You might also like
- Medicaid Services Manual CompleteDocument1,971 pagesMedicaid Services Manual CompleteTDOGGIENo ratings yet
- Class Action LawsuitDocument78 pagesClass Action LawsuitLindsey BasyeNo ratings yet
- 2020 Health Mart Atlas Currently Contracted PBM Listing PDFDocument5 pages2020 Health Mart Atlas Currently Contracted PBM Listing PDFRao Arslan RajputNo ratings yet
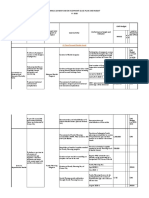
- GAD Accomplishment Report 4th QDocument14 pagesGAD Accomplishment Report 4th QCristine Viernes Gaspar Batay-anNo ratings yet
- OTAG AFP 2021-GAD-Budget-Report-June-2022 PDFDocument35 pagesOTAG AFP 2021-GAD-Budget-Report-June-2022 PDFHaider De LeonNo ratings yet
- 2023 AopDocument48 pages2023 Aopilog ndp100% (1)
- Afghanistan: Current Health Expenditure by Revenue SourcesDocument2 pagesAfghanistan: Current Health Expenditure by Revenue SourcesquintqasNo ratings yet
- 2021 PnhaDocument1 page2021 Pnhakiteli mendozaNo ratings yet
- Medicines Profile Ban EngDocument4 pagesMedicines Profile Ban EngMd K IslamNo ratings yet
- Afghanistan: Health Expenditure ProfileDocument2 pagesAfghanistan: Health Expenditure ProfileJoannaNo ratings yet
- 7 Dr. Dineros - PhilHealth CHO MHODocument15 pages7 Dr. Dineros - PhilHealth CHO MHOKristel Joy Verzon-BunaganNo ratings yet
- In 2018, Total Health Expenditure Contributed 4.6% To GDP.: Health Capital Formation Expenditure, Share and Growth RatesDocument1 pageIn 2018, Total Health Expenditure Contributed 4.6% To GDP.: Health Capital Formation Expenditure, Share and Growth RatesDean Mark AnacioNo ratings yet
- FINAL - Budget BriefDocument6 pagesFINAL - Budget BriefArin DNo ratings yet
- Data TablesDocument78 pagesData Tablesdale naughtonNo ratings yet
- Drug Names PharmacologyDocument40 pagesDrug Names PharmacologyjessssNo ratings yet
- National Health Mission (NHM) : Kavita Singh, Director - FinanceDocument64 pagesNational Health Mission (NHM) : Kavita Singh, Director - FinanceOWAIS ZAHOOR BHATNo ratings yet
- NPA - VAWC Budget Analysis BriefDocument4 pagesNPA - VAWC Budget Analysis BriefGeofrey BennyNo ratings yet
- Operating Budget of Healthcare OrganizationDocument15 pagesOperating Budget of Healthcare OrganizationAchacha Jr El PatronNo ratings yet
- Workshop - Sample Annual GPB For LGUs (PCM Level) 2022Document3 pagesWorkshop - Sample Annual GPB For LGUs (PCM Level) 2022CDS Cavite DILGNo ratings yet
- (SLIDES) Contracting PCWHSDocument16 pages(SLIDES) Contracting PCWHSWilNo ratings yet
- GlobalFund HealthFinancingPolicyBrief Ethiopia Palladium FinalMar2019 - 2Document36 pagesGlobalFund HealthFinancingPolicyBrief Ethiopia Palladium FinalMar2019 - 2Estalew YalewNo ratings yet
- Money Report House HHS Subcommittee Report - 05!14!2015Document20 pagesMoney Report House HHS Subcommittee Report - 05!14!2015CarolinaMercuryNo ratings yet
- Annual Gender and Development (Gad) Plan and Budget FY 2020 Region: VII Province: LeyteDocument6 pagesAnnual Gender and Development (Gad) Plan and Budget FY 2020 Region: VII Province: LeytePatricio Perez Cabahug100% (1)
- PRESENTATION: Financial Sustainability of Reforms by Hiddo HuitzingDocument11 pagesPRESENTATION: Financial Sustainability of Reforms by Hiddo HuitzingADB Health Sector GroupNo ratings yet
- Healthcare Delivery in India-CRISIL-Report-January-8-2022Document52 pagesHealthcare Delivery in India-CRISIL-Report-January-8-2022adikabraNo ratings yet
- Health Financing 1Document65 pagesHealth Financing 1Ruth Mary PadaNo ratings yet
- Healthcare Infographic March 2020 - USDocument1 pageHealthcare Infographic March 2020 - USTheDazzler420No ratings yet
- Leyte (Cities)Document6 pagesLeyte (Cities)Jillian LiganNo ratings yet
- 3) Financial and Operational Performance Analysis 2018-2021Document33 pages3) Financial and Operational Performance Analysis 2018-2021Tomas LeonardelliNo ratings yet
- Health Care Financing Under NHM: 13 Common Review MissionDocument29 pagesHealth Care Financing Under NHM: 13 Common Review MissionnareshNo ratings yet
- 18653-19126 PhilippinesOOPDocument8 pages18653-19126 PhilippinesOOPkasjdkasNo ratings yet
- Pharmaceuticals Industry of Bangladesh PDFDocument24 pagesPharmaceuticals Industry of Bangladesh PDFKazi Rashedul HasanNo ratings yet
- Jdep Strategic Update Meeting 310321 PresentationDocument47 pagesJdep Strategic Update Meeting 310321 PresentationWendy TaborNo ratings yet
- Mar 5 2021 - NASBODocument31 pagesMar 5 2021 - NASBONational Press FoundationNo ratings yet
- Adjusted Results Framework 2022Document6 pagesAdjusted Results Framework 2022Karl Mico AlanguiNo ratings yet
- TMV Template - 2021806Document1 pageTMV Template - 2021806acasushi ginzagaNo ratings yet
- 2018 Sin Tax Incremental Revenue ReportDocument16 pages2018 Sin Tax Incremental Revenue ReportHealth Planning Unit CHD-MMNo ratings yet
- CRS Report RL30731, AIDS Funding For Federal Government Programs - FY1981-FY2003, by Judith A. JohnsonDocument20 pagesCRS Report RL30731, AIDS Funding For Federal Government Programs - FY1981-FY2003, by Judith A. JohnsonConor GuiserNo ratings yet
- Growth Opportunities Abound in Hong Kong's Insurance MarketDocument6 pagesGrowth Opportunities Abound in Hong Kong's Insurance Marketlinru xieNo ratings yet
- PSHD Budget Brief 2016-17Document10 pagesPSHD Budget Brief 2016-17muhammad farhanNo ratings yet
- Cavite 2021Document2 pagesCavite 2021Camae Echin CelisNo ratings yet
- National Health Insurance Fund Nhif Note VfdocxDocument7 pagesNational Health Insurance Fund Nhif Note Vfdocxgeophrey kajokiNo ratings yet
- Gad 2019 Accomplishment Report 2020Document7 pagesGad 2019 Accomplishment Report 2020Gladys EscanoNo ratings yet
- India Macro HealthcareDocument5 pagesIndia Macro HealthcareVansh AggarwalNo ratings yet
- NHA-Policy-Brief Uganda 2016-2019 FINALDocument4 pagesNHA-Policy-Brief Uganda 2016-2019 FINALGodwinNo ratings yet
- One Assure Investment Final DeckDocument21 pagesOne Assure Investment Final DeckSaharshNo ratings yet
- Insights Universal Healthcare Boon For Hospitals PDFDocument34 pagesInsights Universal Healthcare Boon For Hospitals PDFLukman Al-HafizNo ratings yet
- The Philippine Economy: Prospects and Outlook For 2015-2016Document13 pagesThe Philippine Economy: Prospects and Outlook For 2015-2016ristNo ratings yet
- PH UHC Law Series Health Financing Final UpdatedDocument15 pagesPH UHC Law Series Health Financing Final UpdatedArlo Winston De GuzmanNo ratings yet
- Wednesday HoaglandDocument29 pagesWednesday HoaglandNational Press FoundationNo ratings yet
- Webinar GHER 2023 Launch - PresentationDocument14 pagesWebinar GHER 2023 Launch - PresentationAbu WidaadNo ratings yet
- The California Budget: The Top Ten Budget Myths... and The TruthDocument34 pagesThe California Budget: The Top Ten Budget Myths... and The TruthceruleandazeNo ratings yet
- DOF DBCC Presentation FY 2022Document31 pagesDOF DBCC Presentation FY 2022Regine May AbarquezNo ratings yet
- Medicaid Upper Payment Limit Policies: Overcoming A Barrier To ManagedDocument23 pagesMedicaid Upper Payment Limit Policies: Overcoming A Barrier To ManagediGrasshopperNo ratings yet
- Q2 BlashDocument2 pagesQ2 Blashchetan singhNo ratings yet
- Global Pharmaceutical Market Revenue (Billion $) : India's Import and Export 2015-19 TrendDocument2 pagesGlobal Pharmaceutical Market Revenue (Billion $) : India's Import and Export 2015-19 Trendchetan singhNo ratings yet
- Bangladesh: Country SnapshotDocument56 pagesBangladesh: Country SnapshotFaim HasanNo ratings yet
- The Trump White House Policy Wish ListDocument6 pagesThe Trump White House Policy Wish ListCrooked100% (6)
- Updated Equity Valuation Report On Square Pharmaceuticlas LimtiedDocument14 pagesUpdated Equity Valuation Report On Square Pharmaceuticlas LimtiedmaybelNo ratings yet
- Q3 2017 PFE Earnings ReleaseDocument38 pagesQ3 2017 PFE Earnings ReleaseSérgioNo ratings yet
- EHealth in IndiaDocument28 pagesEHealth in IndiasunnyNo ratings yet
- Gender and Development 2020Document8 pagesGender and Development 2020ANN-ANN S. SABANGNo ratings yet
- An Actuarial Model for Costing Universal Health Coverage in ArmeniaFrom EverandAn Actuarial Model for Costing Universal Health Coverage in ArmeniaNo ratings yet
- DI - CHS Consumer SurveyDocument16 pagesDI - CHS Consumer SurveyCNo ratings yet
- Edtech in Southeast Asia White Paper - Executive SummaryDocument7 pagesEdtech in Southeast Asia White Paper - Executive SummaryCNo ratings yet
- Poverty Incidences Region XIIDocument6 pagesPoverty Incidences Region XIICNo ratings yet
- Robert Walters Salary Survey 2021 (Banking)Document7 pagesRobert Walters Salary Survey 2021 (Banking)CNo ratings yet
- Should Universal Healthcare Be Free To All Americans?Document7 pagesShould Universal Healthcare Be Free To All Americans?movys musicNo ratings yet
- Internship Project PresentationDocument20 pagesInternship Project PresentationPRITAM DUTTANo ratings yet
- Welcome Letter - 0320 - MEDocument2 pagesWelcome Letter - 0320 - MELimitless PritamNo ratings yet
- NHS FPX 6008 Assessment 3 Business Case For ChangeDocument6 pagesNHS FPX 6008 Assessment 3 Business Case For Changefarwaamjad771No ratings yet
- Welcome To Hollandzorg!: All Documents in My Hollandzorg'Document2 pagesWelcome To Hollandzorg!: All Documents in My Hollandzorg'Sunand SharmaNo ratings yet
- Fortune Medicare Inc. v. AmorinDocument2 pagesFortune Medicare Inc. v. AmorinRoyet MaligroNo ratings yet
- Star Health Comprehensive Insurance PolicyDocument2 pagesStar Health Comprehensive Insurance PolicyNags KNo ratings yet
- BRILINTA CAD $5 No FTO PDFDocument1 pageBRILINTA CAD $5 No FTO PDFperaNo ratings yet
- Topic 3 Chapter 10 Analysis of Insurance ContractsDocument29 pagesTopic 3 Chapter 10 Analysis of Insurance ContractsYu WenNo ratings yet
- Medical Insurance Guide - QLM - 2021Document12 pagesMedical Insurance Guide - QLM - 2021Murthy VvnNo ratings yet
- Chapter 10 Employee BenefitsDocument21 pagesChapter 10 Employee BenefitsSophie CheungNo ratings yet
- Adv2022-0035 Guidelines On Accreditation Renewal For CY 2023Document1 pageAdv2022-0035 Guidelines On Accreditation Renewal For CY 2023Renso De LeonNo ratings yet
- Family Care Giving Guide AARPD20374Document7 pagesFamily Care Giving Guide AARPD20374Ardal Powell MA PhD CLTC FSCPNo ratings yet
- Health and Disability InsuranceDocument24 pagesHealth and Disability InsurancePrasanna ThalaNo ratings yet
- Max Bupa Reimb Claim Form (1604v1)Document4 pagesMax Bupa Reimb Claim Form (1604v1)Arun Kumar PNo ratings yet
- Sicko Documentary AnalysisDocument3 pagesSicko Documentary AnalysisShahroze JavaidNo ratings yet
- Health Benefits Coverage of Children Until Age 31 Under Chapter 375Document2 pagesHealth Benefits Coverage of Children Until Age 31 Under Chapter 375MarloNo ratings yet
- 2020-Observership ApplicationDocument10 pages2020-Observership ApplicationShirley RamirezNo ratings yet
- The UB-04 Claim Form and NPIDocument4 pagesThe UB-04 Claim Form and NPIKhoerul AnwarNo ratings yet
- Penetration For Insurance Products Increase Post Covid-19 EraDocument17 pagesPenetration For Insurance Products Increase Post Covid-19 EraSiddhesh jadhavNo ratings yet
- Australia - 17-18Document41 pagesAustralia - 17-18Oyash SahuNo ratings yet
- Health Systems Charateristics LAC. FinancialDocument142 pagesHealth Systems Charateristics LAC. FinancialMaria Belen Coca MogroNo ratings yet
- NHS FPX 6008 Assessment 4 Lobbying For ChangeDocument6 pagesNHS FPX 6008 Assessment 4 Lobbying For Changezadem5266No ratings yet
- Module 7 Health Insurance Types and ImportanceDocument10 pagesModule 7 Health Insurance Types and ImportanceKAH' CHISMISSNo ratings yet
- 22-23 Employee Insurance Guide Liberty Assistance - Cat 1 (B)Document32 pages22-23 Employee Insurance Guide Liberty Assistance - Cat 1 (B)Nelson RichardNo ratings yet
- Introduction To Health EconomicsDocument44 pagesIntroduction To Health EconomicsShuaynat PirbudagovaNo ratings yet
- Schedule KDocument2 pagesSchedule Kapi-457375876No ratings yet