and infection. Int J Hematol 2018; 107:7–15.
study with specific inclusion and exclusion criteria, the external
9. Kawabata H. Transferrin and transferrin receptors update. Free Radic Biol Med
validity to other populations must be carefully considered. The 2019; 133:46–54.
microbial etiology of CAP was established through extensive 10. Harms K, Kaiser T. Beyond soluble transferrin receptor: old challenges and new
horizons. Best Pract Res Clin Endocrinol Metab 2015; 29:799–810.
microbiological investigations. Still, a definite etiological di- 11. Cullis JO, Fitzsimons EJ, Griffiths WJ, et al.; British Society for Haematology.
agnosis was not obtained for 37% of patients, and undetected Investigation and management of a raised serum ferritin. Br J Haematol 2018;
181:331–40.
copathogens may have biased the etiological groups. Larger 12. Parrow NL, Fleming RE, Minnick MF. Sequestration and scavenging of iron in
studies are needed to validate our findings, preferably with a infection. Infect Immun 2013; 81:3503–14.
13. Kell DB, Pretorius E. Serum ferritin is an important inflammatory disease marker,
power to distinguish between single pathogens as well as eti- as it is mainly a leakage product from damaged cells. Metallomics 2014; 6:748–73.
ological groups, because pathogens within the atypical bacte- 14. Holter JC, Müller F, Bjørang O, et al. Etiology of community-acquired pneumonia
and diagnostic yields of microbiological methods: a 3-year prospective study in
rial group may also be different. Finally, the statistical analyses
Norway. BMC Infect Dis 2015; 15:64.
in the present study are used to assess associations and cannot 15. Lim WS, van der Eerden MM, Laing R, et al. Defining community acquired pneu-
prove causal relationships. monia severity on presentation to hospital: an international derivation and valida-
tion study. Thorax 2003; 58:377–82.
16. Holter JC, Ueland T, Jenum PA, et al. Risk factors for long-term mortality after
CONCLUSIONS hospitalization for community-acquired pneumonia: a 5-year prospective fol-
low-up study. PLoS One 2016; 11:e0148741.
In this prospective cohort of CAP patients, high admission 17. Magnusson B, Örnemark U, (eds.). Eurachem Guide: The Fitness for Purpose
of Analytical Methods—A Laboratory Guide to Method Validation and Related
levels of ferritin and hepcidin were in particular associated with Topics. 2nd ed. 2014. Available from: http://www.eurachem.org
a higher risk of atypical bacterial etiology and a lower risk of 18. Kemna EH, Tjalsma H, Podust VN, Swinkels DW. Mass spectrometry-based
hepcidin measurements in serum and urine: analytical aspects and clinical impli-
viral etiology. Hepcidin and ferritin emerge as potential bio- cations. Clin Chem 2007; 53:620–8.
markers of microbial etiology in CAP. 19. Aune ET, Diepeveen LE, Laarakkers CM, et al. Optimizing hepcidin measure-
ment with a proficiency test framework and standardization improvement. Clin
Chem Lab Med 2020; 59:315–23.
Supplementary Data
20. Siljan WW, Holter JC, Michelsen AE, et al. Inflammatory biomarkers are associ-
Supplementary materials are available at Open Forum Infectious Diseases ated with aetiology and predict outcomes in community-acquired pneumonia:
online. Consisting of data provided by the authors to benefit the reader, results of a 5-year follow-up cohort study. ERJ Open Res 2019; 5:00014-2019.
the posted materials are not copyedited and are the sole responsibility 21. Savvateeva EN, Rubina AY, Gryadunov DA. Biomarkers of community-acquired
of the authors, so questions or comments should be addressed to the pneumonia: a key to disease diagnosis and management. Biomed Res Int 2019;
corresponding author. 2019:1701276.
22. Palmer LD, Skaar EP. Transition metals and virulence in bacteria. Annu Rev
Genet 2016; 50:67–91.
Acknowledgments 23. Chlosta S, Fishman DS, Harrington L, et al. The iron efflux protein ferroportin
We thank Ulla Helene Enger (Department of Laboratory Medicine, regulates the intracellular growth of Salmonella enterica. Infect Immun 2006;
Drammen Hospital, Vestre Viken Hospital Trust, Drammen, Norway) for 74:3065–7.
24. Willemetz A, Beatty S, Richer E, et al. Iron- and hepcidin-independent
technical assistance and guidance in the analysis of HFE gene variants.
downregulation of the iron exporter ferroportin in macrophages during salmo-
Author contributions. L. H., J. C. H., E. H., W. W. S., T. L., P. A., T. U., and
nella infection. Front Immunol 2017; 8:498.
K. O. conceptualized and designed the study. C. B., Ø. S., T. L., A. E. M., and 25. Stefanova D, Raychev A, Arezes J, et al. Endogenous hepcidin and its agonist me-
K. O. contributed to the acquisition of data. T. U. and K. O. performed sta- diate resistance to selected infections by clearing non-transferrin-bound iron.
tistical analysis. L. H., T. U., P. A., T. S., E. H., J. C. H., and K. O. were central Blood 2017; 130:245–57.
Iron and Microbial Etiology • ofid • 7
26. Motley ST, Morrow BJ, Liu X, et al. Simultaneous analysis of host and pathogen management of adult lower respiratory tract infections. Eur Respir J 2005;
interactions during an in vivo infection reveals local induction of host acute 26:1138–80.
phase response proteins, a novel bacterial stress response, and evidence of a host- 33. Mandell LA, Wunderink RG, Anzueto A, et al.; Infectious Diseases Society
imposed metal ion limited environment. Cell Microbiol 2004; 6:849–65. of America; American Thoracic Society. Infectious Diseases Society of
27. Peyssonnaux C, Zinkernagel AS, Datta V, et al. TLR4-dependent hepcidin America/American Thoracic Society consensus guidelines on the manage-
expression by myeloid cells in response to bacterial pathogens. Blood 2006; ment of community-acquired pneumonia in adults. Clin Infect Dis 2007;
107:3727–32. 44:S27–72.
28. Theurl I, Theurl M, Seifert M, et al. Autocrine formation of hepcidin induces iron 34. Cillóniz C, Torres A, Niederman M, et al. Community-acquired pneumonia re-
retention in human monocytes. Blood 2008; 111:2392–9. lated to intracellular pathogens. Intensive Care Med 2016; 42:1374–86.
29. Drakesmith H, Prentice AM. Hepcidin and the iron-infection axis. Science 2012; 35. Martín C, Etxaniz A, Uribe KB, et al. Adenylate cyclase toxin promotes bacterial
338:768–72. internalisation into non phagocytic cells. Sci Rep 2015; 5:13774.
30. Cunha BA. The atypical pneumonias: clinical diagnosis and importance. Clin 36. Subramanian K, Henriques-Normark B, Normark S. Emerging concepts in the
Microbiol Infect 2006; 12:12–24. pathogenesis of the Streptococcus pneumoniae: from nasopharyngeal colonizer to
31. Murdoch DR, Chambers ST. Atypical pneumonia–time to breathe new life into a intracellular pathogen. Cell Microbiol 2019; 21:e13077.
useful term? Lancet Infect Dis 2009; 9:512–9. 37. Eisenreich W, Rudel T, Heesemann J, Goebel W. How viral and intracellular bacte-
32. Woodhead M, Blasi F, Ewig S, et al.; European Respiratory Society; European rial pathogens reprogram the metabolism of host cells to allow their intracellular
Society of Clinical Microbiology and Infectious Diseases. Guidelines for the replication. Front Cell Infect Microbiol 2019; 9:42.
8 • ofid • Oppen et al
You might also like
- Pass PACES in Single AttemptDocument101 pagesPass PACES in Single AttemptSOMNATHNo ratings yet
- Clinical Obsessive Compulsive DisordersDocument231 pagesClinical Obsessive Compulsive DisordersKareem Helmy100% (2)
- Hepcidin, A Key Regulator of Iron Metabolism and Mediator of Anemia of InflammationDocument6 pagesHepcidin, A Key Regulator of Iron Metabolism and Mediator of Anemia of InflammationCesar Josué GarcíaNo ratings yet
- Impact of Folic Acid Supplementation On Ischemia Reperfusion-Induced Kidney Injury in Rats: Folic Acid Prophylactic Role RevisitedDocument13 pagesImpact of Folic Acid Supplementation On Ischemia Reperfusion-Induced Kidney Injury in Rats: Folic Acid Prophylactic Role RevisitedYounis AhmedNo ratings yet
- Impact of Chronic and Acute Inflammation On Extra - and Intracellular Iron Homeostasis (Ross, 2017)Document7 pagesImpact of Chronic and Acute Inflammation On Extra - and Intracellular Iron Homeostasis (Ross, 2017)Maria Luisa Sibajas ÁvilaNo ratings yet
- Review Sepsis CCM 2007Document9 pagesReview Sepsis CCM 2007Nicole MariaNo ratings yet
- Hepcidin Knockout Mice Fed With Iron Rich DietDocument9 pagesHepcidin Knockout Mice Fed With Iron Rich DietEduardo Henrique de Sousa SalvinoNo ratings yet
- Alterations of Lung Microbial Communities in Obese Allergic Asthma and Metabolic PotentialDocument18 pagesAlterations of Lung Microbial Communities in Obese Allergic Asthma and Metabolic PotentialMila KaniyaNo ratings yet
- The Role of Zinc in Antiviral ImmunityDocument15 pagesThe Role of Zinc in Antiviral ImmunityKhalifatul Aulia AsyuriyahNo ratings yet
- Anemia 2Document11 pagesAnemia 2Ajeng RetnoNo ratings yet
- Iron Biology, Immunology, Aging, and Obesity: Four Fields Connected by The Small Peptide Hormone HepcidinDocument16 pagesIron Biology, Immunology, Aging, and Obesity: Four Fields Connected by The Small Peptide Hormone HepcidinSagita DarmasariNo ratings yet
- Quercetin Alleviates Acute Kidney Injury by Inhibiting FerroptosisDocument13 pagesQuercetin Alleviates Acute Kidney Injury by Inhibiting Ferroptosisdiego.battiatoNo ratings yet
- Antioxidants 10 00186 PublishedDocument50 pagesAntioxidants 10 00186 PublishedPeter SuraiNo ratings yet
- The Hyperferritinemic Syndrome: Macrophage Activation Syndrome, Still 'S Disease, Septic Shock and Catastrophic Antiphospholipid SyndromeDocument11 pagesThe Hyperferritinemic Syndrome: Macrophage Activation Syndrome, Still 'S Disease, Septic Shock and Catastrophic Antiphospholipid SyndromeLUCIENE CRISTALDO ALBUQUERQUENo ratings yet
- The Role of Zinc in Antiviral Immunity: ReviewDocument15 pagesThe Role of Zinc in Antiviral Immunity: ReviewNandkumar ChinaiNo ratings yet
- Association of Pulmonary Tuberculosis With Increased Dietary IronDocument4 pagesAssociation of Pulmonary Tuberculosis With Increased Dietary Ironchuye alemayehuNo ratings yet
- Respiratory Infections Drive Hepcidin-MediatedDocument9 pagesRespiratory Infections Drive Hepcidin-MediatedMariaJesusWongNo ratings yet
- Anemie NDT2005Document6 pagesAnemie NDT2005Sherif ElkadyNo ratings yet
- CC 9290Document12 pagesCC 9290elektifppra2022No ratings yet
- Hepcidin The Gatekeeper of Iron in Malaria ResistanceDocument8 pagesHepcidin The Gatekeeper of Iron in Malaria ResistanceKIU PUBLICATION AND EXTENSIONNo ratings yet
- Nutrients 14 00132Document14 pagesNutrients 14 00132Gina CyinthiaNo ratings yet
- Blunted Hepcidin Response To Oral Iron Challenge in HFE Related He - 2007 - BlooDocument5 pagesBlunted Hepcidin Response To Oral Iron Challenge in HFE Related He - 2007 - BlooTareeqanwar MohammedNo ratings yet
- Eosinophils From A To Z: Lea Gigon - Timothée Fettrelet - Shida Yousefi - Dagmar Simon - Hans-Uwe SimonDocument37 pagesEosinophils From A To Z: Lea Gigon - Timothée Fettrelet - Shida Yousefi - Dagmar Simon - Hans-Uwe SimonywtmyxpezickztrkcfNo ratings yet
- Profound Gene Expression Changes in The Epithelial Monolayer of Active Ulcerative Colitis and Crohn's DiseaseDocument23 pagesProfound Gene Expression Changes in The Epithelial Monolayer of Active Ulcerative Colitis and Crohn's DiseaseYaumil ChoiriNo ratings yet
- Trace Elements in Blood of Leukemia PatientsDocument6 pagesTrace Elements in Blood of Leukemia PatientsMediterr J Pharm Pharm SciNo ratings yet
- Pubmed HecidinaDocument9 pagesPubmed HecidinaeddcitoNo ratings yet
- Ijms 23 05144 v2Document23 pagesIjms 23 05144 v2Yomara MuñozNo ratings yet
- 2020 Khan - Serum Copper, Ceruloplasmin, Iron, Transferrin LevDocument10 pages2020 Khan - Serum Copper, Ceruloplasmin, Iron, Transferrin LevPratyay HasanNo ratings yet
- Giammanco & Giammanco Selenium ThyroidDocument2 pagesGiammanco & Giammanco Selenium ThyroidMarco GiammancoNo ratings yet
- 1 s2.0 S2214623714000040 MainDocument7 pages1 s2.0 S2214623714000040 MainSagita DarmasariNo ratings yet
- Role of Hepcidin in Anemia of Chronic Disease in Rheumatoid ArthritisDocument6 pagesRole of Hepcidin in Anemia of Chronic Disease in Rheumatoid ArthritishelenaNo ratings yet
- Gene Expression of Adipokines and Inflammatory Cytokines in Peripheral Blood Mononuclear Cells of Obese DogsDocument7 pagesGene Expression of Adipokines and Inflammatory Cytokines in Peripheral Blood Mononuclear Cells of Obese DogsAna Luiza LeroyNo ratings yet
- A Saga of Hepcidin Anti-Microbial Effectiveness As Iron Acquisitor and Anemia Initiator in Mycobacterium Tuberculosis InfectionDocument7 pagesA Saga of Hepcidin Anti-Microbial Effectiveness As Iron Acquisitor and Anemia Initiator in Mycobacterium Tuberculosis InfectionidhaNo ratings yet
- Hepcidin Regulation of Iron TransportDocument5 pagesHepcidin Regulation of Iron TransportQistina SudarnotoNo ratings yet
- Op Tim IzationDocument17 pagesOp Tim IzationANo ratings yet
- Ferroptosis 2022Document13 pagesFerroptosis 2022Adrian ValenciaNo ratings yet
- Research Article: Prevalence, Predictive Factors, and Characteristics of Osteoporosis in Hyperthyroid PatientsDocument7 pagesResearch Article: Prevalence, Predictive Factors, and Characteristics of Osteoporosis in Hyperthyroid Patientsdek fafaNo ratings yet
- Research Article: Prevalence, Predictive Factors, and Characteristics of Osteoporosis in Hyperthyroid PatientsDocument8 pagesResearch Article: Prevalence, Predictive Factors, and Characteristics of Osteoporosis in Hyperthyroid PatientsMutiara DamayantiNo ratings yet
- Research Article: Prevalence, Predictive Factors, and Characteristics of Osteoporosis in Hyperthyroid PatientsDocument8 pagesResearch Article: Prevalence, Predictive Factors, and Characteristics of Osteoporosis in Hyperthyroid PatientsMutiara DamayantiNo ratings yet
- Microvascular Research: A 1 A 1 D F A A A C A C G B H e A CDocument10 pagesMicrovascular Research: A 1 A 1 D F A A A C A C G B H e A CPablo Tapia BatallaNo ratings yet
- Editorial: Editorial Current Drug Targets, 2007, Vol. 8, No. 4 491Document76 pagesEditorial: Editorial Current Drug Targets, 2007, Vol. 8, No. 4 491laraalvarenga5832No ratings yet
- Terraneo2014 PDFDocument10 pagesTerraneo2014 PDFYun AkbarNo ratings yet
- Camaschella 2017Document9 pagesCamaschella 2017Walter Jhon Delgadillo Arone0% (1)
- КАПСУЛИРУЕМСЯ, БРАТВАDocument33 pagesКАПСУЛИРУЕМСЯ, БРАТВААлексей КочетовNo ratings yet
- Serum Ferritin - Past, Present and FutureDocument21 pagesSerum Ferritin - Past, Present and FutureAleksandar KitanovskiNo ratings yet
- Cancer Related Anemia An Integrated Multitarget Approach and Lifestyle InterventionsDocument36 pagesCancer Related Anemia An Integrated Multitarget Approach and Lifestyle InterventionsChitra MeytarizqiNo ratings yet
- Allergy - 2023 - Gigon - Eosinophils From A To ZDocument37 pagesAllergy - 2023 - Gigon - Eosinophils From A To ZGhost11mNo ratings yet
- Jci 133 159941Document12 pagesJci 133 159941Dhivya l.sNo ratings yet
- The Role of Hepcidin in Iron MetabolismDocument10 pagesThe Role of Hepcidin in Iron MetabolismTatiana JalbaNo ratings yet
- Cloning & Transgenesis: ISSN: 2168-9849Document8 pagesCloning & Transgenesis: ISSN: 2168-9849FrontiersNo ratings yet
- Oxygen and Viruses: A Breathing Story: ReviewDocument4 pagesOxygen and Viruses: A Breathing Story: ReviewVedanthNo ratings yet
- Omega 3 Terapia COVID 19Document11 pagesOmega 3 Terapia COVID 19Carlos MendozaNo ratings yet
- Wilson Disease - at The Crossroads Between Genetics andDocument10 pagesWilson Disease - at The Crossroads Between Genetics andBarry SeeboNo ratings yet
- ChoiDocument19 pagesChoiLuciana RafaelNo ratings yet
- Antioxidants 11 00726 v3Document16 pagesAntioxidants 11 00726 v3boopathiraja.chinnasamyNo ratings yet
- 1 s2.0 0891584995000472 Main PDFDocument6 pages1 s2.0 0891584995000472 Main PDFMarliCurcioNo ratings yet
- Pi Is 1471491423003027Document2 pagesPi Is 1471491423003027maow2No ratings yet
- European Journal of Medicinal Chemistry: Aditya Sharma, Archana PanDocument11 pagesEuropean Journal of Medicinal Chemistry: Aditya Sharma, Archana PanDiego TulcanNo ratings yet
- And Rio Poulos 2006Document7 pagesAnd Rio Poulos 2006Richi VasquezNo ratings yet
- Nutrients 16 00850Document11 pagesNutrients 16 00850Vianey Rios CarbajalNo ratings yet
- Vitamin D Deficiency and Severity of Pneumonia in Indonesian ChildrenDocument14 pagesVitamin D Deficiency and Severity of Pneumonia in Indonesian ChildrenYoutube MaliaNo ratings yet
- The Impact of Blood Glucose On CapDocument8 pagesThe Impact of Blood Glucose On CapYoutube MaliaNo ratings yet
- Sars Cov 2 PathogenesisDocument15 pagesSars Cov 2 PathogenesisYoutube MaliaNo ratings yet
- Ferritin Procalcitonin Ratio in Covid and Bacterial PneumoniaDocument20 pagesFerritin Procalcitonin Ratio in Covid and Bacterial PneumoniaYoutube MaliaNo ratings yet
- Diagnosis Value of CRP in PneumoniaDocument6 pagesDiagnosis Value of CRP in PneumoniaYoutube MaliaNo ratings yet
- I. Nursing Process A. Assessment 1. Personal Data A. Demographic DataDocument6 pagesI. Nursing Process A. Assessment 1. Personal Data A. Demographic DataNicole Anne TungolNo ratings yet
- Acute Renal FailureDocument6 pagesAcute Renal FailureFrancine Kyle SusanoNo ratings yet
- General Practitioner - Neurology MCQsDocument20 pagesGeneral Practitioner - Neurology MCQsAsif Newaz100% (3)
- How Trumps Vaccines Prevent The Great Reset and Save HumanityDocument38 pagesHow Trumps Vaccines Prevent The Great Reset and Save Humanityrhizoma100% (1)
- Suppurative Lung Diseases.Document37 pagesSuppurative Lung Diseases.Salman KhanNo ratings yet
- Medication Guide Floxin (Flox In) (Ofloxacin) : Reference ID: 2910767Document7 pagesMedication Guide Floxin (Flox In) (Ofloxacin) : Reference ID: 2910767Eko YuliantoNo ratings yet
- Psoriasis JOADocument7 pagesPsoriasis JOAckchatNo ratings yet
- Pedi PN RISCDocument4 pagesPedi PN RISCRamo EdumNo ratings yet
- MCN MT 1Document23 pagesMCN MT 1Jekka Ann Dela CruzNo ratings yet
- FON Mcqs..-1Document2 pagesFON Mcqs..-1Rizwan EjazNo ratings yet
- Blood Bank UnitDocument9 pagesBlood Bank UnitMary CabalceNo ratings yet
- 1w72mlbDocument5 pages1w72mlbnandaaa aprilNo ratings yet
- Haines 2002Document3 pagesHaines 2002Basilharbi HammadNo ratings yet
- Redox Biology: Bernard Schmitt, Morgane Vicenzi, Catherine Garrel, Frédéric M. DenisDocument8 pagesRedox Biology: Bernard Schmitt, Morgane Vicenzi, Catherine Garrel, Frédéric M. Denisrocio fernandez san juanNo ratings yet
- Congenital SyphilisDocument15 pagesCongenital SyphilisAlejandraSevillaNo ratings yet
- Quiz 17 - Cancer-Emergencies-Toxicology Básicos e Intermedios (Hoja Alumno) CortoDocument3 pagesQuiz 17 - Cancer-Emergencies-Toxicology Básicos e Intermedios (Hoja Alumno) CortoCynthia Argüelles GuzmánNo ratings yet
- (ADA) Package Insert (CE)Document31 pages(ADA) Package Insert (CE)Sinari AlfatNo ratings yet
- Iron Deficiency Anaemia: LT Col Hamid Iqbal Fcps (Haem) CL Pathologist MH RawalpindiDocument32 pagesIron Deficiency Anaemia: LT Col Hamid Iqbal Fcps (Haem) CL Pathologist MH RawalpindiHamid IqbalNo ratings yet
- The ANA Test: All You Need To KnowDocument14 pagesThe ANA Test: All You Need To KnowJackeline DoigNo ratings yet
- 30 Types of Yoga Mudras & Their Significance To Health: MantrasDocument37 pages30 Types of Yoga Mudras & Their Significance To Health: MantrasSwami AbhayanandNo ratings yet
- Hematology Dissertation TopicsDocument6 pagesHematology Dissertation TopicsManchester100% (1)
- Literature ReviewDocument4 pagesLiterature Reviewapi-548908089No ratings yet
- Clinonc Assignment FinalDocument28 pagesClinonc Assignment Finalapi-633652323No ratings yet
- Final Synopsis Format Sample ACNDocument25 pagesFinal Synopsis Format Sample ACNAbhijit DasNo ratings yet
- Brintellix: What Is in This LeafletDocument5 pagesBrintellix: What Is in This LeafletFsNo ratings yet
- Acid-Base Balance Study GuideDocument2 pagesAcid-Base Balance Study GuideNoah ClevengerNo ratings yet
- Media Hypes Moderna's COVID Vaccine, Downplays Risks - Children's Health DefenseDocument10 pagesMedia Hypes Moderna's COVID Vaccine, Downplays Risks - Children's Health DefenseDMDONo ratings yet
- Fluoride Menace in OrissaDocument83 pagesFluoride Menace in OrissaProfessor PrabhatNo ratings yet