You might also like
- HBA1CDocument17 pagesHBA1CMiguel Enrique Castro CruzNo ratings yet
- HbA1c Reageant KitsDocument4 pagesHbA1c Reageant KitsMichael TanglaoNo ratings yet
- EN - HEMOGLOBIN A1cDocument4 pagesEN - HEMOGLOBIN A1cأنا الجفاNo ratings yet
- Apolipoprotein BDocument13 pagesApolipoprotein BcarineNo ratings yet
- Hba1C HPLC Assay: Package InsertDocument9 pagesHba1C HPLC Assay: Package InsertKery B. SantsNo ratings yet
- Upload 00000340 1667845764873Document4 pagesUpload 00000340 1667845764873M.AhmedNo ratings yet
- Cormay Hba Direct: Diagnostic Kit For Determination of Haemoglobin A Concentration Ii GenerationDocument2 pagesCormay Hba Direct: Diagnostic Kit For Determination of Haemoglobin A Concentration Ii GenerationTrần Văn BìnhNo ratings yet
- SYNCHRON System(s) Chemistry Information Sheet HDL CholesterolDocument11 pagesSYNCHRON System(s) Chemistry Information Sheet HDL CholesterolanggaririnNo ratings yet
- Hemoglobin A1c Reagent SetDocument2 pagesHemoglobin A1c Reagent SetAde FeriyatnaNo ratings yet
- HBA1C AbcDocument2 pagesHBA1C AbcmrashrafiNo ratings yet
- GHbA1cDocument3 pagesGHbA1cAmos Babu JettiNo ratings yet
- Hba C Glycated Hemoglobin: 1B 1B 1B 1BDocument2 pagesHba C Glycated Hemoglobin: 1B 1B 1B 1BvijayaNo ratings yet
- Lab Policies Hemoglobin A1C - Cobas c501 Lab 4004Document6 pagesLab Policies Hemoglobin A1C - Cobas c501 Lab 4004yosefinNo ratings yet
- Truechemie: Hba1C Test KitDocument2 pagesTruechemie: Hba1C Test KitAniket dubeyNo ratings yet
- Archem HbA1cDocument5 pagesArchem HbA1cTisha Patricia OedoyNo ratings yet
- Haemoglobin: Colorimetric Method (Cyanmethemoglobin)Document2 pagesHaemoglobin: Colorimetric Method (Cyanmethemoglobin)Rury Darwa NingrumNo ratings yet
- Catalog : Alcohol Reagent SetDocument1 pageCatalog : Alcohol Reagent SetTrần Thanh ViệnNo ratings yet
- Bilirrubina DirectaDocument11 pagesBilirrubina DirectaMASSTTERNo ratings yet
- APOAT enDocument3 pagesAPOAT enYunita RapaNo ratings yet
- Measure HbA1c Levels AccuratelyDocument2 pagesMeasure HbA1c Levels AccuratelyTrần Văn BìnhNo ratings yet
- AlcoholDocument1 pageAlcoholtuan vănNo ratings yet
- HBA1C Kit Insert DiatekDocument1 pageHBA1C Kit Insert DiatekKurnia Lavigne0% (1)
- Apobt: Nacl Diluent 9%Document3 pagesApobt: Nacl Diluent 9%Yunita RapaNo ratings yet
- AlbuminaDocument4 pagesAlbuminaSuprovet LabotatorioNo ratings yet
- 8 AmylaseDocument9 pages8 AmylaseAzhar Clinical Laboratory TubeNo ratings yet
- Synchron System(s) Chemistry Information Sheet Gluh: GlucoseDocument16 pagesSynchron System(s) Chemistry Information Sheet Gluh: GlucosehongNo ratings yet
- Pointe Hemoglobin A1c InsertDocument2 pagesPointe Hemoglobin A1c InsertMario TogniniNo ratings yet
- Principle Principle PrincipleDocument12 pagesPrinciple Principle PrincipleDarshana JuvekarNo ratings yet
- Glycated Hba1CDocument2 pagesGlycated Hba1CMohammed Nasser AL-delphiNo ratings yet
- Infinity ACE Liquid Reagent ENDocument2 pagesInfinity ACE Liquid Reagent ENKOUAME EDYMAIN FRANCISNo ratings yet
- COD reagents measure protein concentrationDocument1 pageCOD reagents measure protein concentrationNisa Javadd100% (2)
- ALBUMIN BLOSR6x02 ENDocument2 pagesALBUMIN BLOSR6x02 ENMeethuanNo ratings yet
- A1C-2 Whole Blood enDocument6 pagesA1C-2 Whole Blood enSyahdie FahledieNo ratings yet
- Total Protein Test ProcedureDocument2 pagesTotal Protein Test ProcedureTrần Thanh ViệnNo ratings yet
- En AlbuminDocument2 pagesEn AlbuminCướpBiểnChộtNo ratings yet
- AU Instructions For Use Albumin: PrincipleDocument6 pagesAU Instructions For Use Albumin: PrincipleAnas TjNo ratings yet
- 14 CreatinineDocument8 pages14 CreatinineAzhar Clinical Laboratory TubeNo ratings yet
- A 1 CDocument8 pagesA 1 CRajiv RanjanNo ratings yet
- Alkaline Phosphatase Activity Test KitDocument2 pagesAlkaline Phosphatase Activity Test KitRury Darwa Ningrum100% (1)
- Bilirubin Total Blosr6x12 enDocument2 pagesBilirubin Total Blosr6x12 enMeethuanNo ratings yet
- Clonatest Amylase MRDocument4 pagesClonatest Amylase MRSuprovet LabotatorioNo ratings yet
- 1105000I Rev. 02Document2 pages1105000I Rev. 02Riadh BenyoucefNo ratings yet
- EN - CRP OSR Special ChemistryDocument7 pagesEN - CRP OSR Special ChemistryYến Minh NguyễnNo ratings yet
- Biomed AlbuminDocument2 pagesBiomed Albuminahmad FouadNo ratings yet
- 7 AmmoniaDocument7 pages7 AmmoniaAzhar Clinical Laboratory TubeNo ratings yet
- Hba1c BDocument1 pageHba1c BAjay ChauhanNo ratings yet
- Immunoscan CCPlus RA 96PLUS Multilingual E 23 0182 09Document135 pagesImmunoscan CCPlus RA 96PLUS Multilingual E 23 0182 09vijayaNo ratings yet
- EN - TOTAL PROTEIN - BAOSR6x32 - USDocument3 pagesEN - TOTAL PROTEIN - BAOSR6x32 - USDharmesh PatelNo ratings yet
- Microalbumin ReagentDocument5 pagesMicroalbumin Reagenttuan vănNo ratings yet
- Lyphase 11760I-Reagent A 510 Reagent B 300 Sample 9 Standard 113Document1 pageLyphase 11760I-Reagent A 510 Reagent B 300 Sample 9 Standard 113mahinNo ratings yet
- 2.AlbuminDocument2 pages2.AlbuminHiếu Chí PhanNo ratings yet
- GA4256 00 - Direct BilirubinDocument2 pagesGA4256 00 - Direct BilirubinTrần Thanh ViệnNo ratings yet
- ALT Reagent Set Test for Liver EnzymeDocument2 pagesALT Reagent Set Test for Liver EnzymeJashmyn JagonapNo ratings yet
- 1.Alpha AmylaseDocument2 pages1.Alpha AmylaseHiếu Chí PhanNo ratings yet
- Α Α Α Α-Amylase-Eps: Biosystems S.ADocument1 pageΑ Α Α Α-Amylase-Eps: Biosystems S.ARisqon Anjahiranda AdiputraNo ratings yet
- HbA1c (09.09.16)Document12 pagesHbA1c (09.09.16)Sharom Zelene Cordova RomanNo ratings yet
- Hba1C Direct With Calibrator: 30 Days at 2-8°C. Do Not FreezeDocument2 pagesHba1C Direct With Calibrator: 30 Days at 2-8°C. Do Not FreezeSanjay KumarNo ratings yet
- Carbamazepine: Konelab™ / T SeriesDocument27 pagesCarbamazepine: Konelab™ / T SeriesKouame FrancisNo ratings yet
- Microalbumin Turbilatex - Liquid CalibratorDocument2 pagesMicroalbumin Turbilatex - Liquid CalibratorDinesh SreedharanNo ratings yet
- Hba1c (Hemoglobin A1c) Blosb00389-09 EnglishDocument12 pagesHba1c (Hemoglobin A1c) Blosb00389-09 EnglishVũng Tàu LabNo ratings yet
- No. 91-025 Mar. 01, 2006: APN-P - S215'M'Document1 pageNo. 91-025 Mar. 01, 2006: APN-P - S215'M'Vũng Tàu LabNo ratings yet
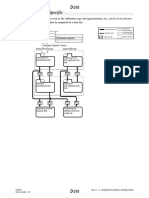
- M514 Manual Chapters on Special Operation and PlumbingDocument12 pagesM514 Manual Chapters on Special Operation and PlumbingVũng Tàu LabNo ratings yet
- Calib Phan UngDocument11 pagesCalib Phan UngVũng Tàu LabNo ratings yet
- (GUIDE) MLBB Dictionary - General Discussion - Mobile Legends - Bang Bang - Mobile - Powered by Discuz!Document7 pages(GUIDE) MLBB Dictionary - General Discussion - Mobile Legends - Bang Bang - Mobile - Powered by Discuz!Jenny Lyn MahinayNo ratings yet
- Elecius Franklin IndictmentDocument2 pagesElecius Franklin Indictmentthe kingfishNo ratings yet
- Financial Planning GodrejDocument199 pagesFinancial Planning GodrejriteshnaikNo ratings yet
- M.2 - R-Value References - Learn C++Document18 pagesM.2 - R-Value References - Learn C++njb25bcnqfNo ratings yet
- Group-5-Chapter-IV - Abstract, Summary, Conclusion, and ReccomendationDocument38 pagesGroup-5-Chapter-IV - Abstract, Summary, Conclusion, and Reccomendationjelian castroNo ratings yet
- Montessori Practical Life ExercisesDocument3 pagesMontessori Practical Life ExercisesSiti ShalihaNo ratings yet
- Domestic Violence Cycle of Violence Types of Families-2Document22 pagesDomestic Violence Cycle of Violence Types of Families-2api-340420872No ratings yet
- National Register of Large Dams -2019: Government of India Central Water CommissionDocument300 pagesNational Register of Large Dams -2019: Government of India Central Water CommissionPrabhjeet BaidNo ratings yet
- l2 Unit 8 Statement of Aims Blank 2023 Templa 1Document8 pagesl2 Unit 8 Statement of Aims Blank 2023 Templa 1api-631701024No ratings yet
- The Nightingale and The RoseDocument23 pagesThe Nightingale and The RosesaimaNo ratings yet
- SUCCESSION CHAMP Notes (BALANE)Document91 pagesSUCCESSION CHAMP Notes (BALANE)carlee01483% (6)
- Pem735 D00084 D XxenDocument6 pagesPem735 D00084 D XxenYigit SarıkayaNo ratings yet
- Tactical Baptism: Q. Is Major Benson Pain Correct and Justified To Use Waterboarding Against AbuDocument4 pagesTactical Baptism: Q. Is Major Benson Pain Correct and Justified To Use Waterboarding Against AbuLAW10101100% (2)
- Lesson Plan and ProductDocument4 pagesLesson Plan and Productapi-435897192No ratings yet
- Question Bank Topic 1 Economic Thinking and Choice in A World of ScarcityDocument19 pagesQuestion Bank Topic 1 Economic Thinking and Choice in A World of ScarcityHide Yasu NakajimaNo ratings yet
- How To Prepare General Awareness For SSC CGLDocument7 pagesHow To Prepare General Awareness For SSC CGLreshmaNo ratings yet
- Abbott Ruby CasebookDocument91 pagesAbbott Ruby CasebookjtmchughNo ratings yet
- Bundling and Best FitDocument41 pagesBundling and Best FitJeena JnNo ratings yet
- Directions To Candidates Paper 1 - MedicalDocument29 pagesDirections To Candidates Paper 1 - MedicalMedicEdNo ratings yet
- Standardization For Livable Spaces in Historic EnvironmentsDocument10 pagesStandardization For Livable Spaces in Historic EnvironmentsmetamakNo ratings yet
- Corporal Punishment Versus Capital PunishmentDocument8 pagesCorporal Punishment Versus Capital PunishmentWac GunarathnaNo ratings yet
- Mise en place ingredients and equipment listDocument10 pagesMise en place ingredients and equipment listDavis Sagini ArtNo ratings yet
- Rufino Luna, Et - Al V CA, Et - Al (G.R. No. 100374-75)Document3 pagesRufino Luna, Et - Al V CA, Et - Al (G.R. No. 100374-75)Alainah ChuaNo ratings yet
- Wrongful Restraint and Wrongful ConfinementDocument11 pagesWrongful Restraint and Wrongful ConfinementPrabhnoor Guliani100% (1)
- Interzone 5140: Epoxy PrimerDocument4 pagesInterzone 5140: Epoxy PrimerTrịnh Minh KhoaNo ratings yet
- ENGLSIH LISTENING SKILLS (Question Paper) PDFDocument2 pagesENGLSIH LISTENING SKILLS (Question Paper) PDFGagan H RNo ratings yet
- MPEGRepair HDDocument173 pagesMPEGRepair HDMAHTorresNo ratings yet
- Regents Prep 4Document7 pagesRegents Prep 4api-24284785450% (2)
- 50 Hour Foundation Course Complete English Tenses Class 2 1Document79 pages50 Hour Foundation Course Complete English Tenses Class 2 1Riya KushwahNo ratings yet