You might also like
- Pediatric Immunology: A Case-Based Collection with MCQs, Volume 2From EverandPediatric Immunology: A Case-Based Collection with MCQs, Volume 2No ratings yet
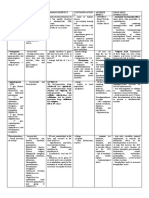
- Drug Index Generic Name MOA Clinical Uses Side Effects/ Contraindications DosageDocument3 pagesDrug Index Generic Name MOA Clinical Uses Side Effects/ Contraindications Dosageyoke limuriaNo ratings yet
- AB in HematooncoDocument39 pagesAB in HematooncokemalahmadNo ratings yet
- Hiper IgD Syndrome (HIDS) Clinical and Genetic Features in Five PatientsDocument1 pageHiper IgD Syndrome (HIDS) Clinical and Genetic Features in Five PatientsDavids MarinNo ratings yet
- Iris More Answers More QSTDocument4 pagesIris More Answers More QSTHoussemSoltanaNo ratings yet
- PENAFIEL M6 April21-2023Document21 pagesPENAFIEL M6 April21-2023Precious Valerie PenafielNo ratings yet
- Drug Study MMRDocument2 pagesDrug Study MMRErika Marie Calucab100% (2)
- 4753-Article Text-31653-2-10-20221130Document10 pages4753-Article Text-31653-2-10-20221130ariniyulfa endrianiNo ratings yet
- Preeclampsia: Pathophysiology, Old and New Strategies For ManagementDocument7 pagesPreeclampsia: Pathophysiology, Old and New Strategies For ManagementAndre GunawanNo ratings yet
- CH 008 Enteric Fever PDFDocument7 pagesCH 008 Enteric Fever PDFVibojaxNo ratings yet
- Successful Treatment of NDM-1 Klebsiella Pneumoniae Bacteraemia in A Neutropenic PatientDocument3 pagesSuccessful Treatment of NDM-1 Klebsiella Pneumoniae Bacteraemia in A Neutropenic PatientSundus ShehzadNo ratings yet
- Acute Bacterial MeningitisDocument10 pagesAcute Bacterial Meningitisjmichel2No ratings yet
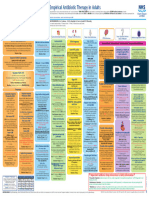
- 2021 Infection Management PosterDocument1 page2021 Infection Management PosterBosco WoodsNo ratings yet
- CIDP - Current Treatments and Identification of Targets For Future Specific Therapeutic Intervention.Document14 pagesCIDP - Current Treatments and Identification of Targets For Future Specific Therapeutic Intervention.zaquvubeNo ratings yet
- Aminoglycosides - Synergistic Bactericidal EffectDocument12 pagesAminoglycosides - Synergistic Bactericidal EffectBern NerquitNo ratings yet
- Antibiotic Prescribing in Primary Care - Therapeutic Guidelines Summary Table 2019Document2 pagesAntibiotic Prescribing in Primary Care - Therapeutic Guidelines Summary Table 2019RL100% (1)
- Cefuroxime (Drug Study)Document2 pagesCefuroxime (Drug Study)Rosebel LaguraNo ratings yet
- Wesleyan: College of Nursing and Allied Medical SciencesDocument2 pagesWesleyan: College of Nursing and Allied Medical SciencesShane Aileen AngelesNo ratings yet
- Guidelines Emporical Antibiotic Therapy in AdultDocument2 pagesGuidelines Emporical Antibiotic Therapy in Adultgulf jobsNo ratings yet
- RUG Tudy: College of NursingDocument3 pagesRUG Tudy: College of NursingYoko Mae YanoNo ratings yet
- Ivermectin Potential Candidate For The Treatment of Covid 19Document3 pagesIvermectin Potential Candidate For The Treatment of Covid 19glenwell sentosaNo ratings yet
- DRUG TABULATION EditedDocument7 pagesDRUG TABULATION EditedAlexa Nicole GayosoNo ratings yet
- Drug Classification/Indicati ON Mechanis MOF Action Contraindication Adverse Reaction Dose, Route, Frequenc Y Nursing Responsibiliti ESDocument5 pagesDrug Classification/Indicati ON Mechanis MOF Action Contraindication Adverse Reaction Dose, Route, Frequenc Y Nursing Responsibiliti ESNicole cuencosNo ratings yet
- Drug StudyDocument2 pagesDrug StudyRenmen Rosito Hortelano100% (3)
- How Do I Manage Nocardiosis?Document9 pagesHow Do I Manage Nocardiosis?Dan JaiNo ratings yet
- Any Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently ReceivingDocument1 pageAny Up-Dates Are To Be Completed in Different Color Ink. The Student Is Expected To Document All Meds The Client Is Currently Receivinggeorgeloto12No ratings yet
- Vaccines 10 00716Document7 pagesVaccines 10 00716Rutvik ShahNo ratings yet
- Transport of Critically Ill Adults 2011Document1 pageTransport of Critically Ill Adults 2011velocity25No ratings yet
- Ofelia L. Mendoza - Drug StudyDocument3 pagesOfelia L. Mendoza - Drug StudyMaenard JavierNo ratings yet
- Hepatitis of Unknown IKRA 2022Document25 pagesHepatitis of Unknown IKRA 2022NHIANo ratings yet
- Drug Study - AmpicillinDocument1 pageDrug Study - AmpicillinsebbyenolaNo ratings yet
- Manajemen PneumoniaeDocument47 pagesManajemen PneumoniaeEfen YtNo ratings yet
- MeningitisDocument4 pagesMeningitisIan CiarNo ratings yet
- Risk For Infection Related To Failure To Avoid Pathogen Secondary To Exposure To COVID-19Document2 pagesRisk For Infection Related To Failure To Avoid Pathogen Secondary To Exposure To COVID-19Yessamin Paith Roderos100% (1)
- CeftriaxoneDocument1 pageCeftriaxonecen janber cabrillosNo ratings yet
- Drug Study 4Document5 pagesDrug Study 4Saito SanNo ratings yet
- Drug Name Therapeutic Actions Indications Adverse Effect Indication Contraindication Nursing ResponsibilitiesDocument5 pagesDrug Name Therapeutic Actions Indications Adverse Effect Indication Contraindication Nursing ResponsibilitiesJoshua Davantes100% (1)
- MainDocument14 pagesMainwiwiNo ratings yet
- College of Nursing: Pharmacological ManagementDocument3 pagesCollege of Nursing: Pharmacological ManagementAnika PleñosNo ratings yet
- Duration of Antifungal Treatment in Mold.4Document7 pagesDuration of Antifungal Treatment in Mold.4Dokter Umum PTTNo ratings yet
- Methylene Blue For The Treatment-BMJ Case Rep-2022Document4 pagesMethylene Blue For The Treatment-BMJ Case Rep-2022Lisandro IglesiasNo ratings yet
- Concept Map For DenvDocument4 pagesConcept Map For Denvnikki sabs67% (3)
- Cardiacand Respiratory CMsDocument23 pagesCardiacand Respiratory CMsday alcoberNo ratings yet
- Penicillin Allergy GuidanceDocument9 pagesPenicillin Allergy Guidancerob burrNo ratings yet
- Corticosteroid Therapy in Combination With Antibiotics For ErysipelasDocument4 pagesCorticosteroid Therapy in Combination With Antibiotics For Erysipelasyubi arsanaNo ratings yet
- DownloadDocument13 pagesDownloadjtd9h2xp5hNo ratings yet
- Assessment Nursing Diagnosis Scientific Explanation Objectives Interventions Rationale Expected OutcomeDocument3 pagesAssessment Nursing Diagnosis Scientific Explanation Objectives Interventions Rationale Expected OutcomeRammiel Saylo CarlosNo ratings yet
- Efficacy and Safety of Oral Administration of A Mixture of Probiotic Strains in Patients With Psoriasis: A Randomized Controlled Clinical TrialDocument7 pagesEfficacy and Safety of Oral Administration of A Mixture of Probiotic Strains in Patients With Psoriasis: A Randomized Controlled Clinical TrialHafid Adi NugrohoNo ratings yet
- Association Between Treatment With Colchicine and Improved Survival in A Single-Centre Cohort of Adult Hospitalised Patients With COVID-19 Pneumonia and Acute Respiratory Distress SyndromeDocument4 pagesAssociation Between Treatment With Colchicine and Improved Survival in A Single-Centre Cohort of Adult Hospitalised Patients With COVID-19 Pneumonia and Acute Respiratory Distress SyndromeEmilioNo ratings yet
- ENDOPHTHALMITISDocument1 pageENDOPHTHALMITISb99401114No ratings yet
- Pengobatan Gabapentin Terhadap Postherpetic Neuralgia (PHN) : November 2019Document7 pagesPengobatan Gabapentin Terhadap Postherpetic Neuralgia (PHN) : November 2019hanananwarNo ratings yet
- Word CmeDocument4 pagesWord CmeJasper VictoriaNo ratings yet
- Microbiology Assignment. ADocument26 pagesMicrobiology Assignment. ACynthia AbbangNo ratings yet
- Internal Medicine Journal - 2018 - Young - Meningitis in Adults Diagnosis and ManagementDocument14 pagesInternal Medicine Journal - 2018 - Young - Meningitis in Adults Diagnosis and Managementfitri dwiyantiNo ratings yet
- Consideration of Severe Coronavirus Disease 2019.12Document5 pagesConsideration of Severe Coronavirus Disease 2019.12yovanNo ratings yet
- DM Topical BacterialDocument10 pagesDM Topical BacterialKowe Bento TenanNo ratings yet
- 4753-Article Text-31653-2-10-20221130Document10 pages4753-Article Text-31653-2-10-20221130ariniyulfa endrianiNo ratings yet
- Drug Study MugnaDocument7 pagesDrug Study Mugnakint manlangitNo ratings yet
- VancomycinDocument1 pageVancomycinJUSTINE ALLYSA MAY CASTILLONo ratings yet
- Ref For Slide (4) Nosocomial InfectionsDocument7 pagesRef For Slide (4) Nosocomial InfectionsAyesha SamnaniNo ratings yet
- Procalcitonin Levels in Surgical Patients at Risk of CandidemiaDocument6 pagesProcalcitonin Levels in Surgical Patients at Risk of CandidemiaKeziaNo ratings yet
- Serum Procalcitonin Levels of Patients With Candidemia Hospitalized in Intensive Care UnitsDocument4 pagesSerum Procalcitonin Levels of Patients With Candidemia Hospitalized in Intensive Care UnitsKeziaNo ratings yet
- The Clinical Outcomes and Predictive Factors For.24Document5 pagesThe Clinical Outcomes and Predictive Factors For.24KeziaNo ratings yet
- Jof 08 00305 v3Document14 pagesJof 08 00305 v3KeziaNo ratings yet
- Structure and Function of Liver and GallbladderDocument21 pagesStructure and Function of Liver and GallbladderKeziaNo ratings yet
- Buccal Mucosa CancerDocument9 pagesBuccal Mucosa Cancermuhammad_ariefNo ratings yet
- State of Health in The EU Cycle, OECD PublishingDocument204 pagesState of Health in The EU Cycle, OECD PublishingJasmin Džaja DurmiševićNo ratings yet
- Vertebral HemangiomaDocument6 pagesVertebral HemangiomanotallowedNo ratings yet
- Matary Appendix Summary01Document4 pagesMatary Appendix Summary01Muhammad GoharNo ratings yet
- Linfedema en Mexico: Un Panorama Clínico y EpidemiologicoDocument11 pagesLinfedema en Mexico: Un Panorama Clínico y EpidemiologicoEnrique LopezNo ratings yet
- Glomerular Diseases: Assistant Professor Dr. Shumaila Rafi MedicineDocument17 pagesGlomerular Diseases: Assistant Professor Dr. Shumaila Rafi MedicineMuhammad MakkiNo ratings yet
- LMNH Manta F BlastoidaDocument3 pagesLMNH Manta F BlastoidaAlinaNo ratings yet
- Invasive Cervical Cancer - Epidemiology, Risk Factors, Clinical Manifestations, and Diagnosis PDFDocument16 pagesInvasive Cervical Cancer - Epidemiology, Risk Factors, Clinical Manifestations, and Diagnosis PDFUzair TariqNo ratings yet
- Brenner and Rector's The Kidney, 2-Volume Set, 10th Edition: Skorecki, Chertow, Marsden, Taal & YuDocument4 pagesBrenner and Rector's The Kidney, 2-Volume Set, 10th Edition: Skorecki, Chertow, Marsden, Taal & YuJim Dominguez RosalesNo ratings yet
- Beyond N-Cadherin Casal y Bartolomé 2019Document20 pagesBeyond N-Cadherin Casal y Bartolomé 2019Ricardo Leon PosadaNo ratings yet
- Nurse Labs Practice Test 12 PDFDocument5 pagesNurse Labs Practice Test 12 PDFNatalie Pemberton-ParrisNo ratings yet
- Asesmen GinekologiDocument15 pagesAsesmen GinekologiYumeko AiharaNo ratings yet
- STDs and Pregnancy Fact SheetDocument2 pagesSTDs and Pregnancy Fact SheetRebecca RichardsonNo ratings yet
- PansitopeniaDocument33 pagesPansitopeniaBrad WrightNo ratings yet
- AEC S301 SyllabusDocument6 pagesAEC S301 SyllabusringobingogoNo ratings yet
- Ca72 4Document2 pagesCa72 4wongso100% (1)
- Liver Function TestDocument20 pagesLiver Function TestkuzhandaiveluNo ratings yet
- Cystosarcoma PhyllodesDocument3 pagesCystosarcoma PhyllodesrahadianharyantoNo ratings yet
- Hodgkin's LymphomaDocument14 pagesHodgkin's LymphomaBeulah AlexNo ratings yet
- Unesco - Eolss Sample Chapter: Plants As A Source of Anti-Cancer AgentsDocument15 pagesUnesco - Eolss Sample Chapter: Plants As A Source of Anti-Cancer AgentsSundararajan Jeyaraman100% (1)
- Cancer CellDocument146 pagesCancer CellmanbastiNo ratings yet
- German Shepherd Dog CharacteristicsDocument10 pagesGerman Shepherd Dog CharacteristicsJoseph Vijay100% (2)
- Oregano: Food ScienceDocument10 pagesOregano: Food ScienceMariavictoria TuboroNo ratings yet
- PneumoniaDocument102 pagesPneumoniaJay Kumar100% (1)
- Overcoming Bladder Disease PDFDocument214 pagesOvercoming Bladder Disease PDFdr. omarNo ratings yet
- Cold Agglutinin DiseaseDocument8 pagesCold Agglutinin Diseasehtunnm@gmail.comNo ratings yet
- National Guidelines For The Management of Sexually Transmitted Infections-Oa6yxme8Document84 pagesNational Guidelines For The Management of Sexually Transmitted Infections-Oa6yxme8HabtamNo ratings yet
- Bio Energetic TherapyDocument19 pagesBio Energetic TherapyVishnu Moorthy Raja Singam100% (2)
- Analytical StudiesDocument23 pagesAnalytical StudiesnavneetbadeshaNo ratings yet
- Clinical Trials and BiostatisticsDocument16 pagesClinical Trials and BiostatisticsArumugam RamasamyNo ratings yet