You might also like
- PENGGUNAAN OBAT PADA SISTEM CARDIOVASCULARDocument56 pagesPENGGUNAAN OBAT PADA SISTEM CARDIOVASCULARwidya vannesaNo ratings yet
- Oh My Gout!: Jasmine Grace G. Africano, M.D. 1 Year IM-SIGHDocument32 pagesOh My Gout!: Jasmine Grace G. Africano, M.D. 1 Year IM-SIGHJasmine AfricanoNo ratings yet
- Medically ComprmisedDocument73 pagesMedically Comprmisedhaitham192002No ratings yet
- Chapter 3: Perioperative ManagementDocument14 pagesChapter 3: Perioperative ManagementpoddataNo ratings yet
- Management of Severe Hypertension, Hypertension in Special ConditionDocument43 pagesManagement of Severe Hypertension, Hypertension in Special Conditionabhandlung100% (3)
- 6.Z8sNyP 6 GHafez HT and Antihypertensive DrugsDocument81 pages6.Z8sNyP 6 GHafez HT and Antihypertensive Drugsyasmin.rahmany03No ratings yet
- Vasodilator and Anticoagulant Agents SummaryDocument23 pagesVasodilator and Anticoagulant Agents Summarymonyet65No ratings yet
- Drugs Used in Cardiovascular SystemDocument57 pagesDrugs Used in Cardiovascular SystemSandeep ChaudharyNo ratings yet
- 1614978209sampleDocument9 pages1614978209sampleReddyNo ratings yet
- 5 Pre Op CS & Major Surgery 22.06.2015Document5 pages5 Pre Op CS & Major Surgery 22.06.2015Mahesh RathnayakeNo ratings yet
- Cardiac AnesthesiologyDocument48 pagesCardiac AnesthesiologyNiaNo ratings yet
- Drugs Used in DentistryDocument48 pagesDrugs Used in DentistrySeptimiu TiplicaNo ratings yet
- An Update Management of Acute Ischemic Stroke: SurotoDocument36 pagesAn Update Management of Acute Ischemic Stroke: SurotoShinta DianNo ratings yet
- Oral Anti-HTN Medications: ACE Inhibitors, ARBs, CCBs, Diuretics, Beta BlockersDocument84 pagesOral Anti-HTN Medications: ACE Inhibitors, ARBs, CCBs, Diuretics, Beta Blockersأبوأحمد الحكيمNo ratings yet
- Anesthesia Revision E6.5 (Medicalstudyzone - Com)Document34 pagesAnesthesia Revision E6.5 (Medicalstudyzone - Com)Rohan RathoreNo ratings yet
- Palliative care-MBODocument17 pagesPalliative care-MBOChonnikan LimpongsanurukNo ratings yet
- Atrial Fibrillation TDDocument6 pagesAtrial Fibrillation TDapi-594366475No ratings yet
- Pharmacology For Nclex PowerPointDocument209 pagesPharmacology For Nclex PowerPointEver Rose DangaseNo ratings yet
- Neutropenic Sepsis-Tls-Anaphylaxis-ExtravasationDocument40 pagesNeutropenic Sepsis-Tls-Anaphylaxis-ExtravasationSA NodeNo ratings yet
- Farmakoterapi StrokeDocument33 pagesFarmakoterapi StrokeMuhammad Aldi SetiawanNo ratings yet
- Presentasi Hipertensi BPJS 20518Document109 pagesPresentasi Hipertensi BPJS 20518Dody TamaraNo ratings yet
- ExodoniaDocument184 pagesExodoniaMohsin HabibNo ratings yet
- Farmakologi 1 Antihypertension: NURUL HASANAH (1800085)Document31 pagesFarmakologi 1 Antihypertension: NURUL HASANAH (1800085)MutiaraBintangNo ratings yet
- Anti Hypertensive DrugsDocument113 pagesAnti Hypertensive DrugsRobert DowneyNo ratings yet
- Anaesthesia Revision E6.5Document33 pagesAnaesthesia Revision E6.5Riya SharmaNo ratings yet
- PharmacologyDocument4 pagesPharmacologyEmmanuel CuevasNo ratings yet
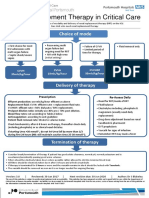
- Renal Replacement Therapy in Critical Care: Choice of ModeDocument15 pagesRenal Replacement Therapy in Critical Care: Choice of ModePeter AgabaNo ratings yet
- Neonatal HypertensionDocument21 pagesNeonatal HypertensionMuhammad Ammar Abdul WahabNo ratings yet
- Tatalaksana Krisis HipertensiDocument38 pagesTatalaksana Krisis HipertensiDr Edi HidayatNo ratings yet
- ACLS DrugsDocument16 pagesACLS Drugstostc100% (2)
- Case Presentation On Perforated Gastric Ulcer With Alcoholic Cirrhosis and Tongue CancerDocument19 pagesCase Presentation On Perforated Gastric Ulcer With Alcoholic Cirrhosis and Tongue CancerUmme habeebaNo ratings yet
- HypertensionDocument15 pagesHypertensionSusan GamalNo ratings yet
- Hypertension: Classification, Treatment and Special PopulationsDocument21 pagesHypertension: Classification, Treatment and Special PopulationsRawabi SalehNo ratings yet
- Drugs Study Neh Jai2xDocument10 pagesDrugs Study Neh Jai2xjai2xNo ratings yet
- Clinical Features and Management of Common PoisonsDocument33 pagesClinical Features and Management of Common PoisonsTrishenth FonsekaNo ratings yet
- Anaesthesia For A Patient With Coagulation DisorderDocument33 pagesAnaesthesia For A Patient With Coagulation DisorderNdenwaneku OkuwaNo ratings yet
- Anti ArrhythmicsDocument46 pagesAnti Arrhythmicsmunim1192No ratings yet
- Drug StudyDocument10 pagesDrug Studytamtam_antonioNo ratings yet
- PCRDocument7 pagesPCRJorge RodriguesNo ratings yet
- Prosthodontic Management of Geriatric PatientDocument101 pagesProsthodontic Management of Geriatric PatientMrunal Doiphode100% (2)
- Lisinopril, TAB: Generic Name of Medication: Brand/trade Name of MedicationDocument6 pagesLisinopril, TAB: Generic Name of Medication: Brand/trade Name of MedicationCliff by the seaNo ratings yet
- Common Drugs in Obsgyn 2Document42 pagesCommon Drugs in Obsgyn 2Meekel SusikuNo ratings yet
- CASE PRESENTATION ON STROKE by SriramDocument18 pagesCASE PRESENTATION ON STROKE by SriramSriram SuryaNo ratings yet
- Cardiovascular Diseases 2Document40 pagesCardiovascular Diseases 2Ali MuradNo ratings yet
- Management Strategy in Hypertensive Crisis The Role of NicardipineDocument38 pagesManagement Strategy in Hypertensive Crisis The Role of Nicardipinezulfikar adiNo ratings yet
- Drugs Used in CcuDocument169 pagesDrugs Used in CcuAnusha Verghese100% (3)
- Mi FinalDocument29 pagesMi Finalmuthu gowthamNo ratings yet
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument112 pagesOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreabctutorNo ratings yet
- En Ox A Par inDocument3 pagesEn Ox A Par inapi-3797941No ratings yet
- Laporan Learning Objective Skenario 2 Blok Emergency: Sabrina Fazriesa 1418011194Document22 pagesLaporan Learning Objective Skenario 2 Blok Emergency: Sabrina Fazriesa 1418011194Sabrina FazriesaNo ratings yet
- ACLS ModuleDocument68 pagesACLS ModuleSalah ElbadawyNo ratings yet
- Pharm Defn IPE CasesDocument6 pagesPharm Defn IPE CasesbenjamingNo ratings yet
- Renal, Urinary and GI Complications After SurgeryDocument38 pagesRenal, Urinary and GI Complications After SurgeryAbdurre YNo ratings yet
- DILIDocument40 pagesDILIYunik YuliapsariNo ratings yet
- Critical Care Drugs OverviewDocument23 pagesCritical Care Drugs OverviewAsri Ernadi100% (1)
- Updates On Acute Coronary SyndromeDocument121 pagesUpdates On Acute Coronary SyndromeDwi Akbarina YahyaNo ratings yet
- Case Icu 1Document40 pagesCase Icu 1Salwa KaramanNo ratings yet
- Cardiotoxicology ToxicologyDocument41 pagesCardiotoxicology ToxicologyIncha MaayaloNo ratings yet
- Ste Conchem q4m5 Ffhnas Annex PDFDocument31 pagesSte Conchem q4m5 Ffhnas Annex PDFJesus GombaNo ratings yet
- Covid-19 Info DriveDocument61 pagesCovid-19 Info DriveMac MacapilNo ratings yet
- Summative P.E 11Document1 pageSummative P.E 11SHAINA MARIE ESGUERRANo ratings yet
- Burkitt's LyphomaDocument21 pagesBurkitt's Lyphomamacdominic22No ratings yet
- Case Analysis - Pregnant With AsthmaDocument1 pageCase Analysis - Pregnant With AsthmaJanine mae MacaraigNo ratings yet
- Pediatric Nutrition Assessment FormDocument2 pagesPediatric Nutrition Assessment FormSHAILAJA SORTENo ratings yet
- Epidemiology of Mental Health Disorders Particularly PTSD Among Internally Displaced People (IDPs) in Port-Sudan Post-Conflict Setting: A Community-Based Cross-Sectional StudyDocument7 pagesEpidemiology of Mental Health Disorders Particularly PTSD Among Internally Displaced People (IDPs) in Port-Sudan Post-Conflict Setting: A Community-Based Cross-Sectional StudyInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- FirelightDocument112 pagesFirelightgurlcinnamon125No ratings yet
- ICU Diploma MCQDocument14 pagesICU Diploma MCQMin Thu Lwin100% (2)
- Autoimmune Lymphoproliferative Syndrome. Update and ReviewDocument18 pagesAutoimmune Lymphoproliferative Syndrome. Update and Reviewstefany acNo ratings yet
- POCUS Guide for Evaluating Intravenous Cava (IVC) and Shock TypesDocument55 pagesPOCUS Guide for Evaluating Intravenous Cava (IVC) and Shock TypesKorkrit MeekaewNo ratings yet
- Mental Status Assessment FormDocument3 pagesMental Status Assessment FormJohn Paolo OrioNo ratings yet
- TyphusDocument21 pagesTyphusJ J MEDIANo ratings yet
- GIT ChecklistDocument3 pagesGIT Checklisthak jsoNo ratings yet
- Cidesco Case Histories BookletDocument11 pagesCidesco Case Histories Bookletmatina papaspyrouNo ratings yet
- Detecting and Treating Lung Congestion With Kidney.20Document9 pagesDetecting and Treating Lung Congestion With Kidney.20uriel1No ratings yet
- Case Report 1676563639Document6 pagesCase Report 1676563639noah jemedafeNo ratings yet
- (ENT-OPT-FRS) End-Posting Examination Questions (G3) - 20180208 - 160700Document23 pages(ENT-OPT-FRS) End-Posting Examination Questions (G3) - 20180208 - 160700Steph Stephanie100% (1)
- Addendum of Charged PersonsDocument6 pagesAddendum of Charged PersonsCynthiaMcLeodSun0% (1)
- ThyrotoxicosisDocument16 pagesThyrotoxicosisFiorella Peña MoraNo ratings yet
- Lithium ToxicityDocument28 pagesLithium ToxicityReejan PaudelNo ratings yet
- 2-PLAB Answer Big Mock April 2021-PrintDocument12 pages2-PLAB Answer Big Mock April 2021-Printali etikar100% (1)
- VVVV PDFDocument13 pagesVVVV PDFNimas Ayu NNo ratings yet
- Bells Palsy Nelsons TextBook of Pediatrics 20th EditionDocument3 pagesBells Palsy Nelsons TextBook of Pediatrics 20th EditionKRIZIA CORRINE CAINGCOY SAN PEDRONo ratings yet
- Initial Management of The Critically Ill Adult With An Unknown Overdose - UpToDateDocument17 pagesInitial Management of The Critically Ill Adult With An Unknown Overdose - UpToDateDANIELA BOHÓRQUEZ ORTEGANo ratings yet
- Girl Interrupted Borderline Antisocial Personality Case Study PDFDocument6 pagesGirl Interrupted Borderline Antisocial Personality Case Study PDFcalliemozartNo ratings yet
- Anxiety Disorders Selective Mutism and Specific PhobiaDocument8 pagesAnxiety Disorders Selective Mutism and Specific PhobiaIQRA YOUSAFNo ratings yet
- Awareness of Antibiotic Usage and Antibiotic Resistance - A Case Study in Selangor, MalaysiaDocument9 pagesAwareness of Antibiotic Usage and Antibiotic Resistance - A Case Study in Selangor, MalaysiaNoor NordinNo ratings yet
- Isosorbide DinitrateDocument1 pageIsosorbide Dinitrate202110439No ratings yet
- Color Doppler Flow Imaging of Retrobulbar Ocular Blood Flow Changes in Retinal Artery Occlusions Caused by Cosmetic Facial Filler InjectionsDocument5 pagesColor Doppler Flow Imaging of Retrobulbar Ocular Blood Flow Changes in Retinal Artery Occlusions Caused by Cosmetic Facial Filler InjectionsKerlida SantosNo ratings yet