You might also like
- Assessment of KIRICARE - A Health Financing Strengthening Project in Kirinyaga, Kenya - Esbon GakuuDocument20 pagesAssessment of KIRICARE - A Health Financing Strengthening Project in Kirinyaga, Kenya - Esbon Gakuuesbon gakuuNo ratings yet
- The Philippine Public Health SystemDocument44 pagesThe Philippine Public Health SystemMark Johnuel DuavisNo ratings yet
- The Organization of Health Services PDFDocument4 pagesThe Organization of Health Services PDFbaihern24No ratings yet
- Telemedicine: International Group Institute For Information Industry Jan 2008Document30 pagesTelemedicine: International Group Institute For Information Industry Jan 2008Ted Chao100% (7)
- RHCF: Reaching Primary Healthcare To The Base of The PyramidDocument31 pagesRHCF: Reaching Primary Healthcare To The Base of The PyramidHensi ShethNo ratings yet
- Dva CardsDocument2 pagesDva Cardsjemarus86No ratings yet
- DOH DevolutionDocument91 pagesDOH Devolutionapi-3704562100% (12)
- Engaging Private Health Providers For TB Care and Prevention in Kirinyaga, Kenya - EsbonDocument12 pagesEngaging Private Health Providers For TB Care and Prevention in Kirinyaga, Kenya - Esbonesbon gakuuNo ratings yet
- Introduction+to+the+Health+System+2023 RPDocument42 pagesIntroduction+to+the+Health+System+2023 RPSibabalwe DlovasheNo ratings yet
- Delivery of Health Care Services in RuralDocument29 pagesDelivery of Health Care Services in RuralMahenurNo ratings yet
- HealthCareSysteminIndiaDocument34 pagesHealthCareSysteminIndiaMridula SaranNo ratings yet
- Performance Analysis of The Kirinyaga County Health System, Kenya - GAKUU EsbonDocument17 pagesPerformance Analysis of The Kirinyaga County Health System, Kenya - GAKUU Esbonesbon gakuuNo ratings yet
- Submitted By:-Shubhomita Shweta Suryansh SahilDocument57 pagesSubmitted By:-Shubhomita Shweta Suryansh SahilShweta SainiNo ratings yet
- Comparative Models of Healthcare System: Canada: Group 6ADocument13 pagesComparative Models of Healthcare System: Canada: Group 6AAnonymouscat100% (1)
- CHN NotesDocument16 pagesCHN Noteshoney requermeNo ratings yet
- Health System of CanadaDocument37 pagesHealth System of Canadaranjan kapaliNo ratings yet
- HSS FBO Report NigeriaDocument9 pagesHSS FBO Report NigeriaStevenNo ratings yet
- Second Sem Finals - CPH NotesDocument38 pagesSecond Sem Finals - CPH NotesZoe VigiliaNo ratings yet
- Nilkantha Muncipality PresentationsDocument56 pagesNilkantha Muncipality Presentationsradha poudelNo ratings yet
- Trends in Health Policies in Viet Nam To Promote Women's Sexual and Reproductive HealthDocument19 pagesTrends in Health Policies in Viet Nam To Promote Women's Sexual and Reproductive HealthADBI EventsNo ratings yet
- Fundamentals in Nursing-ReviewerDocument19 pagesFundamentals in Nursing-ReviewerAlthea DapasenNo ratings yet
- UK Experience in Managing NHS From A Public Policymanagement Perspective (GD2 10-05-17)Document40 pagesUK Experience in Managing NHS From A Public Policymanagement Perspective (GD2 10-05-17)Yofintya R.S.P.25No ratings yet
- Uhc Ra 11223Document8 pagesUhc Ra 11223deevoncNo ratings yet
- Hospital and Its OrganizationDocument16 pagesHospital and Its Organizationprathusha78% (9)
- 04 HEALTH CARE DELIVERY SYSTEM INDIA For CHODocument34 pages04 HEALTH CARE DELIVERY SYSTEM INDIA For CHOKailash Nagar100% (1)
- PerbincanganDocument69 pagesPerbincanganh78k3r0p0kNo ratings yet
- Presentation by DR NB DholakiaDocument23 pagesPresentation by DR NB DholakiaNishith DholakiaNo ratings yet
- Introduction to Community medicine อ.ชโนดม ICH1 2019Document105 pagesIntroduction to Community medicine อ.ชโนดม ICH1 2019محمدNo ratings yet
- De La Salle University Medical Center (Dlsumc) : Hospital AdministrationDocument1 pageDe La Salle University Medical Center (Dlsumc) : Hospital AdministrationFerl ElardoNo ratings yet
- Health Care Delivery System in Rural AreaDocument40 pagesHealth Care Delivery System in Rural AreaSantosh K YatnattiNo ratings yet
- Health Care Delivery System in India: By. Kailash NagarDocument34 pagesHealth Care Delivery System in India: By. Kailash NagarAbirajanNo ratings yet
- L-4 Public and Private Health System in IndiaDocument2 pagesL-4 Public and Private Health System in IndiaFilmy LandNo ratings yet
- ENTREPRENEURSHIPDocument20 pagesENTREPRENEURSHIPbananakyuNo ratings yet
- Intro To Healthcare and Ehealth in The Philippines: Kristine Mae P. Magtubo MD MPMDocument17 pagesIntro To Healthcare and Ehealth in The Philippines: Kristine Mae P. Magtubo MD MPMGlenice JoyNo ratings yet
- Principles of Primary Health CareDocument66 pagesPrinciples of Primary Health CareKailash Nagar100% (1)
- Healthcare in PakistanDocument1 pageHealthcare in Pakistanv64wvym7n4100% (1)
- UNIT - 2 Health Care Delivery SystemDocument177 pagesUNIT - 2 Health Care Delivery Systemraina menezesNo ratings yet
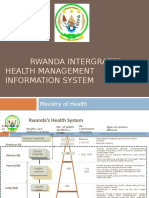
- Rwanda Intergrated Health Management Information SystemDocument11 pagesRwanda Intergrated Health Management Information SystemSanjeev ChouguleNo ratings yet
- FMCH - Doh Org ChartDocument22 pagesFMCH - Doh Org ChartLynx Kee BayatingNo ratings yet
- HCDSDocument87 pagesHCDSCarl LazaroNo ratings yet
- Health Care Delivery SystemDocument37 pagesHealth Care Delivery SystemMARICEL BAUTISTA MARAYAG100% (1)
- 1project Proposal Hospital of Tannu Jan Kalyan Seva SansthanDocument18 pages1project Proposal Hospital of Tannu Jan Kalyan Seva SansthanAVN TrustNo ratings yet
- Maternal Death Review A National PerspectiveDocument19 pagesMaternal Death Review A National PerspectivePrabir Kumar ChatterjeeNo ratings yet
- K-05 Diagnosis Holistik Dan Penatalaksanaan Komprehensif Pada Pelayanan Kesehatan PrimerDocument24 pagesK-05 Diagnosis Holistik Dan Penatalaksanaan Komprehensif Pada Pelayanan Kesehatan PrimerBobby AksandaNo ratings yet
- Telehealth June 2019Document62 pagesTelehealth June 2019MarcNo ratings yet
- Health Care System - StudentDocument43 pagesHealth Care System - StudentValerieNo ratings yet
- HSD Presentation UNIT-5Document45 pagesHSD Presentation UNIT-5Shumaila ArfinNo ratings yet
- 신 슬 주Document10 pages신 슬 주khimciNo ratings yet
- 2 Functions of Public HealthDocument26 pages2 Functions of Public HealthMoreiyamNo ratings yet
- Health Care Delivery Sysytem in India-2020Document46 pagesHealth Care Delivery Sysytem in India-2020Ratna KumariNo ratings yet
- Phil Health Care SystemDocument4 pagesPhil Health Care SystemERESTALL SENNDI GRACE OLIVERASNo ratings yet
- RA 11223 + F1 For HealthDocument3 pagesRA 11223 + F1 For HealthdeevoncNo ratings yet
- Health Care Delivery Sysytem in India-2020Document40 pagesHealth Care Delivery Sysytem in India-2020Sree LathaNo ratings yet
- Project ProposalDocument20 pagesProject ProposalROHAN JHANDANo ratings yet
- Health Care MarketingDocument84 pagesHealth Care Marketingshakya28sushilNo ratings yet
- Managed CareDocument20 pagesManaged Careapi-3743483No ratings yet
- S1 Etienne LangloisDocument11 pagesS1 Etienne LangloisCsu AlumniRelationsNo ratings yet
- Arinaa Medical Tourism OverviewDocument23 pagesArinaa Medical Tourism Overviewbhagavathi.muruganpillai6851No ratings yet
- Health Care SystemsDocument29 pagesHealth Care SystemsVerdah Sabih100% (2)
- The State of Pharmacoeconomic Evaluation Studies in Kenya - GAKUU EsbonDocument40 pagesThe State of Pharmacoeconomic Evaluation Studies in Kenya - GAKUU Esbonesbon gakuuNo ratings yet
- The Impact of Pricing and Affordability of Medicines On Access To Healthcare in Kenya - Gakuu EsbonDocument6 pagesThe Impact of Pricing and Affordability of Medicines On Access To Healthcare in Kenya - Gakuu Esbonesbon gakuuNo ratings yet
- The Burden of Schistosomiasis-A Kenyan Context - GAKUU EsbonDocument15 pagesThe Burden of Schistosomiasis-A Kenyan Context - GAKUU Esbonesbon gakuuNo ratings yet
- Strengthening Health Technology Assessment Systems in Kenya-Esbon GakuuDocument7 pagesStrengthening Health Technology Assessment Systems in Kenya-Esbon Gakuuesbon gakuuNo ratings yet
- Performance Analysis of The Kirinyaga County Health System, Kenya - GAKUU EsbonDocument17 pagesPerformance Analysis of The Kirinyaga County Health System, Kenya - GAKUU Esbonesbon gakuuNo ratings yet
- Kenya Pharmaceutical Pricing Study Policy Analysis and Recommendations - GAKUU EsbonDocument17 pagesKenya Pharmaceutical Pricing Study Policy Analysis and Recommendations - GAKUU Esbonesbon gakuuNo ratings yet
- Devolution in Health-Kenya-Esbon - GakuuDocument21 pagesDevolution in Health-Kenya-Esbon - Gakuuesbon gakuuNo ratings yet
- The State of Pharmacoeconomic Evaluation Studies in Kenya and An Analysis of Their Influence On Medicine Selection and Utilisation: A ReviewDocument20 pagesThe State of Pharmacoeconomic Evaluation Studies in Kenya and An Analysis of Their Influence On Medicine Selection and Utilisation: A Reviewesbon gakuuNo ratings yet
- Engaging Private Health Providers For TB Care and Prevention in Kirinyaga, Kenya - EsbonDocument12 pagesEngaging Private Health Providers For TB Care and Prevention in Kirinyaga, Kenya - Esbonesbon gakuuNo ratings yet
- Celiac Disease: DR Ajeet Kumar Lohana Senior Registrar Gastroenterology AtmcDocument59 pagesCeliac Disease: DR Ajeet Kumar Lohana Senior Registrar Gastroenterology AtmcAjeet LohanaNo ratings yet
- Vis AnneDocument22 pagesVis AnneImelda AtikaNo ratings yet
- Identification of Exudates in InflammationDocument5 pagesIdentification of Exudates in InflammationAnna AzukiNo ratings yet
- Revised Mrcs Syl Lab UsDocument68 pagesRevised Mrcs Syl Lab Usshafa_atNo ratings yet
- Medical Imaging WebquestDocument8 pagesMedical Imaging Webquestapi-262193618No ratings yet
- KENDRIYA VIDYALAYA Biology Investigatory ProjectDocument28 pagesKENDRIYA VIDYALAYA Biology Investigatory Projectvishali GNo ratings yet
- Journal Reading About DengueDocument23 pagesJournal Reading About DengueJoji BaitNo ratings yet
- Test Bank For Ethics and Law in Dental Hygiene 3rd Edition by Beemsterboer DownloadDocument20 pagesTest Bank For Ethics and Law in Dental Hygiene 3rd Edition by Beemsterboer Downloadkennethlewiscsnxqkjoza100% (27)
- Indian Chilhood CirrhosisDocument28 pagesIndian Chilhood CirrhosisBelbi MolNo ratings yet
- Multiple PregnancyDocument20 pagesMultiple PregnancyNurul Fahmiza TumiranNo ratings yet
- Integrated Therapeutics IiiDocument16 pagesIntegrated Therapeutics IiiSalahadinNo ratings yet
- Clinico Histological Evaluation of Dentino-Pulpal Complex of DirectDocument6 pagesClinico Histological Evaluation of Dentino-Pulpal Complex of DirectAle ZuzaNo ratings yet
- WHO TRS 961 EngDocument440 pagesWHO TRS 961 Engkorde1100% (3)
- President Ramon Magsaysay State University: Sagutin Mo Ko! PANUTO: Sagutin Ang Mga Sumusunod Na KatanunganDocument4 pagesPresident Ramon Magsaysay State University: Sagutin Mo Ko! PANUTO: Sagutin Ang Mga Sumusunod Na KatanunganAndrea AngelicaNo ratings yet
- Transoral Laser MicrosurgeryDocument4 pagesTransoral Laser MicrosurgeryanniebuhrNo ratings yet
- Test Blueprinting II: Creating A Test BlueprintDocument10 pagesTest Blueprinting II: Creating A Test BlueprintDr. Doaa El MorsiNo ratings yet
- MED 251 Block 9 PHL Brochure and TarpDocument6 pagesMED 251 Block 9 PHL Brochure and TarpFerdinand Sta Ana Jr.No ratings yet
- Required Coursework For Dental SchoolDocument5 pagesRequired Coursework For Dental Schoolrqaeibifg100% (2)
- NSTP Act2 Suan, Allyna ChantalDocument8 pagesNSTP Act2 Suan, Allyna ChantalChan TalNo ratings yet
- Nova Stat Strip Glucose 261021Document35 pagesNova Stat Strip Glucose 261021Herbanu Haryo PramonoNo ratings yet
- Laporan Kegiatan Dan Reimbursement Biaya Pengurusan Visa AustraliaDocument5 pagesLaporan Kegiatan Dan Reimbursement Biaya Pengurusan Visa AustraliamemekbecekNo ratings yet
- Health Management SynopsisDocument3 pagesHealth Management SynopsisSubrat PatnaikNo ratings yet
- PSM (Must Know)Document19 pagesPSM (Must Know)PranavNo ratings yet
- ENGLISH For NURSESDocument28 pagesENGLISH For NURSESnyoman pastikaNo ratings yet
- Scientific Method ReadingDocument4 pagesScientific Method Readingrai dotcomNo ratings yet
- Quarantine and Isolation Guidance - 1.14.22Document6 pagesQuarantine and Isolation Guidance - 1.14.22Umair Ahmed AbbasiNo ratings yet
- Reseaech Group 4 1 AutoRecovered 2 1Document70 pagesReseaech Group 4 1 AutoRecovered 2 1Abegail Joy AragonNo ratings yet
- SickLeaveCertificate With and Without Diagnosis 20240227 144109Document2 pagesSickLeaveCertificate With and Without Diagnosis 20240227 144109Sawad SawaNo ratings yet
- Rheumatic Heart Disease: Presented by Dr. Thein Tun 2 DR.D.SC (Oral Medicine)Document22 pagesRheumatic Heart Disease: Presented by Dr. Thein Tun 2 DR.D.SC (Oral Medicine)dr.thein tunNo ratings yet
- Pakistan FloodsDocument13 pagesPakistan FloodsfashionIDM77No ratings yet