You might also like
- Running Head: MIAH ZAVARRO V3 Miah Zavarro V3 Name Course Institution DateDocument4 pagesRunning Head: MIAH ZAVARRO V3 Miah Zavarro V3 Name Course Institution DateSammy Chege100% (1)
- Pat Ogden Sensorimotor Therapy PDFDocument16 pagesPat Ogden Sensorimotor Therapy PDFEmili Giralt GuarroNo ratings yet
- ESC-GASTPE School COVID19 Recovery and Readiness Plan S.Y. 2020 - 2021Document5 pagesESC-GASTPE School COVID19 Recovery and Readiness Plan S.Y. 2020 - 2021Jubylyn Aficial100% (3)
- Directions In: PsychiatryDocument44 pagesDirections In: Psychiatrybrad_99100% (2)
- Neurobiology of Post Traumatic Stress Disorder - Newport & NemeroffDocument9 pagesNeurobiology of Post Traumatic Stress Disorder - Newport & NemeroffunonguyNo ratings yet
- PETRONAS Fuel Oil 80: Safety Data SheetDocument10 pagesPETRONAS Fuel Oil 80: Safety Data SheetJaharudin JuhanNo ratings yet
- Postconcussion SyndromeDocument16 pagesPostconcussion SyndromeonaNo ratings yet
- D HC OperatorsDocument5,396 pagesD HC OperatorsCoupon VampireNo ratings yet
- The Body Keeps The ScoreDocument46 pagesThe Body Keeps The ScoreCatalina Ursa50% (4)
- Post Traumatic Stress Disorder The Neurobiological Impact of Psychological TraumaDocument17 pagesPost Traumatic Stress Disorder The Neurobiological Impact of Psychological TraumaMariana VilcaNo ratings yet
- Rta Stress Horowitz 1986Document9 pagesRta Stress Horowitz 1986marielaNo ratings yet
- Andrew Oberle, Neuroscience Informed Approach To TraumaDocument5 pagesAndrew Oberle, Neuroscience Informed Approach To TraumaSilvio danteNo ratings yet
- NIH Public Access: Author ManuscriptDocument43 pagesNIH Public Access: Author ManuscriptL JNo ratings yet
- Peritraumatik Penyebab PTSDDocument7 pagesPeritraumatik Penyebab PTSDistianna nurhidayatiNo ratings yet
- PsychoneuroendocrinologyDocument12 pagesPsychoneuroendocrinologyFahrunnisa NurdinNo ratings yet
- Neurologic Desensitization in The Treatment of Posttraumatic StressDocument16 pagesNeurologic Desensitization in The Treatment of Posttraumatic StressVictor Lopez SueroNo ratings yet
- Structural and Functional Neuroplasticity in Relation To Traumatic StressDocument5 pagesStructural and Functional Neuroplasticity in Relation To Traumatic Stressapi-348971279No ratings yet
- Posttraumatic Stress Disorder After Cerebrovascular EventsDocument2 pagesPosttraumatic Stress Disorder After Cerebrovascular EventsdenisNo ratings yet
- Context Processing and The Neurobiology of Post Traumatic PDFDocument35 pagesContext Processing and The Neurobiology of Post Traumatic PDFUSM San IgnacioNo ratings yet
- Revues - Voluntad 2Document17 pagesRevues - Voluntad 2Victor CarrenoNo ratings yet
- Central Mechanisms of Pathological PainDocument9 pagesCentral Mechanisms of Pathological PainRocio DominguezNo ratings yet
- Contrafactual ThinkingDocument8 pagesContrafactual ThinkingLucasNo ratings yet
- Progress in Neuropsychopharmacology & Biological Psychiatry: Etienne Vachon-PresseauDocument8 pagesProgress in Neuropsychopharmacology & Biological Psychiatry: Etienne Vachon-PresseauFrancisco JavierNo ratings yet
- Post-Traumatic Stress Disorder: In-Depth ReviewDocument5 pagesPost-Traumatic Stress Disorder: In-Depth ReviewStardya RuntuwarowNo ratings yet
- Pathological Grief Diagnosis and ExplanationDocument14 pagesPathological Grief Diagnosis and ExplanationChana FernandesNo ratings yet
- Evaluacion y Tratamiento Psicodinamico en Pacientes TraumatiDocument12 pagesEvaluacion y Tratamiento Psicodinamico en Pacientes TraumatijoNo ratings yet
- Articulo 3Document19 pagesArticulo 3Virginia ManzanoNo ratings yet
- Dissociation Affect Dysregulation Somatization BVDKDocument22 pagesDissociation Affect Dysregulation Somatization BVDKkanuNo ratings yet
- Aupperle 2012 - Executive Function and PTSDDocument9 pagesAupperle 2012 - Executive Function and PTSDElena-Andreea MutNo ratings yet
- Update On The Management of Post-Traumatic Stress Disorder: Volume 38: Number 2: April 2015Document5 pagesUpdate On The Management of Post-Traumatic Stress Disorder: Volume 38: Number 2: April 2015Via Eliadora TogatoropNo ratings yet
- Factorii de Risc În Vulnerabilitatea Durerii CroniceDocument9 pagesFactorii de Risc În Vulnerabilitatea Durerii Cronicecj_catalinaNo ratings yet
- Symptomatology and Psychopathology of Mental Health Problems After DisasterDocument11 pagesSymptomatology and Psychopathology of Mental Health Problems After DisasterFelipe Ignacio Vilugron ConstanzoNo ratings yet
- Post-Traumatic Stress Disorder: In-Depth ReviewDocument5 pagesPost-Traumatic Stress Disorder: In-Depth ReviewnovywardanaNo ratings yet
- D Jeffrey Newport and Charles B Nemeroff : Neurobiology of Posttraumatic Stress DisorderDocument8 pagesD Jeffrey Newport and Charles B Nemeroff : Neurobiology of Posttraumatic Stress DisordermapiNo ratings yet
- Body20keeps20the20score 20kolk20Document22 pagesBody20keeps20the20score 20kolk20lauraspring72No ratings yet
- PTJ 0339Document13 pagesPTJ 0339api-438956780No ratings yet
- Anxiety After Stroke: A Systematic Review and Meta-AnalysisDocument10 pagesAnxiety After Stroke: A Systematic Review and Meta-AnalysisMeilisa KusdiantoNo ratings yet
- Acupuntura AlgoDocument6 pagesAcupuntura AlgoSergio SCNo ratings yet
- The Body Keeps The ScoreDocument22 pagesThe Body Keeps The ScoreLaura Paola Garcia100% (1)
- Psicosis Cicloide y Su Diagnóstico LongitudinalDocument6 pagesPsicosis Cicloide y Su Diagnóstico LongitudinalmarielaNo ratings yet
- Reaction To Severe Stress and Adjustment DisorderDocument22 pagesReaction To Severe Stress and Adjustment DisorderTulika SarkarNo ratings yet
- Quality of Life in Stroke SurvivorsDocument7 pagesQuality of Life in Stroke SurvivorsMiriam NovoNo ratings yet
- NIH Public Access: How The Neurocircuitry and Genetics of Fear Inhibition May Inform Our Understanding of PTSDDocument25 pagesNIH Public Access: How The Neurocircuitry and Genetics of Fear Inhibition May Inform Our Understanding of PTSDmapiNo ratings yet
- ASIADocument9 pagesASIADiana BNo ratings yet
- Mood Disorders Following Traumatic Brain Injury: Ricardo Jorge & Robert G. RobinsonDocument11 pagesMood Disorders Following Traumatic Brain Injury: Ricardo Jorge & Robert G. RobinsonCarolina MuñozNo ratings yet
- DialoguesClinNeurosci 13 366 PDFDocument5 pagesDialoguesClinNeurosci 13 366 PDFAfriza Bin Yuana ArifinNo ratings yet
- Tept Artículo de RevisiónDocument9 pagesTept Artículo de RevisiónVanesa Molina AcurioNo ratings yet
- Nemeroff Heim PTSDDocument12 pagesNemeroff Heim PTSDmariela100% (1)
- Coping With Gulf War Combat Stress: Mediating and Moderating EffectsDocument10 pagesCoping With Gulf War Combat Stress: Mediating and Moderating Effectstatu sorinaNo ratings yet
- Fnins 17 1281401Document16 pagesFnins 17 1281401adinjiaNo ratings yet
- Pittenger 2007Document22 pagesPittenger 2007rocambolescas perthNo ratings yet
- Psychological Therapies For Posttraumatic Stress Disorder PDFDocument5 pagesPsychological Therapies For Posttraumatic Stress Disorder PDFJessicaPudduNo ratings yet
- Diagnosis and Management of Anxiety Disorders: Charles I. Shelton, DODocument4 pagesDiagnosis and Management of Anxiety Disorders: Charles I. Shelton, DODaniar N. HanifahNo ratings yet
- La Psiconeuroinmunología y El TraumaDocument27 pagesLa Psiconeuroinmunología y El TraumaAnonymous Hy99nkiNo ratings yet
- Pyszczynski 2011Document24 pagesPyszczynski 2011cutkilerNo ratings yet
- Npp201088a 2Document20 pagesNpp201088a 2Gia KuteliaNo ratings yet
- Postamatric Stress DisorderDocument1 pagePostamatric Stress DisorderDavid Felipe Gomez AcevedoNo ratings yet
- HHS Public Access: Neurobiology of The Premonitory Urge in Tourette Syndrome: Pathophysiology and Treatment ImplicationsDocument19 pagesHHS Public Access: Neurobiology of The Premonitory Urge in Tourette Syndrome: Pathophysiology and Treatment Implicationsyeremias setyawanNo ratings yet
- A Cognitive Model of Posttraumatic Stress Disorder - Ehlers - Clark - 2000Document27 pagesA Cognitive Model of Posttraumatic Stress Disorder - Ehlers - Clark - 2000Dana Goţia100% (1)
- Caneta MágicaDocument7 pagesCaneta MágicaWeverton MedeirosNo ratings yet
- Stress Brain PlasticityDocument15 pagesStress Brain PlasticityLilian Cerri MazzaNo ratings yet
- Prolonged Psychosocial Effects of Disaster: A Study of Buffalo CreekFrom EverandProlonged Psychosocial Effects of Disaster: A Study of Buffalo CreekRating: 1 out of 5 stars1/5 (1)
- Use of Cannabis in the Treatment of Post-Traumatic Stress DisorderFrom EverandUse of Cannabis in the Treatment of Post-Traumatic Stress DisorderNo ratings yet
- 2005 An Anthropological Hybrid The Pragmatic Arrangement of Universalism andDocument22 pages2005 An Anthropological Hybrid The Pragmatic Arrangement of Universalism andLuana SouzaNo ratings yet
- Fassin SD The Endurance of CritiqueDocument34 pagesFassin SD The Endurance of CritiqueLuana SouzaNo ratings yet
- 2001 The Explanatory Models of Mental Health Amongst Low-Income Women and Health Care Practitioners in LusakaDocument8 pages2001 The Explanatory Models of Mental Health Amongst Low-Income Women and Health Care Practitioners in LusakaLuana SouzaNo ratings yet
- 2001 - Kyol Goeu ('Wind Overload') Part I - A Cultural Syndrome of Orthostatic Panic Among Khmer RefugeesDocument30 pages2001 - Kyol Goeu ('Wind Overload') Part I - A Cultural Syndrome of Orthostatic Panic Among Khmer RefugeesLuana SouzaNo ratings yet
- 2001 - Kyol Goeu ('Wind Overload') Part IIDocument28 pages2001 - Kyol Goeu ('Wind Overload') Part IILuana SouzaNo ratings yet
- 2001) - Trauma and Loss As Determinants of Medically Unexplained Epidemic Illness in A Bhutanese Refugee CampDocument9 pages2001) - Trauma and Loss As Determinants of Medically Unexplained Epidemic Illness in A Bhutanese Refugee CampLuana SouzaNo ratings yet
- Challenging Definitions of Psychological Trauma: Connecting Racial Microaggressions and Traumatic StressDocument15 pagesChallenging Definitions of Psychological Trauma: Connecting Racial Microaggressions and Traumatic StressLuana SouzaNo ratings yet
- 1986 Universal Aspects of Symbolic HealingDocument14 pages1986 Universal Aspects of Symbolic HealingLuana SouzaNo ratings yet
- 2001 Kyol Goeu in CambodiaDocument6 pages2001 Kyol Goeu in CambodiaLuana SouzaNo ratings yet
- 2000 - Globalizing Disaster Trauma - BreslauDocument24 pages2000 - Globalizing Disaster Trauma - BreslauLuana SouzaNo ratings yet
- (Classics of Western Spirituality) Reuven Hammer - The Classic Midrash - Tannaitic Commentaries On The Bible-Paulist Press (1995)Document552 pages(Classics of Western Spirituality) Reuven Hammer - The Classic Midrash - Tannaitic Commentaries On The Bible-Paulist Press (1995)Luana SouzaNo ratings yet
- Artigo Internacional If SHW Is Not A Victime, Dows That Mean She Was Not TraumatizedDocument20 pagesArtigo Internacional If SHW Is Not A Victime, Dows That Mean She Was Not TraumatizedLuana SouzaNo ratings yet
- Jong2013 Collective Trauma ProcessingDocument18 pagesJong2013 Collective Trauma ProcessingLuana SouzaNo ratings yet
- 2018 The Pain I Rise Above - How International Human Rights Can BestDocument33 pages2018 The Pain I Rise Above - How International Human Rights Can BestLuana SouzaNo ratings yet
- Perri Six, Susannah Radstone, Corinne Squire, Amal Treacher (Eds.) - Public Emotions-Palgrave Macmillan UK (2007)Document261 pagesPerri Six, Susannah Radstone, Corinne Squire, Amal Treacher (Eds.) - Public Emotions-Palgrave Macmillan UK (2007)Luana SouzaNo ratings yet
- Cultures of Trauma: Anthropological Views of Posttraumatic Stress Disorder in International HealthDocument15 pagesCultures of Trauma: Anthropological Views of Posttraumatic Stress Disorder in International HealthLuana SouzaNo ratings yet
- 2016 Health Impact of Human Rights Testimony - Harming The Most VulnerableDocument5 pages2016 Health Impact of Human Rights Testimony - Harming The Most VulnerableLuana SouzaNo ratings yet
- 2021 PTSD, Human Rights and Access To HealthcareDocument9 pages2021 PTSD, Human Rights and Access To HealthcareLuana SouzaNo ratings yet
- Artigo Internacional Why Do Rape Survivors Volunteer For Face-To-Face InterviewsDocument11 pagesArtigo Internacional Why Do Rape Survivors Volunteer For Face-To-Face InterviewsLuana SouzaNo ratings yet
- 2018 Trauma, Depression and Burnout in The Human Rights Field - Identifying Barriers and Pathways To Resilient AdvocacyDocument57 pages2018 Trauma, Depression and Burnout in The Human Rights Field - Identifying Barriers and Pathways To Resilient AdvocacyLuana SouzaNo ratings yet
- Artigo Internacional Understanding Rape and Sexual Assault 20 Years of Progress and Future DirectionsDocument5 pagesArtigo Internacional Understanding Rape and Sexual Assault 20 Years of Progress and Future DirectionsLuana SouzaNo ratings yet
- British Prisoners-of-War: From Resilience To Psychological Vulnerability: Reality or PerceptionDocument21 pagesBritish Prisoners-of-War: From Resilience To Psychological Vulnerability: Reality or PerceptionLuana SouzaNo ratings yet
- Irene Visser - Decolonizing Trauma Theory - Retrospect and Prospects - 2015Document16 pagesIrene Visser - Decolonizing Trauma Theory - Retrospect and Prospects - 2015Luana SouzaNo ratings yet
- Example06 Annotations e PDFDocument12 pagesExample06 Annotations e PDFratae20No ratings yet
- QuestionDocument5 pagesQuestionJavy mae masbateNo ratings yet
- Emotional Brain Revisited - (Impulsive Action and Impulse Control)Document24 pagesEmotional Brain Revisited - (Impulsive Action and Impulse Control)LauNo ratings yet
- Chapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamDocument21 pagesChapter 22: The Thyroid Gland: by Marissa Grotzke, Dev AbrahamJanielle FajardoNo ratings yet
- Metil MerkaptanDocument14 pagesMetil MerkaptanEngineer TeknoNo ratings yet
- Titus Lithium Battery: Safety Data SheetDocument5 pagesTitus Lithium Battery: Safety Data SheetKittikun Ap UnitechNo ratings yet
- Activity 3: Worksheet On Developmental Tasks of Being in Grade 11Document2 pagesActivity 3: Worksheet On Developmental Tasks of Being in Grade 11Ian BoneoNo ratings yet
- Peridex (Oral Rinse)Document11 pagesPeridex (Oral Rinse)Emeka NnajiNo ratings yet
- Analysis of The Health Financing Structure of BotswanaDocument5 pagesAnalysis of The Health Financing Structure of BotswanaOlusola Olabisi OgunseyeNo ratings yet
- Sample of mkt202 ProjectDocument16 pagesSample of mkt202 ProjectMohammad Sohan Khan 2121426630No ratings yet
- A Pragmatic View of Thematic AnalysisDocument5 pagesA Pragmatic View of Thematic AnalysisLouis SpencerNo ratings yet
- Health10 q3 Mod1 Healthtrendsissues v5Document27 pagesHealth10 q3 Mod1 Healthtrendsissues v5Wensyl Mae De GuzmanNo ratings yet
- Rinchuse 2006Document10 pagesRinchuse 2006Natalie JaraNo ratings yet
- Print Boarding PassDocument2 pagesPrint Boarding PassAshu SinghNo ratings yet
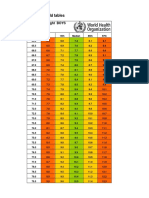
- Boys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Document4 pagesBoys Simplified Field Tables Weight For Length 2 To 5 Years (Percentiles)Gabrielly LopesNo ratings yet
- Citizens Civil Complaint Against Pittsfield, Cell TowerDocument65 pagesCitizens Civil Complaint Against Pittsfield, Cell ToweriBerkshires.comNo ratings yet
- Principles of CGMP in Pharmaceutical IndustriesDocument6 pagesPrinciples of CGMP in Pharmaceutical IndustriesSamer SowidanNo ratings yet
- SKM 4 - COCU - CU5 - Child - Care - Centre - ParentalDocument11 pagesSKM 4 - COCU - CU5 - Child - Care - Centre - ParentalShireen TahirNo ratings yet
- LF105 MSDS报告 2018.2.9Document15 pagesLF105 MSDS报告 2018.2.9penguking_113236970No ratings yet
- EFFECTS OF ALUGBATI (Basella Alba) On The Growth Performance of Mallard DuckDocument7 pagesEFFECTS OF ALUGBATI (Basella Alba) On The Growth Performance of Mallard DuckCyLo PatricioNo ratings yet
- Ravi Kannaiyan: QC Inspection EngineerDocument5 pagesRavi Kannaiyan: QC Inspection EngineerVinoth BalaNo ratings yet
- Sabarimala: Virtual-Q Booking CouponDocument2 pagesSabarimala: Virtual-Q Booking CouponST COMMNICATIONNo ratings yet
- Operating RoomDocument13 pagesOperating RoomrichardNo ratings yet
- EAPPQ4W4CADocument9 pagesEAPPQ4W4CAPhebi ReyNo ratings yet
- Research Paper FinalDocument12 pagesResearch Paper Finalapi-609577576No ratings yet
- Planned Parenthood Maryland 2020Document12 pagesPlanned Parenthood Maryland 2020Kate AndersonNo ratings yet