You might also like
- Brukner and Khans Clinical Sports Medicine Injuries, Volume 1 - MedicineDocument7 pagesBrukner and Khans Clinical Sports Medicine Injuries, Volume 1 - Medicinezaferyha17% (6)
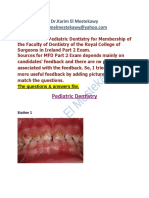
- MFD Part 2 - Pediatric Dentistry Exams Questions & AnswersDocument17 pagesMFD Part 2 - Pediatric Dentistry Exams Questions & AnswersDental Knowledge School100% (1)
- 05 Clinical Failures and Its Management in Fixed Partial DentureDocument45 pages05 Clinical Failures and Its Management in Fixed Partial Denturesonal_karania66% (29)
- Space Maintainer - A ReviewDocument5 pagesSpace Maintainer - A ReviewHabeeb AL-AbsiNo ratings yet
- Recent Criterias of Tooth Preparation inDocument6 pagesRecent Criterias of Tooth Preparation inFelyciaNo ratings yet
- Serial ExtractionDocument38 pagesSerial ExtractionRamy HanyNo ratings yet
- YANG SHENG 2011 October B PDFDocument70 pagesYANG SHENG 2011 October B PDFSasa PuiuNo ratings yet
- Jurnal Kebidanan KomunitasDocument5 pagesJurnal Kebidanan KomunitasdeffiNo ratings yet
- Bulacan State University College of Nursing: Bulsu-Op-Con-23F15 Revision: 0Document6 pagesBulacan State University College of Nursing: Bulsu-Op-Con-23F15 Revision: 0Richmon SantosNo ratings yet
- Altoukhi 2020Document13 pagesAltoukhi 2020Alvaro LaraNo ratings yet
- Inlays & Onlays Clinical Experiences and Literature Review: Journal of Dental Health, Oral Disorders & TherapyDocument7 pagesInlays & Onlays Clinical Experiences and Literature Review: Journal of Dental Health, Oral Disorders & TherapycindyannisamelatiNo ratings yet
- Pulp Therapy For The Young Permanent Dentition: ApexogenesisDocument15 pagesPulp Therapy For The Young Permanent Dentition: Apexogenesisapi-3855312No ratings yet
- Lect 14 Preventive Dentistry - Dental SealantDocument8 pagesLect 14 Preventive Dentistry - Dental Sealantزهراء فاضل اجبير فعيلNo ratings yet
- Lecture 7 Management of Deep Seated Carious LesionsDocument11 pagesLecture 7 Management of Deep Seated Carious LesionsDt omarNo ratings yet
- Pit and Fissure Sealants: Preventive DentistryDocument10 pagesPit and Fissure Sealants: Preventive Dentistryبان منذر قدوريNo ratings yet
- New Approach in Restorative DentistryDocument6 pagesNew Approach in Restorative Dentistryبان منذر قدوريNo ratings yet
- Pediatric Dentistry: Restorative Dentistry For ChildrenDocument28 pagesPediatric Dentistry: Restorative Dentistry For ChildrenDr-Kinan Khalil ShraifyNo ratings yet
- Post Insertion Problems and Their Management in Co PDFDocument6 pagesPost Insertion Problems and Their Management in Co PDFHussein MakhloufNo ratings yet
- Restorative Dentistry in The Primary Dentition - Decisions in DentistryDocument11 pagesRestorative Dentistry in The Primary Dentition - Decisions in DentistryRayhan DaneoNo ratings yet
- Caries Managements: Is Restoration Required??Document24 pagesCaries Managements: Is Restoration Required??Jitender ReddyNo ratings yet
- NQVH The Hall Technique ManualDocument19 pagesNQVH The Hall Technique Manualpriti adsulNo ratings yet
- Which Restorative Materials Would You Recommend For Use in Primary TeethDocument9 pagesWhich Restorative Materials Would You Recommend For Use in Primary TeethentistdeNo ratings yet
- Management Flabby RidgeDocument4 pagesManagement Flabby RidgeNidya Patricia Sembiring100% (1)
- Surgical Treatment of Impacted CaninesDocument10 pagesSurgical Treatment of Impacted CaninesDavid ArévaloNo ratings yet
- Gigi Tiruan GasketDocument5 pagesGigi Tiruan GasketGus BasyaNo ratings yet
- CariologyDocument6 pagesCariologyNadia Khalil100% (1)
- OprativeDocument62 pagesOprativesamar yousif mohamedNo ratings yet
- Pulpotomy: IndicationsDocument5 pagesPulpotomy: IndicationsAseelNo ratings yet
- Patient Selection in Lingual OrthodonticsDocument8 pagesPatient Selection in Lingual OrthodonticsSreenivasa Krishna ChaitanyaNo ratings yet
- Patient Care Letter & Consent Form DateDocument10 pagesPatient Care Letter & Consent Form DaterchmurovicNo ratings yet
- PCC 1Document4 pagesPCC 1Dinar Sukma PamungkasNo ratings yet
- Hall TechniqueDocument19 pagesHall TechniqueanatomimanusiaNo ratings yet
- Conservative Treatment and PeriodontiumDocument4 pagesConservative Treatment and PeriodontiumReham RashwanNo ratings yet
- Over DentureDocument19 pagesOver DentureMohammed HassanNo ratings yet
- The Ultimate Dental Implants Guide From Gipsy Lane Dental CareDocument6 pagesThe Ultimate Dental Implants Guide From Gipsy Lane Dental CareAbdou SnaponsmileNo ratings yet
- DentureDocument80 pagesDentureDrShweta SainiNo ratings yet
- Extractions in OrthodonticsDocument6 pagesExtractions in OrthodonticsZubair AhmedNo ratings yet
- Gingival Mask 2013Document3 pagesGingival Mask 2013annysaNo ratings yet
- Prosthodontic Rehabilitation of A Patient With Maxillary Flabby Ridge - A Case ReportDocument4 pagesProsthodontic Rehabilitation of A Patient With Maxillary Flabby Ridge - A Case ReportdedeNo ratings yet
- Hall Technique, Stepwise Excavation, Partial Caries Removal TechniqueDocument4 pagesHall Technique, Stepwise Excavation, Partial Caries Removal TechniqueImbador LiesiesNo ratings yet
- Practical Dentistry For Veterinary NursesDocument10 pagesPractical Dentistry For Veterinary NursesLucy LulubinaNo ratings yet
- Crowding and Space Management in The Mixed DentitionDocument6 pagesCrowding and Space Management in The Mixed Dentitionaphist87No ratings yet
- 1457792866immediate DenturesDocument5 pages1457792866immediate DenturesegarochmawatiNo ratings yet
- Onlay InlayDocument7 pagesOnlay InlaySarino RagilNo ratings yet
- Management of Deep Carious Lesions 2Document6 pagesManagement of Deep Carious Lesions 2rujul_parikh_ind100% (1)
- Interceptive FinalDocument60 pagesInterceptive FinalRaj SinghNo ratings yet
- Pulpotomy ResearchDocument2 pagesPulpotomy ResearchdellorewoenamNo ratings yet
- Lecture 4 Pit and FissureDocument7 pagesLecture 4 Pit and FissureKhaled Al-haddadNo ratings yet
- Imediate 4Document3 pagesImediate 4Alifia Ayu DelimaNo ratings yet
- Adjuncts To Mouth Reconstruction S.: Alexander Forster, New York, N. YDocument5 pagesAdjuncts To Mouth Reconstruction S.: Alexander Forster, New York, N. YAmar BhochhibhoyaNo ratings yet
- 2 ExodontiaDocument53 pages2 ExodontiaWasiAliMemonNo ratings yet
- 10 - Fissure SealantDocument5 pages10 - Fissure SealantMohammed TarekNo ratings yet
- Lecture No8 Drnidhal 2017 Treatment PlaningDocument9 pagesLecture No8 Drnidhal 2017 Treatment PlaningQueen LiveNo ratings yet
- Guideline On Pediatric Restorative Dentistry: Originating Committee Review Council Adopted RevisedDocument7 pagesGuideline On Pediatric Restorative Dentistry: Originating Committee Review Council Adopted RevisedEduardo SánchezNo ratings yet
- Cu Sil DenturesDocument6 pagesCu Sil Denturessiddu76No ratings yet
- Treatment of Vital Pulp ExposureDocument10 pagesTreatment of Vital Pulp ExposureDana StanciuNo ratings yet
- Tugas Ikga Text BookDocument7 pagesTugas Ikga Text BookAprilTerbaeekNo ratings yet
- MFD Part 2 - Pediatric Dentistry Exams AnswersDocument19 pagesMFD Part 2 - Pediatric Dentistry Exams Answerszara khanNo ratings yet
- Articulo 2 EndoDocument11 pagesArticulo 2 EndoPedro Gonzalez DelgadoNo ratings yet
- Periodontal Assessment and Managment in Fixed ProsthodonticsDocument56 pagesPeriodontal Assessment and Managment in Fixed ProsthodonticsCristina Ene100% (2)
- Pin-Retained Restoration With Resin Bonded Composite of A Badly Broken ToothDocument3 pagesPin-Retained Restoration With Resin Bonded Composite of A Badly Broken ToothIOSRjournalNo ratings yet
- A To Z Orthodontics Vol 20 SurgicalDocument23 pagesA To Z Orthodontics Vol 20 Surgicalshruti premsagarNo ratings yet
- Immediate DenturesDocument35 pagesImmediate DenturesSimran SahniNo ratings yet
- Treatment Planning Single Maxillary Anterior Implants for DentistsFrom EverandTreatment Planning Single Maxillary Anterior Implants for DentistsNo ratings yet
- Post Op Complication and ManagementDocument5 pagesPost Op Complication and ManagementElectricken21No ratings yet
- Child Management OPS MIDTERMSDocument4 pagesChild Management OPS MIDTERMSElectricken21No ratings yet
- Anesthesiology For ChildrenDocument5 pagesAnesthesiology For ChildrenElectricken21No ratings yet
- Fixed Space MaintainersDocument3 pagesFixed Space MaintainersElectricken21No ratings yet
- Irr FinalDocument7 pagesIrr Finalapi-612103161No ratings yet
- Simulidae BlackflyDocument17 pagesSimulidae BlackflyVasimNo ratings yet
- Vendor ManualDocument19 pagesVendor Manualvinurules20No ratings yet
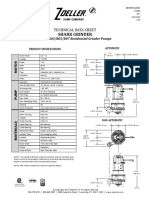
- Ficha Tecnica E803Document2 pagesFicha Tecnica E803Zenen AlarconNo ratings yet
- Outreach Service in Selected Local in Lagos NigeriaDocument48 pagesOutreach Service in Selected Local in Lagos NigeriaDOYINSOLA ADENUGANo ratings yet
- Complementary and Alternative Health Care Client Bill of RightsDocument2 pagesComplementary and Alternative Health Care Client Bill of Rightsapi-31121402No ratings yet
- NRP Newsletter 2015 FallwinterDocument14 pagesNRP Newsletter 2015 FallwinterJehangir AllamNo ratings yet
- Adult Friends Diaper (Thought Process)Document2 pagesAdult Friends Diaper (Thought Process)Rohan HiremathNo ratings yet
- ChapterDocument26 pagesChapterKlarence MendozaNo ratings yet
- Glomerulopathy: Acute Nephritic SyndromeDocument109 pagesGlomerulopathy: Acute Nephritic SyndromekamalNo ratings yet
- Consenso Chileno de Técnicas de Kinesiología Respiratoria en PediatríaDocument15 pagesConsenso Chileno de Técnicas de Kinesiología Respiratoria en PediatríaRobert CerdaNo ratings yet
- Metacarpal FractureDocument45 pagesMetacarpal FractureJinnasit TeeNo ratings yet
- OetDocument5 pagesOetGina Victor100% (2)
- Research IntroductionDocument18 pagesResearch IntroductionAngelica TebelinNo ratings yet
- (09032021) Press Release For Resumption of Selected Sports For NSG 2021 - MOEDocument2 pages(09032021) Press Release For Resumption of Selected Sports For NSG 2021 - MOEthesuperprogamer2 gamerNo ratings yet
- IPO Vijaya Diagnostic - 01092021 1630476491Document6 pagesIPO Vijaya Diagnostic - 01092021 1630476491Neil MannikarNo ratings yet
- Summary Report For:: 29-1131.00 - VeterinariansDocument6 pagesSummary Report For:: 29-1131.00 - Veterinariansapi-266289406No ratings yet
- WWW - England.nhs - Uk: Business Continuity Management NHS WorkshopDocument52 pagesWWW - England.nhs - Uk: Business Continuity Management NHS WorkshopForbetNo ratings yet
- Cryonics RereportDocument11 pagesCryonics RereporttysoncandyNo ratings yet
- Cox, D.R. - Donnelly, C.A. - Principles of Applied StatisticsDocument209 pagesCox, D.R. - Donnelly, C.A. - Principles of Applied Statisticstgabi2012No ratings yet
- Commrev - Insurance - Loti NotesDocument99 pagesCommrev - Insurance - Loti NotesCarlota Nicolas VillaromanNo ratings yet
- Effects of PollutionDocument1 pageEffects of PollutionSieben HerzenNo ratings yet
- Donut Hole LetterDocument2 pagesDonut Hole LetterPeter SullivanNo ratings yet
- Coxa PlanaDocument9 pagesCoxa PlanaRegine BlanzaNo ratings yet
- Advisory Additional Reminders Trainings and Seminars Barangay OfficialsDocument3 pagesAdvisory Additional Reminders Trainings and Seminars Barangay OfficialsJo ReyesNo ratings yet
- HR BipartitismDocument18 pagesHR BipartitismrobingehlotNo ratings yet