You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Avfistula or Tunnelled Catheter For Haemodialysis Jok 1000e102Document1 pageAvfistula or Tunnelled Catheter For Haemodialysis Jok 1000e102tenty isniNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Cardiac Complications of Arteriovenous Fistulas in Patients With End-Stage Renal DiseaseDocument12 pagesCardiac Complications of Arteriovenous Fistulas in Patients With End-Stage Renal Diseasetenty isniNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Atrial Fibrillation and Thromboembolism in Patients With Chronic Kidney DiseaseDocument13 pagesAtrial Fibrillation and Thromboembolism in Patients With Chronic Kidney Diseasetenty isniNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Haemodialysis Journey From The West To The EastDocument7 pagesA Haemodialysis Journey From The West To The Easttenty isniNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Administration of Alpha1 Antitrypsin in Haemodialysis KDC 1000102Document3 pagesAdministration of Alpha1 Antitrypsin in Haemodialysis KDC 1000102tenty isniNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Jadwal Zaal Anak-1Document20 pagesJadwal Zaal Anak-1tenty isniNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
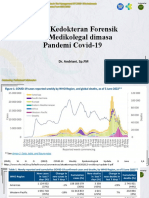
- Peran Kedokteran ForensikDocument63 pagesPeran Kedokteran Forensiktenty isniNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Role of Imaging in Post Pnemumonia COVID-19Document22 pagesRole of Imaging in Post Pnemumonia COVID-19tenty isniNo ratings yet
- Diagnostik Dasar Radiologis COVID-19Document42 pagesDiagnostik Dasar Radiologis COVID-19tenty isniNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- EWS and Triage in COVID - 19 FIXDocument26 pagesEWS and Triage in COVID - 19 FIXtenty isniNo ratings yet
- Anti Inflammasi Pada Covid 19Document54 pagesAnti Inflammasi Pada Covid 19tenty isniNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- 6.miocard Infarction in COVID-19Document37 pages6.miocard Infarction in COVID-19tenty isniNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- RSOP Patient TransportationDocument6 pagesRSOP Patient TransportationE.m. SoorajNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Anal Fistula2Document43 pagesAnal Fistula2api-19641337No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- CMR - Guide - 2nd - Edition - 148x105mm - 03may2017 - Last VersionDocument124 pagesCMR - Guide - 2nd - Edition - 148x105mm - 03may2017 - Last VersionCristián Martínez BocazNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Radiesse - Advanced Techniques and Applications For A Unique and Versatile ImplantDocument7 pagesRadiesse - Advanced Techniques and Applications For A Unique and Versatile ImplantAnonymous LnWIBo1G100% (2)
- Acyanotic Congenital Heart Disease: Left-to-Right Shunt LesionsDocument17 pagesAcyanotic Congenital Heart Disease: Left-to-Right Shunt LesionsAgustinaNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Developing Human Clinically Oriented Embryology 10th Edition Moore Test BankDocument9 pagesDeveloping Human Clinically Oriented Embryology 10th Edition Moore Test Bankryanrhodestobgjkeicr100% (27)
- 00010asdfDocument3 pages00010asdfthzone1986No ratings yet
- Orthopedic PathologyDocument2 pagesOrthopedic PathologyvetpathforumNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Distal Radius FracturesDocument115 pagesDistal Radius FracturesRahimulla Hamid100% (2)
- Cardiovascular SystemDocument3 pagesCardiovascular Systemhz1588No ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Transabdominal Esophago-Cutaneous Fistula Closure With Endoscopic Negative Pressure Therapy Using A Thin Open-Pore Film Drain in A Pull-Through Technique PDFDocument2 pagesTransabdominal Esophago-Cutaneous Fistula Closure With Endoscopic Negative Pressure Therapy Using A Thin Open-Pore Film Drain in A Pull-Through Technique PDFMilan JovicNo ratings yet
- Case Scenario - Week 4 - Group 2Document34 pagesCase Scenario - Week 4 - Group 2Angel Hannah100% (1)
- ASN 085.12 - WorldTracer System Enhancement UpdatesDocument3 pagesASN 085.12 - WorldTracer System Enhancement UpdatesBurcu Yıldız100% (2)
- Head To Toe Assessment GuideDocument3 pagesHead To Toe Assessment GuideUmer Masood0% (1)
- Periodontal Accelerated Osteogenic Orthodontics Technique For RapidDocument10 pagesPeriodontal Accelerated Osteogenic Orthodontics Technique For RapidATZIRI CHAVEZ PORTILLONo ratings yet
- Journal Club Gut PrepDocument14 pagesJournal Club Gut PrepMohammad NomanNo ratings yet
- ATLS RangkumanDocument162 pagesATLS RangkumanA. Muh. IksanNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Sme Package Summary of Benefits (2305843009215646953)Document7 pagesSme Package Summary of Benefits (2305843009215646953)RIVERA - SARVIDA CONSTRUCTION INC.No ratings yet
- Fixed ProsthodonticsDocument11 pagesFixed ProsthodonticsArxhenta ÇupiNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Apollo Hospital Press Release 5 02 Sept 14Document2 pagesApollo Hospital Press Release 5 02 Sept 14LUKAZA2013No ratings yet
- 64 - Skin TumorsDocument20 pages64 - Skin TumorsAlexa GabrielaNo ratings yet
- Critical Care Nephrology Core Curriculum 2019Document34 pagesCritical Care Nephrology Core Curriculum 2019Edmilson R. LimaNo ratings yet
- 062012SCNADocument11 pages062012SCNAMc KobaNo ratings yet
- 2020 Taiwan - Acute Pancreatitis GuidelineDocument10 pages2020 Taiwan - Acute Pancreatitis Guideline吳任爵No ratings yet
- Benign Prostatic Hyperplasia (BPH)Document8 pagesBenign Prostatic Hyperplasia (BPH)miftah ar rahmahNo ratings yet
- Anatomy Notes by Drmayur SaytaDocument180 pagesAnatomy Notes by Drmayur SaytaRaiyani NidhiNo ratings yet
- Grade Ruptur RosadeDocument31 pagesGrade Ruptur RosadeAntoniusNo ratings yet
- MOCKBOARD PART 3 Answer KeyDocument23 pagesMOCKBOARD PART 3 Answer KeyJayrald CruzadaNo ratings yet
- List of Abbreviations: (French)Document9 pagesList of Abbreviations: (French)Maurine SampangNo ratings yet
- Laparoscopy and Laparoscopic SurgeryDocument7 pagesLaparoscopy and Laparoscopic SurgeryLaura RojasNo ratings yet