You might also like
- Cure Tooth Decay - Interview TranscriptDocument16 pagesCure Tooth Decay - Interview TranscripteisenreichNo ratings yet
- New Neighbors (January 2023)Document16 pagesNew Neighbors (January 2023)Watertown Daily TimesNo ratings yet
- Non-Vital Tooth Bleaching TechniquesDocument19 pagesNon-Vital Tooth Bleaching TechniquesPriyabrat Pattanaik100% (1)
- Composite Resin Properties and Restoration TechniqueDocument46 pagesComposite Resin Properties and Restoration Techniquetj_sweetgirl100% (1)
- Bonding in OrthodonticsDocument112 pagesBonding in OrthodonticslkjhgfdsalkNo ratings yet
- Pulp Protection AgentsDocument59 pagesPulp Protection Agentsتامي المغربيNo ratings yet
- Topical Fluorides for Caries PreventionDocument66 pagesTopical Fluorides for Caries PreventionSanthoshi ReddyNo ratings yet
- Direct Pulp Capping and Pulpotomy ProceduresDocument10 pagesDirect Pulp Capping and Pulpotomy ProceduresAhmed AbdNo ratings yet
- Isolation in Restorative DentistryDocument49 pagesIsolation in Restorative DentistrySusan100% (1)
- Conservative Esthetic Procedures: Part 2Document9 pagesConservative Esthetic Procedures: Part 2Dt omarNo ratings yet
- Pulp Therapy in ChildrenDocument4 pagesPulp Therapy in ChildrenshahinshamshiriNo ratings yet
- Obturation TechniquesDocument19 pagesObturation TechniquesRere AaserNo ratings yet
- 4 Pit and FissureDocument74 pages4 Pit and FissureAME DENTAL COLLEGE RAICHUR, KARNATAKANo ratings yet
- Restoration of Endodontically Treated TeethDocument7 pagesRestoration of Endodontically Treated TeethSuaeni Kurnia WirdaNo ratings yet
- Management of Deep Carious LesionDocument52 pagesManagement of Deep Carious LesionLaiba Asif RajputNo ratings yet
- Indirect Pulp Capping TechniqueDocument39 pagesIndirect Pulp Capping TechniqueEdo ArdiansahNo ratings yet
- DENT342-lec.21-1 2Document39 pagesDENT342-lec.21-1 2Zhilia MuhammedNo ratings yet
- Pit and Fissure Sealant in Prevention of Dental CariesDocument4 pagesPit and Fissure Sealant in Prevention of Dental CariesSyuhadaSetiawanNo ratings yet
- Endo & RestorativeDocument59 pagesEndo & RestorativeLoredana RaduNo ratings yet
- Pit and Fissure SealantsDocument34 pagesPit and Fissure SealantsSamridhi SrivastavaNo ratings yet
- Exam Questions Dental Material 41 To 71Document11 pagesExam Questions Dental Material 41 To 71jimmyNo ratings yet
- Pit and Fissure Sealants New-1Document32 pagesPit and Fissure Sealants New-1Krishnanunni KmNo ratings yet
- Lect 14 Preventive Dentistry - Dental SealantDocument8 pagesLect 14 Preventive Dentistry - Dental Sealantزهراء فاضل اجبير فعيلNo ratings yet
- Vital Pulp Therapy TechniquesDocument11 pagesVital Pulp Therapy TechniquesZeinab Mohamed MorsyNo ratings yet
- Group 2 Student List and Dental Sealant InformationDocument33 pagesGroup 2 Student List and Dental Sealant InformationFarhan AhmedNo ratings yet
- Managing Deep Carious Lesions and Pulp ExposuresDocument11 pagesManaging Deep Carious Lesions and Pulp ExposuresDt omarNo ratings yet
- Management of Deep Carious LesionsDocument6 pagesManagement of Deep Carious Lesionsrujul_parikh_ind100% (1)
- CBL ENGLISH BLOK 7 - Fissure Sealant Procedure and PreventionDocument7 pagesCBL ENGLISH BLOK 7 - Fissure Sealant Procedure and PreventionIfata RDNo ratings yet
- Lec.6 Operative And Esthetic Dentistry اشرش ب .د يدعسDocument5 pagesLec.6 Operative And Esthetic Dentistry اشرش ب .د يدعسHayder MaqsadNo ratings yet
- Managing Deep Caries LesionsDocument5 pagesManaging Deep Caries LesionsEmeka V. ObiNo ratings yet
- Pit and Fissure SealantsDocument5 pagesPit and Fissure SealantsAkram HatamNo ratings yet
- New Approach in Restorative DentistryDocument6 pagesNew Approach in Restorative Dentistryبان منذر قدوريNo ratings yet
- Pit and Fissure SealantsDocument44 pagesPit and Fissure Sealantsmksweda10No ratings yet
- HapticsDocument11 pagesHapticsmehtakruti1021No ratings yet
- Rinse thoroughly with water and dry with compressed airDocument56 pagesRinse thoroughly with water and dry with compressed airهجرسNo ratings yet
- Restorative Dentistry for ChildrenDocument62 pagesRestorative Dentistry for Childrensamar yousif mohamedNo ratings yet
- Public Health DentistryDocument24 pagesPublic Health Dentistryananya saxenaNo ratings yet
- Pit and Fissure Sealants: Preventive DentistryDocument10 pagesPit and Fissure Sealants: Preventive Dentistryبان منذر قدوريNo ratings yet
- Mohamad Jalloul Endo Assign 2023Document13 pagesMohamad Jalloul Endo Assign 2023AliciaNo ratings yet
- Preventive care for dental patientsDocument14 pagesPreventive care for dental patientsMohamed NabilNo ratings yet
- Final Prof Lecture On Pit and Fissure Sealant PDFDocument51 pagesFinal Prof Lecture On Pit and Fissure Sealant PDFDrBhawna AroraNo ratings yet
- Clinical techniques for composite restoration placementDocument4 pagesClinical techniques for composite restoration placementRizta RiztiaNo ratings yet
- Lecture 4 Pit and FissureDocument7 pagesLecture 4 Pit and FissureKhaled Al-haddadNo ratings yet
- Pit and Fissure SealantDocument3 pagesPit and Fissure SealantSaugat DasNo ratings yet
- Pit and Fissure SealantsDocument35 pagesPit and Fissure SealantsshrutiNo ratings yet
- Treatment of Carious Primary TeethDocument32 pagesTreatment of Carious Primary TeethruchikaNo ratings yet
- Final StagesDocument18 pagesFinal StagesshimaambadawyNo ratings yet
- Ijss Feb Cr16Document5 pagesIjss Feb Cr16Pascal FilioNo ratings yet
- Relation Between Periodontics and Other Dental FieldsDocument9 pagesRelation Between Periodontics and Other Dental FieldsZakria Al-HadadNo ratings yet
- CariesDocument13 pagesCarieshosam ahmedNo ratings yet
- TIEDocument4 pagesTIEIrwandi MuslimNo ratings yet
- Răng trẻ emDocument39 pagesRăng trẻ emHoàng Đức NghĩaNo ratings yet
- Pits and Fissure Sealants ExplainedDocument22 pagesPits and Fissure Sealants ExplainedmisdduaaNo ratings yet
- Dis ColorDocument13 pagesDis ColortarekrabiNo ratings yet
- Penetration DepthDocument8 pagesPenetration DepthSahasraNo ratings yet
- Pit and Fissure Sealing Is Defined As The Application and Mechanical Bonding of A Resin Material To An AcidDocument2 pagesPit and Fissure Sealing Is Defined As The Application and Mechanical Bonding of A Resin Material To An AcidSanchit RaoNo ratings yet
- Fate of Extruded SealersDocument5 pagesFate of Extruded SealersRedhabAbbassNo ratings yet
- Hall Technique for Sealing CariesDocument2 pagesHall Technique for Sealing CariesElectricken21No ratings yet
- Microleakage Evaluation of Two Types of Fissure Sealants After Enamel Surface Pretreatment With Erbium Chromium LaserDocument14 pagesMicroleakage Evaluation of Two Types of Fissure Sealants After Enamel Surface Pretreatment With Erbium Chromium Lasereman.moheb22No ratings yet
- Pulp Protection and Cavity Liners in Operative DentistryDocument21 pagesPulp Protection and Cavity Liners in Operative DentistryRashed ShannanNo ratings yet
- Pulpotomy ProcedureDocument5 pagesPulpotomy ProcedureAseelNo ratings yet
- Pit and Fissure SealantsDocument35 pagesPit and Fissure Sealantsfajar dwi anggono100% (1)
- Devitalizing Agents, Non-Vital Methods of Root Canal Therapy, Non-Vital Pulpotomy and Pulpectomy, Indications, Description of TechniquesDocument45 pagesDevitalizing Agents, Non-Vital Methods of Root Canal Therapy, Non-Vital Pulpotomy and Pulpectomy, Indications, Description of TechniquesGeorgeNo ratings yet
- Pit and Fissure SealantsDocument19 pagesPit and Fissure SealantsAkshay Sreeraman KecheryNo ratings yet
- Hospitalised Sports Injury in Australia, 2016-17: Published February 2020Document20 pagesHospitalised Sports Injury in Australia, 2016-17: Published February 2020Mohammed TarekNo ratings yet
- Management of A Bilateral Mandibular Fracture in A Single-Humped CamelDocument4 pagesManagement of A Bilateral Mandibular Fracture in A Single-Humped CamelMohammed TarekNo ratings yet
- R O RO R O RO /RH R O /RH RO /RH R O /RH RO Oxidation StateDocument1 pageR O RO R O RO /RH R O /RH RO /RH R O /RH RO Oxidation StateMohammed TarekNo ratings yet
- The Epidemiology of Mandibular Fractures Treated at Chiang Mai University Hospital: A Review of 198 CasesDocument7 pagesThe Epidemiology of Mandibular Fractures Treated at Chiang Mai University Hospital: A Review of 198 CasesMohammed TarekNo ratings yet
- Oral Surgery Guide by Dr. Labeed SamiDocument22 pagesOral Surgery Guide by Dr. Labeed SamiMohammed TarekNo ratings yet
- Introduction to Computers and C++ Programming ChapterDocument38 pagesIntroduction to Computers and C++ Programming Chapterken lacedaNo ratings yet
- Relationship Between Mandible Fractures and Third Molars: Archives of Craniofacial SurgeryDocument6 pagesRelationship Between Mandible Fractures and Third Molars: Archives of Craniofacial SurgeryMohammed TarekNo ratings yet
- Periodic Table of The Elements: Atomic Number Symbol NameDocument1 pagePeriodic Table of The Elements: Atomic Number Symbol Namechen haoNo ratings yet
- HPS Per Table With SPDF Ions and Families To PostDocument87 pagesHPS Per Table With SPDF Ions and Families To PostMohammed TarekNo ratings yet
- Mendeleev's Periodic Table of The ElementsDocument20 pagesMendeleev's Periodic Table of The ElementsMohammed TarekNo ratings yet
- 3A The Periodic TableDocument7 pages3A The Periodic TableMohammed TarekNo ratings yet
- Mendeleev's Periodic Table of The ElementsDocument20 pagesMendeleev's Periodic Table of The ElementsMohammed TarekNo ratings yet
- Tierny Visualization Introductionc++Document26 pagesTierny Visualization Introductionc++DurandNo ratings yet
- PDDocument1 pagePDMohammed TarekNo ratings yet
- Computer10to12 2008 PDFDocument72 pagesComputer10to12 2008 PDFA YoungeNo ratings yet
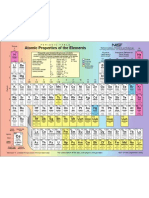
- Atomic Properties of The Elements TableDocument1 pageAtomic Properties of The Elements TableMaahiNo ratings yet
- Periodic Table IsotopesDocument1 pagePeriodic Table IsotopeslamantreveurNo ratings yet
- MR Robot 1x01 - PilotDocument64 pagesMR Robot 1x01 - Pilotchosen_one_dtnNo ratings yet
- EndoDocument1 pageEndoMohammed TarekNo ratings yet
- Material de ApoyoDocument57 pagesMaterial de ApoyoALEXANDER MONDRAGON DIAZNo ratings yet
- Introduction To Endocrine Disrupting ChemicalsDocument76 pagesIntroduction To Endocrine Disrupting ChemicalsMohammed TarekNo ratings yet
- ENDO Agar: Mode of Action LiteratureDocument2 pagesENDO Agar: Mode of Action LiteratureadiazcalidadNo ratings yet
- ERN On Endocrine Conditions (Endo-ERN)Document1 pageERN On Endocrine Conditions (Endo-ERN)Mohammed TarekNo ratings yet
- 1462 PDFDocument5 pages1462 PDFMohammed TarekNo ratings yet
- CC - MVSA0147 Report Great Barrier Reef - V4 FA - Low Res - Single PagesDocument32 pagesCC - MVSA0147 Report Great Barrier Reef - V4 FA - Low Res - Single PagesMohammed TarekNo ratings yet
- Metabolic Changes by Wine Flor-Yeasts With Gluconic Acid As The Sole Carbon SourceDocument15 pagesMetabolic Changes by Wine Flor-Yeasts With Gluconic Acid As The Sole Carbon SourceMohammed TarekNo ratings yet
- Endo EngDocument107 pagesEndo EngMohammed TarekNo ratings yet
- Chlorine Bleach Sanitizing GuideDocument2 pagesChlorine Bleach Sanitizing GuidearjmandquestNo ratings yet
- Research Article: Characterization, Acid Activation, and Bleaching Performance of Ibeshe Clay, Lagos, NigeriaDocument6 pagesResearch Article: Characterization, Acid Activation, and Bleaching Performance of Ibeshe Clay, Lagos, NigeriarmburraNo ratings yet
- Tooth Bleaching - Tooth Whitening (May 2013) (SHC 8782)Document19 pagesTooth Bleaching - Tooth Whitening (May 2013) (SHC 8782)Mohammed TarekNo ratings yet
- Bds PDFDocument227 pagesBds PDFAiswaryaNo ratings yet
- Xylitol For HealthDocument24 pagesXylitol For HealthDonald WehmeyerNo ratings yet
- Step-by-Step Techniques for Bulk-Fill Composite RestorationsDocument9 pagesStep-by-Step Techniques for Bulk-Fill Composite RestorationssusethNo ratings yet
- Vital Pulp Therapy and Regeneration: Prof. Abeer ElgendyDocument22 pagesVital Pulp Therapy and Regeneration: Prof. Abeer ElgendyNasser HashimNo ratings yet
- Dental Enamel CompositionDocument5 pagesDental Enamel CompositionARJUN Sreenivas100% (1)
- Gic SandwichDocument6 pagesGic Sandwich12345sagarNo ratings yet
- Pulpal DiagnosisDocument14 pagesPulpal DiagnosisSimina LungociNo ratings yet
- Pop Research PaperDocument14 pagesPop Research Paperapi-253449395No ratings yet
- BIODENTINE EndovitalDocument8 pagesBIODENTINE EndovitalLupu SebastianNo ratings yet
- Bo Suu Tap 2 Chon HSG Tieng Anh Lop 9Document100 pagesBo Suu Tap 2 Chon HSG Tieng Anh Lop 9Thảo Nguyên HồNo ratings yet
- Short GuidelinesDocument52 pagesShort GuidelinesMohamed FaizalNo ratings yet
- Sectional Matrix: Step-By-Step Directions For Their Clinical UseDocument5 pagesSectional Matrix: Step-By-Step Directions For Their Clinical UseRaniyah Az-zahraNo ratings yet
- Oral Health of Elephant KeepersDocument2 pagesOral Health of Elephant KeepersdilrukshiNo ratings yet
- Diet and Dental CariesDocument84 pagesDiet and Dental CariesArun MamachanNo ratings yet
- ProtrkaDocument8 pagesProtrkaMihaela VasiliuNo ratings yet
- Pediatric Oral HealthDocument172 pagesPediatric Oral HealthArif HidayatNo ratings yet
- Memo FormatDocument60 pagesMemo FormatJulieto ResusNo ratings yet
- V I Y M: Dissertations/Theses Undertaken at The Faculty of Dentistry UNI ERS T OF Alaya For The Year 2009Document19 pagesV I Y M: Dissertations/Theses Undertaken at The Faculty of Dentistry UNI ERS T OF Alaya For The Year 2009Hoshang AbdelrahmanNo ratings yet
- Comparitive Study Colgate and PepsodentDocument10 pagesComparitive Study Colgate and PepsodentSunil MathewsNo ratings yet
- Prevention of Periodontal Disease HandoutDocument13 pagesPrevention of Periodontal Disease HandoutShady AnwarNo ratings yet
- BOOKDocument6 pagesBOOKAnoop maniNo ratings yet
- The Invisible Toothbrush-Emmanuel CheraskinDocument10 pagesThe Invisible Toothbrush-Emmanuel CheraskinDavidNo ratings yet
- Fdi-Oral Cancer-Prevention and Patient ManagementDocument12 pagesFdi-Oral Cancer-Prevention and Patient ManagementNindy PutriNo ratings yet
- Kode Icd X (Gigi)Document5 pagesKode Icd X (Gigi)Lia CitraNo ratings yet
- 0 Enamel FactoidDocument6 pages0 Enamel FactoidmoffittajNo ratings yet