You might also like
- Sample Job AnalysisDocument3 pagesSample Job AnalysisAbdi Rahman Farah WarsameNo ratings yet
- Caw 3-1Document2 pagesCaw 3-1api-507981264No ratings yet
- Work-Related Version of The BAT: InstructionDocument4 pagesWork-Related Version of The BAT: InstructionYesenia condor toscanoNo ratings yet
- Pelvic Floor Impact QuestionnaireDocument1 pagePelvic Floor Impact Questionnairemaria_daniNo ratings yet
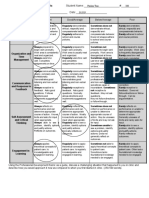
- Approaches To Learning Rubric & Goals (2020)Document2 pagesApproaches To Learning Rubric & Goals (2020)Juanita McGarrigleNo ratings yet
- E Pds Questionnaire April 2013Document1 pageE Pds Questionnaire April 2013antivenomNo ratings yet
- Caw 3-1Document2 pagesCaw 3-1api-490406210No ratings yet
- Self-Assessment in Work EthicsDocument1 pageSelf-Assessment in Work EthicsMark Anthony UmaliNo ratings yet
- Research QuestionnaireDocument2 pagesResearch QuestionnaireRaquel C. VillarinNo ratings yet
- AAAWM Community Survey 2019Document5 pagesAAAWM Community Survey 2019macoyo ormilloNo ratings yet
- Pelvic Floor Impact Questionnaire (PFIQ-7)Document2 pagesPelvic Floor Impact Questionnaire (PFIQ-7)Dharitri PurohitNo ratings yet
- Individual Work Preferences Assessment (IWPA) Long VersionDocument8 pagesIndividual Work Preferences Assessment (IWPA) Long VersionAzela GladyNo ratings yet
- RBQ 3 OTHER v1.3Document4 pagesRBQ 3 OTHER v1.3chv9xcvjvzNo ratings yet
- Mental Health Plan Assessment Form: Relationship PhoneDocument6 pagesMental Health Plan Assessment Form: Relationship Phonealotfya100% (1)
- SCCPSS+SELCompetencies ElementaryDocument4 pagesSCCPSS+SELCompetencies Elementarysavannahnow.comNo ratings yet
- Annual Medicare Wellness Visit Health Risk Assessment: Physical Activity Tobacco UseDocument3 pagesAnnual Medicare Wellness Visit Health Risk Assessment: Physical Activity Tobacco UseShobhitNo ratings yet
- Adhd QuestDocument1 pageAdhd QuestLive8shrinkNo ratings yet
- Clearing My Way Into Ca InterDocument4 pagesClearing My Way Into Ca InterchocNo ratings yet
- Job Holder Name: Status: Job Title: Reports ToDocument3 pagesJob Holder Name: Status: Job Title: Reports ToAhmad FarooqNo ratings yet
- Perceived Deficits QuestionnaireDocument1 pagePerceived Deficits Questionnairemahashweta bhattacharyaNo ratings yet
- Domains Check The Box That Applies To You. Answer The Following QuestionsDocument2 pagesDomains Check The Box That Applies To You. Answer The Following QuestionseulaNo ratings yet
- Subordinate T3v1 27jan23Document3 pagesSubordinate T3v1 27jan23mohammad zubairNo ratings yet
- Copsoq II Medium Size Questionnaire EnglishDocument11 pagesCopsoq II Medium Size Questionnaire EnglishL_AverbookNo ratings yet
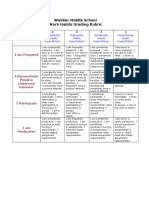
- 2018 ARSU K-5 Habits of Work Scoring CriteriaDocument2 pages2018 ARSU K-5 Habits of Work Scoring CriteriaDEHNo ratings yet
- 5 - Copsoq II Medium Size Questionnaire English PDFDocument11 pages5 - Copsoq II Medium Size Questionnaire English PDFOthan CatorzaNo ratings yet
- HEALTH AND WELL-BEING QUESTIONNAIRE - SF36 - EnglDocument4 pagesHEALTH AND WELL-BEING QUESTIONNAIRE - SF36 - EnglzineeddineboukadoumNo ratings yet
- Clase Nº7Document23 pagesClase Nº7Nadia CarriNo ratings yet
- Character Reference: This Person Is Applying To Be Au Pair AbroadDocument6 pagesCharacter Reference: This Person Is Applying To Be Au Pair AbroadAstina SelenaNo ratings yet
- Do'a Sebelum BelajarDocument24 pagesDo'a Sebelum BelajarRizkiPratamaNo ratings yet
- SCRIPT WST Q 5.3.1manualDocument9 pagesSCRIPT WST Q 5.3.1manualAliren Alejandra FloresNo ratings yet
- FullChecklistRev10 22Document10 pagesFullChecklistRev10 22Vishmitha NNo ratings yet
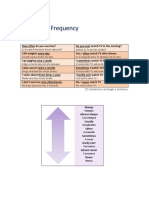
- Freq. Adverbs - Questions With HowDocument2 pagesFreq. Adverbs - Questions With HowAnalia Solange HidalgoNo ratings yet
- Daily Checklist: Did You... Mo N Tu e We D TH U FR I Sa T Su NDocument4 pagesDaily Checklist: Did You... Mo N Tu e We D TH U FR I Sa T Su NRae Dominick Aquino SalvaNo ratings yet
- Avance de Módulo 1Document29 pagesAvance de Módulo 1Claudia GuillenNo ratings yet
- Caw 3-1Document2 pagesCaw 3-1api-508302201No ratings yet
- How The 2190 Rule Helps You Build Good Habits and A Better Life - CapeSpaceDocument1 pageHow The 2190 Rule Helps You Build Good Habits and A Better Life - CapeSpaceYash KamathiNo ratings yet
- The Slight EdgeDocument6 pagesThe Slight EdgeddebusNo ratings yet
- Ili - BDSDocument3 pagesIli - BDSClarence ChunNo ratings yet
- PDR 2020Document1 pagePDR 2020api-506024957No ratings yet
- GIDYQ-AA (Female Adult Version)Document2 pagesGIDYQ-AA (Female Adult Version)jadeNo ratings yet
- Baseline Functional Assessment Tool - Draft - 6Document2 pagesBaseline Functional Assessment Tool - Draft - 6M.DalaniNo ratings yet
- Go-Cademics Presentation by Josephine AghedoDocument19 pagesGo-Cademics Presentation by Josephine AghedoJosephine AghedoNo ratings yet
- Adverbs of Frequency Life and LeisureDocument7 pagesAdverbs of Frequency Life and LeisureWilson Andrés Castro RiascosNo ratings yet
- Highest Priority? Asking For Extensions?Document2 pagesHighest Priority? Asking For Extensions?vishal9patel-63No ratings yet
- WorkDocument1 pageWorkapi-421878308No ratings yet
- Adhd Questionnaire ASRS111 1Document1 pageAdhd Questionnaire ASRS111 1fvktyzvxzbNo ratings yet
- ADHD ChecklistDocument1 pageADHD Checklistbob cretNo ratings yet
- Business and Research Methods 123Document6 pagesBusiness and Research Methods 123Wazeeer AhmadNo ratings yet
- G56 - U5 - Speaking Activity - How Often Do You Do House CoresDocument9 pagesG56 - U5 - Speaking Activity - How Often Do You Do House CoresMirian CorralesNo ratings yet
- How Do I Feel About MyselfDocument2 pagesHow Do I Feel About MyselfJustlene AbdonNo ratings yet
- Individual Work Preferences Assessment+ (IWPA) Short VersionDocument4 pagesIndividual Work Preferences Assessment+ (IWPA) Short VersionAzela GladyNo ratings yet
- Assessment ToolDocument42 pagesAssessment ToolDonbosco RajkumarNo ratings yet
- Slcs/Semester Grade ReflectionsDocument2 pagesSlcs/Semester Grade Reflectionsapi-312434691No ratings yet
- Effectiveness of HRD Programs QuestionnaireDocument6 pagesEffectiveness of HRD Programs QuestionnairePradeeba Ganesh KumarNo ratings yet
- Learning Loop: The Medicine BagDocument8 pagesLearning Loop: The Medicine BagCarlos Jose Guerra MeardiNo ratings yet
- Summary For The Touglen Aív Mérnish Wut - ShártanakDocument9 pagesSummary For The Touglen Aív Mérnish Wut - ShártanaktomivinocurNo ratings yet
- 09 B Your Eating Habits PDFDocument1 page09 B Your Eating Habits PDFGhionna KelleyNo ratings yet
- Work-Related Version of The BAT: InstructionDocument4 pagesWork-Related Version of The BAT: InstructionRichard Oswaldo Valenzuela MendietaNo ratings yet
- Picture of Stomatitis, Glossitis, Cheilosis, Petechiae (Javier, BSN - 2B)Document2 pagesPicture of Stomatitis, Glossitis, Cheilosis, Petechiae (Javier, BSN - 2B)Jan Vier B. JavierNo ratings yet
- English Nursing Workshop Second TermDocument4 pagesEnglish Nursing Workshop Second TermJaneth CallejasNo ratings yet
- Guadalupe Sabio - ENDocument2 pagesGuadalupe Sabio - ENIlaria iudiceNo ratings yet
- COVID-19 Vaccine Information SheetDocument11 pagesCOVID-19 Vaccine Information SheetKirbyCronoNo ratings yet
- Mycotic InfectionDocument22 pagesMycotic InfectionDevanshi Kulkarni100% (1)
- 9 Clinical IndicatorDocument7 pages9 Clinical IndicatorJatoveda HaldarNo ratings yet
- Daftar Diagnosis Penyakit Dengan Gejala AfpDocument1 pageDaftar Diagnosis Penyakit Dengan Gejala Afpnurlaila asmaraniNo ratings yet
- Effects of High Dose Vitamin C Supplementation On Severe Covid19 Patients in The ICU - A Retrospective AnalysisDocument1 pageEffects of High Dose Vitamin C Supplementation On Severe Covid19 Patients in The ICU - A Retrospective AnalysiszipzoinkNo ratings yet
- NSTP AssignmentDocument9 pagesNSTP AssignmentDiana Ruth ElizagaNo ratings yet
- Incidence of Malaria Among Children Under Five YearsDocument43 pagesIncidence of Malaria Among Children Under Five YearsUsman Ahmad TijjaniNo ratings yet
- Learning Activity Sheets Biotechnology 8 (Q4-Lesson 1 & 2) Application of Biotechnology in HealthDocument12 pagesLearning Activity Sheets Biotechnology 8 (Q4-Lesson 1 & 2) Application of Biotechnology in Healthms. dlcrzNo ratings yet
- Inflammatory Bowel Disease (IBD)Document41 pagesInflammatory Bowel Disease (IBD)ririNo ratings yet
- 2nd Unit 2 ALL SESSIONSDocument11 pages2nd Unit 2 ALL SESSIONSOtakanime FRNo ratings yet
- Jytvol 1 2 Contents SynopsisDocument48 pagesJytvol 1 2 Contents SynopsisMohammedNo ratings yet
- 10 Penyakit Terbanyak Rajal Rsud Dr. Iskak 2018Document22 pages10 Penyakit Terbanyak Rajal Rsud Dr. Iskak 2018Anie IstiyaniNo ratings yet
- HSB Sba FFFFFDocument17 pagesHSB Sba FFFFFshelly0% (1)
- ID For ABIM - Parham 2014Document140 pagesID For ABIM - Parham 2014Jeronim H'gharNo ratings yet
- VPE 321veterinary Epidemiology and ZoonosisDocument240 pagesVPE 321veterinary Epidemiology and ZoonosisshivaNo ratings yet
- BabesiaDocument38 pagesBabesiaturinawe haggaiNo ratings yet
- Volume3 Issue4 Jul Aug No.329 665 667Document3 pagesVolume3 Issue4 Jul Aug No.329 665 667MadeKurniawanAsNo ratings yet
- CMS FM Form 1Document9 pagesCMS FM Form 1Ali HamzaNo ratings yet
- HVHJDocument7 pagesHVHJUser NameNo ratings yet
- تقرير اشعه اسنانDocument10 pagesتقرير اشعه اسنانSaif HashimNo ratings yet
- Case KohortDocument37 pagesCase KohortNasir AhmadNo ratings yet
- ImmunizationDocument1 pageImmunizationMicah Lou CalambaNo ratings yet
- Consolidated Physical Fitness Test Form SY: 2018 - 2019 Part I: Health Related Fitness TestDocument4 pagesConsolidated Physical Fitness Test Form SY: 2018 - 2019 Part I: Health Related Fitness TestAlbert MarzanNo ratings yet
- Practice Guidelines For Family Physicians 4 Infection by MansdocsDocument92 pagesPractice Guidelines For Family Physicians 4 Infection by MansdocsDrTarek Mahmoud Abo KammerNo ratings yet
- Bacterial Meningitis and Meningococcal Septicaemia: Implementing NICE GuidanceDocument18 pagesBacterial Meningitis and Meningococcal Septicaemia: Implementing NICE GuidanceZarwo Black UstadzNo ratings yet
- Health Facts Covid 19 Fast Facts About CovidDocument2 pagesHealth Facts Covid 19 Fast Facts About Covidanastacia arceNo ratings yet
- Thyroid CrisisDocument11 pagesThyroid CrisisKoka KolaNo ratings yet