You might also like
- Edan (Onile) Orisa - Ogboni (Osugbo) - Yoruba HistoryDocument4 pagesEdan (Onile) Orisa - Ogboni (Osugbo) - Yoruba Historychveloso75% (4)
- Manual of HeraldryDocument146 pagesManual of HeraldryTrung Tiên100% (1)
- Grant ProposalDocument18 pagesGrant Proposalapi-582889983No ratings yet
- Intensive Behavioral Therapy For Autism Spectrum Disorders: Coverage RationaleDocument14 pagesIntensive Behavioral Therapy For Autism Spectrum Disorders: Coverage Rationalediana100% (1)
- Wells Brief Cognitive Therapy For Social Phobia - A Case SeriesDocument8 pagesWells Brief Cognitive Therapy For Social Phobia - A Case SeriesjuaromerNo ratings yet
- SEC vs. Universal RightfieldDocument3 pagesSEC vs. Universal RightfieldCaitlin KintanarNo ratings yet
- Reyes-Ortega 2019 ACT or DBT or Both - With Borderline Personality DisorderDocument16 pagesReyes-Ortega 2019 ACT or DBT or Both - With Borderline Personality DisorderMario Lopez PadillaNo ratings yet
- What Is Round Robin SchedulingDocument5 pagesWhat Is Round Robin Schedulingtridibearth100% (3)
- Parallel Lines and TransversalsDocument15 pagesParallel Lines and TransversalsJasmin Move-RamirezNo ratings yet
- French Revolution NotesDocument19 pagesFrench Revolution Notesaksekhon13No ratings yet
- Pre-Post OT InterventionDocument16 pagesPre-Post OT InterventionIdanerlisNo ratings yet
- Organizational Behavior CH 4 Mcqs PDFDocument4 pagesOrganizational Behavior CH 4 Mcqs PDFAzeem KhanNo ratings yet
- Salazar v. CFIDocument2 pagesSalazar v. CFILouie BruanNo ratings yet
- PALE Casals v. CusiDocument2 pagesPALE Casals v. CusiCharm Pedrozo100% (1)
- Assignment Money Cash Flow Inc Group 21,23,27,30Document3 pagesAssignment Money Cash Flow Inc Group 21,23,27,30Karan Vashee100% (3)
- MindfulnessDocument14 pagesMindfulnessRosa SecoNo ratings yet
- Grade 5 DLL English 5 Q2 Week 6Document4 pagesGrade 5 DLL English 5 Q2 Week 6kotarobrother2350% (2)
- British J Clinic Psychol - 2018 - Romero Mart Nez - Improving Empathy With Motivational Strategies in Batterer InterventionDocument15 pagesBritish J Clinic Psychol - 2018 - Romero Mart Nez - Improving Empathy With Motivational Strategies in Batterer InterventionNicolás MossoNo ratings yet
- Clinical Efficacy of A Combined AcceptanDocument16 pagesClinical Efficacy of A Combined AcceptanEmanuel EspinosaNo ratings yet
- Rey - Cyberbullying Victimization and Somatic ComplaintsDocument5 pagesRey - Cyberbullying Victimization and Somatic ComplaintsJohanna FejerNo ratings yet
- Emotion Regulation and Experiential AviodanceDocument29 pagesEmotion Regulation and Experiential Aviodancealexandra rivasNo ratings yet
- Versión Española Maunal Transdiagnóstico Ansiedad DepresiónDocument18 pagesVersión Española Maunal Transdiagnóstico Ansiedad DepresiónMiguel QuezadaNo ratings yet
- Effect Emotional Intelligence in Prevention of ViolenceDocument11 pagesEffect Emotional Intelligence in Prevention of ViolenceEva GonNo ratings yet
- Treatment Resistant Perpetrators of Intimate Partner ViolenceResearch AdvancesDocument4 pagesTreatment Resistant Perpetrators of Intimate Partner ViolenceResearch AdvancesAbigail MJNo ratings yet
- Abstract STD (In English)Document2 pagesAbstract STD (In English)Luiz Henrique Sampaio JuniorNo ratings yet
- Journal of Contextual Behavioral Science: Marge A. Sierra, Eliana OrtizDocument12 pagesJournal of Contextual Behavioral Science: Marge A. Sierra, Eliana OrtizEliana Ortiz GarzonNo ratings yet
- Emotional Regulation and Interpersonal Effectiveness As Mechanisms of Change For Treatment Outcomes Within A DBT Program For AdolescentsDocument13 pagesEmotional Regulation and Interpersonal Effectiveness As Mechanisms of Change For Treatment Outcomes Within A DBT Program For AdolescentsLauraLoaizaNo ratings yet
- Healthcare 2148202 2Document20 pagesHealthcare 2148202 2Andres RamirezNo ratings yet
- Running Head: Increased Effectiveness of Sensory Integration With AutismDocument15 pagesRunning Head: Increased Effectiveness of Sensory Integration With Autismapi-340625860No ratings yet
- Stigma and Outcome of Treatment Among Patients With Psychological Disorders and Their AttendersDocument5 pagesStigma and Outcome of Treatment Among Patients With Psychological Disorders and Their AttendersFathima ZoharaNo ratings yet
- Young 2015Document11 pagesYoung 2015PhilipNo ratings yet
- Treating Women Who Have Experienced Intimate Partner ViolenceDocument12 pagesTreating Women Who Have Experienced Intimate Partner ViolenceMyriam Hernández NúñezNo ratings yet
- Alzh 1 ART Intervenciones Psicosocial y Conductual en Demencia-BurnsDocument5 pagesAlzh 1 ART Intervenciones Psicosocial y Conductual en Demencia-BurnsKitzia AveiriNo ratings yet
- PsychologicalDocument7 pagesPsychologicalPragati PrakashNo ratings yet
- 10 14710@nmjn V10i1 22220Document11 pages10 14710@nmjn V10i1 22220Isabel CuevasNo ratings yet
- Acceptance and Commitment Therapy Focused On Repetitive Negative Thinking For Child Depression - A Randomized Multiple-Baseline EvaluationDocument18 pagesAcceptance and Commitment Therapy Focused On Repetitive Negative Thinking For Child Depression - A Randomized Multiple-Baseline EvaluationVíctor CaparrósNo ratings yet
- Version of Record:: ManuscriptDocument20 pagesVersion of Record:: ManuscriptElizabeth Roxan Lizaso GonzálezNo ratings yet
- Emotion Regulation Framework PreprintDocument53 pagesEmotion Regulation Framework PreprintAndreia SilvaNo ratings yet
- Effects of Attachment-Based Compassion Therapy (ABCT) On Self-Compassion and Attachment Style in Healthy PeopleDocument12 pagesEffects of Attachment-Based Compassion Therapy (ABCT) On Self-Compassion and Attachment Style in Healthy PeopleAoiNo ratings yet
- Relationship Between EmotionalDocument6 pagesRelationship Between Emotionalsebastian manga sanchezNo ratings yet
- Running Head: Sensory Integration TherapyDocument12 pagesRunning Head: Sensory Integration Therapyapi-380681224No ratings yet
- International Journal of Clinical and Health Psychology: Original ArticleDocument8 pagesInternational Journal of Clinical and Health Psychology: Original Articlealejandra sarmientoNo ratings yet
- Treating Somatization: A Multimodal ApproachDocument7 pagesTreating Somatization: A Multimodal ApproachDr. Ranjan KumarNo ratings yet
- Herrero Aulet Et Al 2019 - Art Ni.18035.herDocument29 pagesHerrero Aulet Et Al 2019 - Art Ni.18035.herJaume Grané MorcilloNo ratings yet
- Fernandez 2022 Smartphone Famliy ConnectionsDocument7 pagesFernandez 2022 Smartphone Famliy ConnectionsBrayan PomaNo ratings yet
- J Jcbs 2019 02 005Document36 pagesJ Jcbs 2019 02 005kenth yuNo ratings yet
- Opoka 2021Document15 pagesOpoka 2021aliceNo ratings yet
- Coping I Mysli SamobojczeDocument19 pagesCoping I Mysli SamobojczePiotr Sylwester WojdaNo ratings yet
- NRES ChapterDocument16 pagesNRES ChapterScytllaNo ratings yet
- Mobile Health (Mhealth) Versus Clinic-Based Group Intervention For People With Serious Mental Illness: A Randomized Controlled TrialDocument8 pagesMobile Health (Mhealth) Versus Clinic-Based Group Intervention For People With Serious Mental Illness: A Randomized Controlled TrialOlivia NasarreNo ratings yet
- Effectiveness of Acceptance and Commitment TherapyDocument8 pagesEffectiveness of Acceptance and Commitment TherapySreejith RamadasanNo ratings yet
- The Mediating Role of Cognitive Reappraisal Between Childhood Physical Abuse and Substance Abuse Among Young Adult Residents in A Selected Treatment and Rehabilitation Center in BicutanDocument14 pagesThe Mediating Role of Cognitive Reappraisal Between Childhood Physical Abuse and Substance Abuse Among Young Adult Residents in A Selected Treatment and Rehabilitation Center in BicutanPsychology and Education: A Multidisciplinary JournalNo ratings yet
- Believing Is Doing: Emotion Regulation Beliefs Are Associated With Emotion Regulation Behavioral Choices and Subjective Well-BeingDocument15 pagesBelieving Is Doing: Emotion Regulation Beliefs Are Associated With Emotion Regulation Behavioral Choices and Subjective Well-BeingChelsey XieNo ratings yet
- 2020 Anderson Finkelstein and Horvath Fis Skills Method and Difficult Therapy MomentsDocument7 pages2020 Anderson Finkelstein and Horvath Fis Skills Method and Difficult Therapy MomentsMouloud HAMMOUCHNo ratings yet
- Predictors of Changes in Alcohol-Related Self-Efficacy Over 16 YearsDocument8 pagesPredictors of Changes in Alcohol-Related Self-Efficacy Over 16 Yearsalexandra mariaNo ratings yet
- Archives of Psychiatric Nursing: Ebru Akbas, Gülay Tas Demir Yi Gito GluDocument9 pagesArchives of Psychiatric Nursing: Ebru Akbas, Gülay Tas Demir Yi Gito GluSiti NurfathiniNo ratings yet
- Protocolo Unificado Tratamento Transdiagnóstico 01Document14 pagesProtocolo Unificado Tratamento Transdiagnóstico 01Augusto Duarte Faria100% (1)
- The Effect of Application of Nurse Therapeutic Communication On Cooperative Behavior of Patients With Mental DisordersDocument7 pagesThe Effect of Application of Nurse Therapeutic Communication On Cooperative Behavior of Patients With Mental DisordersRosa SheilaaaNo ratings yet
- ACTforPsychosisRecovery Chapter 1Document25 pagesACTforPsychosisRecovery Chapter 1quentelllNo ratings yet
- Ifransiska,+3 +maryatun-FixDocument13 pagesIfransiska,+3 +maryatun-FixALFIATUR RahmiNo ratings yet
- A Systematic Review and Psychometric Evaluation of Self-Report HoardingDocument45 pagesA Systematic Review and Psychometric Evaluation of Self-Report HoardingAmita GoyalNo ratings yet
- RESUMEN POSTERS - ACBS Annual World Conference 13 (Berlín, 2015)Document138 pagesRESUMEN POSTERS - ACBS Annual World Conference 13 (Berlín, 2015)LandoGuillénChávezNo ratings yet
- ContentServer PDFDocument15 pagesContentServer PDFMaginta Resy DianaNo ratings yet
- Grade 11 ResearchDocument33 pagesGrade 11 ResearchVon Kurt M. SausNo ratings yet
- Effectiveness of A Cognitive Behavioral Group Therapy Program For Reducing Violence Risk in Persons With SchizophreniaDocument5 pagesEffectiveness of A Cognitive Behavioral Group Therapy Program For Reducing Violence Risk in Persons With Schizophreniacamuss23No ratings yet
- Pilot Study of A Psuchotherapeuetic Intervention For Reducing Guilt Feelings in Highlt Distressed Dementia Family CareregiversDocument11 pagesPilot Study of A Psuchotherapeuetic Intervention For Reducing Guilt Feelings in Highlt Distressed Dementia Family CareregiversCristina MPNo ratings yet
- The Future of Psychology Compassion-Focused Outcomes & Using Technology To Increase Compassion Worldwide - Yotam HeinebergDocument28 pagesThe Future of Psychology Compassion-Focused Outcomes & Using Technology To Increase Compassion Worldwide - Yotam HeinebergccareemailNo ratings yet
- Long-Term Efficacy of Psychosocial Treatments For Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic ReviewDocument24 pagesLong-Term Efficacy of Psychosocial Treatments For Adults With Attention-Deficit/Hyperactivity Disorder: A Meta-Analytic Reviewaastha panthNo ratings yet
- Interventions of Choice For THDocument13 pagesInterventions of Choice For THgs67461No ratings yet
- Practical Guide to Child and Adolescent Psychological TestingFrom EverandPractical Guide to Child and Adolescent Psychological TestingNo ratings yet
- Light-Reflection and Refraction PPT 1Document42 pagesLight-Reflection and Refraction PPT 1api-285160905No ratings yet
- Practice English TestDocument5 pagesPractice English Testmahboobulhaq0% (1)
- INF2004 2007 Mid-Term Test (DBMS)Document18 pagesINF2004 2007 Mid-Term Test (DBMS)ruchi1697No ratings yet
- Genome Browser ExerciseDocument5 pagesGenome Browser ExerciseyukiNo ratings yet
- Case Law AnalysisDocument8 pagesCase Law Analysisapi-309579746No ratings yet
- (1989) 3 W.L.R. 1150Document43 pages(1989) 3 W.L.R. 1150pieremicheleNo ratings yet
- Judean Ministry SampleDocument15 pagesJudean Ministry SampleCherian Mathews100% (1)
- Personal Development PlanDocument5 pagesPersonal Development PlanMUHAMMAD UMER 16093No ratings yet
- E500 FD Rel11 Part1 OverviewDocument35 pagesE500 FD Rel11 Part1 OverviewЖорж КаназирскиNo ratings yet
- Interdisciplinary ResearchDocument17 pagesInterdisciplinary ResearchFazil HassanNo ratings yet
- Factors Influencing LearningDocument12 pagesFactors Influencing Learningrosmery15No ratings yet
- Renaissance Thesis TopicsDocument7 pagesRenaissance Thesis Topicssherielliottbillings100% (2)
- Press Release Hit and RunDocument2 pagesPress Release Hit and RunAnthony_Smith4792No ratings yet
- 02 Yujuico V AtienzaDocument24 pages02 Yujuico V AtienzaJm CruzNo ratings yet
- De Thi Giua Ki 2 Tieng Anh 11 Global Success de So 2 1706520556Document4 pagesDe Thi Giua Ki 2 Tieng Anh 11 Global Success de So 2 1706520556trangnguyen23092007No ratings yet
- MaterialDocument5 pagesMaterialEsty LestariNo ratings yet
- A. Look at The Pictures. Write The Words. 1. 2Document20 pagesA. Look at The Pictures. Write The Words. 1. 2CHIEN HUA SJKCNo ratings yet
- A Snake and The MirrorDocument65 pagesA Snake and The Mirroralone smoothNo ratings yet
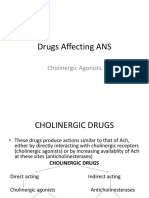
- Drugs Affecting ANS: Cholinergic AgonistsDocument25 pagesDrugs Affecting ANS: Cholinergic AgonistsAjay SinghNo ratings yet