You might also like
- SMETA 6.1 Measurement Criteria PDFDocument96 pagesSMETA 6.1 Measurement Criteria PDFTuấn Mai vănNo ratings yet
- 00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenDocument13 pages00130478-202105000-00006 Serial Neurologic Assessment in Pediatrics (SNAP) : A New Tool For Bedside Neurologic Assessment of Critically Ill ChildrenYo MeNo ratings yet
- Chuyên Đề Rèn Luyện Từ Vựng Tiếng Anh 1 Từ Dùng Cho 3 Câu (3 Nghĩa Khác Nhau) - Vĩnh Bá PDFDocument436 pagesChuyên Đề Rèn Luyện Từ Vựng Tiếng Anh 1 Từ Dùng Cho 3 Câu (3 Nghĩa Khác Nhau) - Vĩnh Bá PDFPhạm Đặng Khánh Hà100% (2)
- Nursing Standard PrinciplesDocument2 pagesNursing Standard PrinciplesRoscelie KhoNo ratings yet
- Clinical Tools Used in Young Infants Born Very Preterm To Predict Motor and Cognitive Delay (Not Cerebral Palsy) : A Systematic ReviewDocument9 pagesClinical Tools Used in Young Infants Born Very Preterm To Predict Motor and Cognitive Delay (Not Cerebral Palsy) : A Systematic ReviewAna paula CamargoNo ratings yet
- Sharma2011 Article GrowthAndNeurosensoryOutcomesODocument6 pagesSharma2011 Article GrowthAndNeurosensoryOutcomesOSayak ChowdhuryNo ratings yet
- Evidencias VojtaDocument9 pagesEvidencias VojtaRommel AndresNo ratings yet
- life-14-00480Document13 pageslife-14-00480Shahmeer HassanNo ratings yet
- Early Brain Enlargement and Excess Fluid Linked to Later Autism DiagnosisDocument11 pagesEarly Brain Enlargement and Excess Fluid Linked to Later Autism DiagnosisSheila Rodriguez LopezNo ratings yet
- Bosanquet Etal DMCN 2013Document9 pagesBosanquet Etal DMCN 2013ramopavelNo ratings yet
- Noetzel and R.D. Sheth M. Shevell, S. Ashwal, D. Donley, J. Flint, M. Gingold, D. Hirtz, A. Majnemer, MDocument16 pagesNoetzel and R.D. Sheth M. Shevell, S. Ashwal, D. Donley, J. Flint, M. Gingold, D. Hirtz, A. Majnemer, MjoeunisaNo ratings yet
- Developmental Interventions in the NICU May Boost Cognitive DevelopmentDocument8 pagesDevelopmental Interventions in the NICU May Boost Cognitive DevelopmentMirza RisqaNo ratings yet
- JurdingDocument6 pagesJurdingsiti hazard aldinaNo ratings yet
- SaudiJKidneyDisTranspl304812-2026889 053748Document7 pagesSaudiJKidneyDisTranspl304812-2026889 053748yenny handayani sihiteNo ratings yet
- gmTIMP CorrelationDocument7 pagesgmTIMP CorrelationArtur SalesNo ratings yet
- Evaluation of The Child With Global Developmental DelayDocument14 pagesEvaluation of The Child With Global Developmental DelaylauramwoodyardNo ratings yet
- She Vell 2003Document15 pagesShe Vell 2003Ivan VeriswanNo ratings yet
- Kinamatic Analisis Por Video Mov 2016Document7 pagesKinamatic Analisis Por Video Mov 2016LucyFloresNo ratings yet
- Paediatrica Indonesiana: Nicholas Calvin, Yetty RamliDocument6 pagesPaediatrica Indonesiana: Nicholas Calvin, Yetty RamliriloaddNo ratings yet
- 10 1016@j Yapd 2019 04 002Document20 pages10 1016@j Yapd 2019 04 002KopitesNo ratings yet
- PTH 725 Research Case ReportDocument10 pagesPTH 725 Research Case Reportapi-528037163No ratings yet
- Mukhopadhyay2010 Article NeurodevelopmentalAndBehavioraDocument5 pagesMukhopadhyay2010 Article NeurodevelopmentalAndBehavioraSayak ChowdhuryNo ratings yet
- HineDocument7 pagesHineAkhila Chowdary100% (1)
- tmp9CF9 TMPDocument9 pagestmp9CF9 TMPFrontiersNo ratings yet
- Children: Devices For Ambulatory Monitoring of Sleep-Associated Disorders in Children With Neurological DiseasesDocument15 pagesChildren: Devices For Ambulatory Monitoring of Sleep-Associated Disorders in Children With Neurological DiseasesSyairah Banu DjufriNo ratings yet
- Early Neurologic Assessment in Preterm-Infants: Integration of Traditional Neurologic Examination and Observation of General MovementsDocument7 pagesEarly Neurologic Assessment in Preterm-Infants: Integration of Traditional Neurologic Examination and Observation of General MovementsAnonymous QOCn5dNo ratings yet
- Relationship Between Communication Skills and Gross Motor Function in Preschool Children With Cerebral PalsyDocument8 pagesRelationship Between Communication Skills and Gross Motor Function in Preschool Children With Cerebral PalsyKiki PuchiNo ratings yet
- Neonatal MRI To Predict Neurodevelopmental Outcomes in Preterm InfantsDocument10 pagesNeonatal MRI To Predict Neurodevelopmental Outcomes in Preterm InfantsJuan Camilo LandazuriNo ratings yet
- Research Article: Sleep Disturbance in ADHD Children: Prevalence, Clinical Profile and InfluencingDocument10 pagesResearch Article: Sleep Disturbance in ADHD Children: Prevalence, Clinical Profile and InfluencingHoney M. LopezNo ratings yet
- Priyanka K P Synopsis-1Document18 pagesPriyanka K P Synopsis-1RAJESHWARI PNo ratings yet
- 52-Article Text-113-1-10-20160201Document6 pages52-Article Text-113-1-10-20160201Gita TikihaiNo ratings yet
- Cerebral Palsy PDFDocument12 pagesCerebral Palsy PDFapi-319493532No ratings yet
- Down SyndromeDocument12 pagesDown SyndromeaidaeimanNo ratings yet
- Cognitive Outcome (2014)Document8 pagesCognitive Outcome (2014)Lore VasquezNo ratings yet
- Dhawan 2016Document6 pagesDhawan 2016lilisNo ratings yet
- Effectiveness of Sensory Integration Program in Motor Skills in Children With AutismDocument6 pagesEffectiveness of Sensory Integration Program in Motor Skills in Children With AutismLiliann RiveraNo ratings yet
- Abstract Booklet 2010Document50 pagesAbstract Booklet 2010Danijela VukicevicNo ratings yet
- Outcome in Childhood Guillain-Barré SyndromeDocument5 pagesOutcome in Childhood Guillain-Barré SyndromechristianFPTNo ratings yet
- Prognostic Factors for Relapse and Outcome in Pediatric Acute Transverse MyelitisDocument11 pagesPrognostic Factors for Relapse and Outcome in Pediatric Acute Transverse Myelitisyusak sampeNo ratings yet
- Care Pathways Early Diagnosis PrintDocument5 pagesCare Pathways Early Diagnosis PrintiannikkiNo ratings yet
- Mukhopadhyay 2010Document4 pagesMukhopadhyay 2010Sayak ChowdhuryNo ratings yet
- Neuropsychology Reports For Childhood Brain Tumor Survivors: Implementation of Recommendations at Home and SchoolDocument8 pagesNeuropsychology Reports For Childhood Brain Tumor Survivors: Implementation of Recommendations at Home and SchoolKamila PorębskaNo ratings yet
- Long-Term Clinical Course of Glut1 Deficiency SyndromeDocument10 pagesLong-Term Clinical Course of Glut1 Deficiency SyndromeilonaskorinNo ratings yet
- Beckung Et Al-2007-Developmental Medicine Child NeurologyDocument6 pagesBeckung Et Al-2007-Developmental Medicine Child Neurologyapi-310963007No ratings yet
- Neuroimagenes en Preterminos y Rendimiento EscolarDocument15 pagesNeuroimagenes en Preterminos y Rendimiento EscolarAlejandroVeraVargasNo ratings yet
- Evaluation of The Child With Global Developmental DelayDocument14 pagesEvaluation of The Child With Global Developmental DelayplaincircleNo ratings yet
- Care Pathways Early Diagnosis Plain LanguageDocument1 pageCare Pathways Early Diagnosis Plain LanguageAbd El-RahmanNo ratings yet
- 1 s2.0 S0022347605815872 MainDocument8 pages1 s2.0 S0022347605815872 MainDaniel SargentNo ratings yet
- 00!!!!!! FINAL THESIS SUMMARYDocument7 pages00!!!!!! FINAL THESIS SUMMARYroshen02No ratings yet
- Early intervention improves cognitive outcomes for preterm infantsDocument9 pagesEarly intervention improves cognitive outcomes for preterm infantsJuan Carlos Jiménez FosadoNo ratings yet
- Assessment of General Movements For Neurological Development of High-Risk Preterm Infants by Seme-CigleneekiDocument7 pagesAssessment of General Movements For Neurological Development of High-Risk Preterm Infants by Seme-CigleneekiFe TusNo ratings yet
- Gagliardi 2008Document6 pagesGagliardi 2008Carolina BorchesNo ratings yet
- 637Document4 pages637Sharuk AhamedNo ratings yet
- INCLEN Diagnostic Tool For Epilepsy (INDT-EPI) For Primary Care Physicians: Development and ValidationDocument5 pagesINCLEN Diagnostic Tool For Epilepsy (INDT-EPI) For Primary Care Physicians: Development and ValidationAulya ArchuletaNo ratings yet
- Pediatric CKD Review Examines Cognition, Neuroimaging and BiomarkersDocument9 pagesPediatric CKD Review Examines Cognition, Neuroimaging and BiomarkersKarina BorgesNo ratings yet
- KoshiDocument8 pagesKoshiCristian Odany Lopez GregorioNo ratings yet
- Gross Motor and SubsequencesDocument10 pagesGross Motor and SubsequencesHOA TRƯƠNGNo ratings yet
- West Syndrome Outcomes Linked to Early TreatmentDocument5 pagesWest Syndrome Outcomes Linked to Early TreatmentHari ThiyagarajanNo ratings yet
- Down 3 - 5 MesesDocument8 pagesDown 3 - 5 MesesJeancarlosTerapiaFisicaNo ratings yet
- Nygren 2012Document11 pagesNygren 2012Jose Alonso Aguilar ValeraNo ratings yet
- Deformidad Craneal y Desarrollo MotorDocument9 pagesDeformidad Craneal y Desarrollo MotordianareinaNo ratings yet
- Mangione Et Al-2011-Ultrasound in Obstetrics & GynecologyDocument6 pagesMangione Et Al-2011-Ultrasound in Obstetrics & GynecologyAnggita Rizki KusumaNo ratings yet
- Neonatal Seizures: Current Management and Future ChallengesFrom EverandNeonatal Seizures: Current Management and Future ChallengesLakshmi NagarajanRating: 4 out of 5 stars4/5 (2)
- Motor BehaviorDocument17 pagesMotor BehaviorMarceNo ratings yet
- 1 s2.0 S1836955321000965 MainDocument9 pages1 s2.0 S1836955321000965 MainMetin HakkanNo ratings yet
- 2021 Padrões de Sono em Bebês e Suas MãesDocument8 pages2021 Padrões de Sono em Bebês e Suas MãesCibelle FormigaNo ratings yet
- 2022 Fatores Associados A Competencia Motora em Pre-Escolares BrasilDocument16 pages2022 Fatores Associados A Competencia Motora em Pre-Escolares BrasilCibelle FormigaNo ratings yet
- Pediatricsleepdurationconsensus PDFDocument2 pagesPediatricsleepdurationconsensus PDFAnonymous iU1h1iRDNo ratings yet
- 2022 Barreiras e Facilitadores para o Método CanguruDocument11 pages2022 Barreiras e Facilitadores para o Método CanguruCibelle FormigaNo ratings yet
- Post Tonsillectomy Bleeding Clinical Practice GuidelineDocument5 pagesPost Tonsillectomy Bleeding Clinical Practice Guidelinemohamed fahmyNo ratings yet
- Safe carriage of dangerous goods by airDocument2 pagesSafe carriage of dangerous goods by airNuran Dursunoğlu100% (1)
- Rcads-Child TemplateDocument3 pagesRcads-Child TemplateHome Sweet100% (1)
- Worksheet For Respiration Low AnswersDocument2 pagesWorksheet For Respiration Low AnswersIcs 2022No ratings yet
- Middy CCTV Case StudyDocument2 pagesMiddy CCTV Case StudyLucas StacheckiNo ratings yet
- Ashgate - Landscape Professional Practice PDFDocument281 pagesAshgate - Landscape Professional Practice PDFyondaimethunderNo ratings yet
- Resona r9 Platinum Multi Parametric Breast SolutionDocument2 pagesResona r9 Platinum Multi Parametric Breast SolutionXing LuNo ratings yet
- 5th Grade Reading Comprehension Worksheets - Fifth Grade Week 4Document2 pages5th Grade Reading Comprehension Worksheets - Fifth Grade Week 4Julius CesarNo ratings yet
- A. Gudang Farmasi 2023 (Feni Dwi) UpdateDocument882 pagesA. Gudang Farmasi 2023 (Feni Dwi) UpdatehefikurniasariNo ratings yet
- Igcse Biology Concepts Revision Chapter 1 To 8Document9 pagesIgcse Biology Concepts Revision Chapter 1 To 8naduniNo ratings yet
- Respiratory and Circulatory Systems Activity SheetDocument7 pagesRespiratory and Circulatory Systems Activity SheetalexNo ratings yet
- ArbomapDocument1 pageArbomapNEWS CENTER MaineNo ratings yet
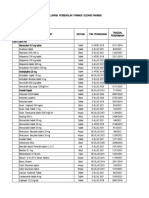
- AFMC MBBS Admissions Screening Dates for NEET UG 2021Document33 pagesAFMC MBBS Admissions Screening Dates for NEET UG 2021robert hookeNo ratings yet
- Covid MemoDocument4 pagesCovid Memocharlie malalangNo ratings yet
- 10 Medicinal Plants Approved by The Department of HealthDocument4 pages10 Medicinal Plants Approved by The Department of HealthASHLEY NICOLE JACINTONo ratings yet
- Benefits of Intermittent FastingDocument3 pagesBenefits of Intermittent FastingSaurabh PandeyNo ratings yet
- Unitati Certificare A5Document2 pagesUnitati Certificare A5enaionNo ratings yet
- Csec Physics Sbaform ModerationDocument1 pageCsec Physics Sbaform Moderationapi-248240402No ratings yet
- Implementing of Rewards and Punishments Toward Students' Motivation in ELDocument13 pagesImplementing of Rewards and Punishments Toward Students' Motivation in ELAriska ChikaNo ratings yet
- 6 135Document6 pages6 135Ashok LenkaNo ratings yet
- Skala Perilaku Seks PranikahDocument6 pagesSkala Perilaku Seks PranikahRiska amaliaNo ratings yet
- Occupational Safety and Health Act 2006Document86 pagesOccupational Safety and Health Act 2006Ivan BuhiinzaNo ratings yet
- OJT PORTFOLIO REDCROSS4A - RoveliDocument52 pagesOJT PORTFOLIO REDCROSS4A - RoveliRaffy Liwan Kalinga ChapterNo ratings yet
- 02network3 XPrac Mod4BDocument3 pages02network3 XPrac Mod4BAle SeviNo ratings yet
- Clearance PDFDocument1 pageClearance PDFJane DeckerNo ratings yet
- Inb 372Document3 pagesInb 372SunnyNo ratings yet
- Project Report On Health & Safety PDFDocument3 pagesProject Report On Health & Safety PDFAakash SolankiNo ratings yet