You might also like
- Doh - Philippine Health Facility Development Plan 2020 - 2040Document115 pagesDoh - Philippine Health Facility Development Plan 2020 - 2040Adrian Doctolero91% (11)
- LEGASPI - Pestel AnalysisDocument3 pagesLEGASPI - Pestel AnalysisErika Mae Legaspi100% (2)
- Business Models in Telemedicine PDFDocument40 pagesBusiness Models in Telemedicine PDFantoci_steliana100% (1)
- New Tax Return Transcript 2222Document7 pagesNew Tax Return Transcript 2222James Franklin67% (3)
- Entrepreneurial Nursing: What Are The Skills and Opportunities For Addressing Health Related ConcernsDocument8 pagesEntrepreneurial Nursing: What Are The Skills and Opportunities For Addressing Health Related ConcernsTeanu Jose Gabrillo TamayoNo ratings yet
- Entrepre NurseDocument14 pagesEntrepre NurseWendy EscalanteNo ratings yet
- Effects of 2022Document10 pagesEffects of 2022EstreLLA ValenciaNo ratings yet
- 01 The PH Health Care Delivery SystemDocument15 pages01 The PH Health Care Delivery SystemSebastianNo ratings yet
- Philippine EconomyDocument18 pagesPhilippine EconomyninaNo ratings yet
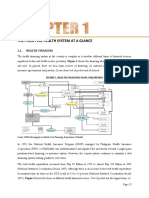
- The Philippine Health System at A GlanceDocument15 pagesThe Philippine Health System at A GlancekrissyNo ratings yet
- Healthcare and TechnologyDocument16 pagesHealthcare and TechnologyAlan MudaryNo ratings yet
- De La Salle University Ramon V. Del Rosario College of BusinessDocument9 pagesDe La Salle University Ramon V. Del Rosario College of BusinessNicole DizonNo ratings yet
- PH UHC Law Series Health Financing Final UpdatedDocument15 pagesPH UHC Law Series Health Financing Final UpdatedArlo Winston De GuzmanNo ratings yet
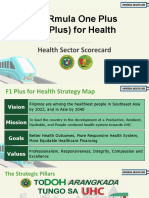
- Fourmula One Plus (F1 Plus) For HealthDocument24 pagesFourmula One Plus (F1 Plus) For Healthchristelm_1No ratings yet
- The Anatomy of The Philippine Health Care SystemDocument43 pagesThe Anatomy of The Philippine Health Care SystemMark Reynie Renz Silva100% (1)
- s12904 021 00847 7Document9 pagess12904 021 00847 7charmyshkuNo ratings yet
- PH UHC Law Series Brief 1Document6 pagesPH UHC Law Series Brief 1Mikko WongNo ratings yet
- Growth Opportunities Abound in Hong Kong's Insurance MarketDocument6 pagesGrowth Opportunities Abound in Hong Kong's Insurance Marketlinru xieNo ratings yet
- Financing Options in Health Care 1Document13 pagesFinancing Options in Health Care 1Saurabh SumanNo ratings yet
- Financing Options in Health Care 1Document13 pagesFinancing Options in Health Care 1Saurabh SumanNo ratings yet
- Ingles 2023-Gastos CatastroficosDocument10 pagesIngles 2023-Gastos CatastroficosEstreLLA ValenciaNo ratings yet
- How Much Household Healthcare Expenditure PDFDocument16 pagesHow Much Household Healthcare Expenditure PDFluis.suarez8899No ratings yet
- Chapter SixDocument11 pagesChapter SixRANDY BAOGBOGNo ratings yet
- Chapter 02Document46 pagesChapter 02JA M ESNo ratings yet
- Universal Health Care-StudentsDocument72 pagesUniversal Health Care-StudentsDoc AchondoNo ratings yet
- Research Article Willingness To Pay For Social Health Insurance and Associated Factors Among Health Care Providers in Addis Ababa, EthiopiaDocument7 pagesResearch Article Willingness To Pay For Social Health Insurance and Associated Factors Among Health Care Providers in Addis Ababa, EthiopiaaisyahNo ratings yet
- Alliancehpsr KenyaabridgedprimasysDocument12 pagesAlliancehpsr Kenyaabridgedprimasysdisposable101No ratings yet
- RPRH Law (RA 10354) Report, 2015 (Popular Version) - Min PDFDocument40 pagesRPRH Law (RA 10354) Report, 2015 (Popular Version) - Min PDFRuzzell AlvarezNo ratings yet
- Ghana - Telemed.v1.060523 Copy 2Document13 pagesGhana - Telemed.v1.060523 Copy 2mpvsx2mnggNo ratings yet
- Marketoverview 0319Document4 pagesMarketoverview 0319Karim DakhchNo ratings yet
- Importance of Health Economics For Health Professionals in NepalDocument2 pagesImportance of Health Economics For Health Professionals in NepalAswiniieNo ratings yet
- 03 Vision 2020 The Right To SightDocument9 pages03 Vision 2020 The Right To SightMwanja MosesNo ratings yet
- Chapter ThreeDocument4 pagesChapter ThreeMitzi MaureenNo ratings yet
- Analysis of Out-of-Pocket Expenditures in The Philippines: V G T. U N A O. CDocument31 pagesAnalysis of Out-of-Pocket Expenditures in The Philippines: V G T. U N A O. CJomer GonzalesNo ratings yet
- HDFC Pharma and Healthcare Fund - Investor PresentationDocument26 pagesHDFC Pharma and Healthcare Fund - Investor Presentationsheikh abdullah aleemNo ratings yet
- Risk Pooling Elaine Baruwa FINAL ENGDocument15 pagesRisk Pooling Elaine Baruwa FINAL ENGMonika Noviena SusantoNo ratings yet
- At A Glance: The Philippine Health Care System: MedicinesDocument15 pagesAt A Glance: The Philippine Health Care System: MedicinesEdrea Aquino MendezNo ratings yet
- Up0023 PDF EngDocument20 pagesUp0023 PDF EngAlejandro Rojas PrietoNo ratings yet
- NATHEALTH HealthFinancing ThoughtLeadershipPaperDocument48 pagesNATHEALTH HealthFinancing ThoughtLeadershipPaperVansh AggarwalNo ratings yet
- DOH Administrative Order No 2020 0043Document11 pagesDOH Administrative Order No 2020 0043Marie AsyethNo ratings yet
- Debate LinesDocument4 pagesDebate LinesLyte LightNo ratings yet
- DOH Annual Report2014a PDFDocument28 pagesDOH Annual Report2014a PDFSheri WilliamsNo ratings yet
- PHDSDocument3 pagesPHDSKathrina Doroneo (rina)No ratings yet
- Competition in Health ServicesDocument8 pagesCompetition in Health ServicesJASSEN BAZANNo ratings yet
- state of The Industry 2019: Financial Condition and Trends in Home and Community-Based CareDocument16 pagesstate of The Industry 2019: Financial Condition and Trends in Home and Community-Based CareEdmondsonNo ratings yet
- HPAD MT Exam - Monica Angelique RamosDocument12 pagesHPAD MT Exam - Monica Angelique RamosMA Orejas RamosNo ratings yet
- Unit 2Document14 pagesUnit 2Moumita MondalNo ratings yet
- SA LIII 42 201018 Utsa PatnaikDocument2 pagesSA LIII 42 201018 Utsa PatnaikRaghubalan DurairajuNo ratings yet
- Economy GauraDocument100 pagesEconomy GaurasudarshanNo ratings yet
- Philippine Health SituationDocument4 pagesPhilippine Health SituationMonsour SalazarNo ratings yet
- EXPLAINER: What Filipinos Can Expect From The Universal Health Care Law?Document14 pagesEXPLAINER: What Filipinos Can Expect From The Universal Health Care Law?Corina Faye RosarioNo ratings yet
- Paraguayan Health System MCMP PresentationDocument23 pagesParaguayan Health System MCMP PresentationcamimontufarNo ratings yet
- Philippine Health AgendaDocument9 pagesPhilippine Health AgendaCzeazarNo ratings yet
- The National Health Policy and MalnutritionDocument11 pagesThe National Health Policy and Malnutritiondishydashy88No ratings yet
- Universal Healthcare in The Philippine Setting: October 2015Document12 pagesUniversal Healthcare in The Philippine Setting: October 2015Sharlot Jimenez AbdurahmanNo ratings yet
- FMA1 AbraciaDocument3 pagesFMA1 AbraciaMel Angelo AbraciaNo ratings yet
- EHealth in IndiaDocument28 pagesEHealth in IndiasunnyNo ratings yet
- Approved UHC FAQsDocument8 pagesApproved UHC FAQsCDOHO-IloiloNo ratings yet
- HEALTHCARE SERVICE QUALITY AND PATIENT SATISFACTION IN OMANI PUBLIC HOSPITALS THROUGHOUT COVID-19 ERA: AN EMPIRICAL INVESTIGATIONFrom EverandHEALTHCARE SERVICE QUALITY AND PATIENT SATISFACTION IN OMANI PUBLIC HOSPITALS THROUGHOUT COVID-19 ERA: AN EMPIRICAL INVESTIGATIONNo ratings yet
- Pandemic Preparedness and Response Strategies: COVID-19 Lessons from the Republic of Korea, Thailand, and Viet NamFrom EverandPandemic Preparedness and Response Strategies: COVID-19 Lessons from the Republic of Korea, Thailand, and Viet NamNo ratings yet
- Intrapartum CareDocument12 pagesIntrapartum CarekasjdkasNo ratings yet
- Pdev Module CPT 21 2Document6 pagesPdev Module CPT 21 2kasjdkasNo ratings yet
- NCP LDocument2 pagesNCP LkasjdkasNo ratings yet
- Aide MemoirDocument2 pagesAide MemoirkasjdkasNo ratings yet
- Musculoskeletal SystemDocument15 pagesMusculoskeletal SystemkasjdkasNo ratings yet
- NotesDocument3 pagesNoteskasjdkasNo ratings yet
- Impact oDocument2 pagesImpact okasjdkasNo ratings yet
- Movie AnalysisDocument2 pagesMovie AnalysiskasjdkasNo ratings yet
- Globalization After Worldwar 1Document1 pageGlobalization After Worldwar 1kasjdkasNo ratings yet
- World War 1 1914 18 G5Document6 pagesWorld War 1 1914 18 G5kasjdkasNo ratings yet
- The Worst Food Crisis in DECADESDocument1 pageThe Worst Food Crisis in DECADESkasjdkasNo ratings yet
- Mallare Woreline 1914 1918Document11 pagesMallare Woreline 1914 1918kasjdkasNo ratings yet
- MovieDocument1 pageMoviekasjdkasNo ratings yet
- STATIC Humss12j CWDocument2 pagesSTATIC Humss12j CWkasjdkasNo ratings yet
- Mallare Impact of WW1Document3 pagesMallare Impact of WW1kasjdkasNo ratings yet
- Pre Act 4Document1 pagePre Act 4kasjdkasNo ratings yet
- Disciplines and Ideas in The Social Sciences - Group 4Document3 pagesDisciplines and Ideas in The Social Sciences - Group 4kasjdkasNo ratings yet
- PATHFIT4 Module 1 (Overview and Brief History of Recreational Activities)Document5 pagesPATHFIT4 Module 1 (Overview and Brief History of Recreational Activities)kasjdkasNo ratings yet
- Lesson 2.2 FINALS - POLITICAL AND LEADERSHIP STRUCTURESDocument7 pagesLesson 2.2 FINALS - POLITICAL AND LEADERSHIP STRUCTURESkasjdkasNo ratings yet
- University of The Cordillera1Document3 pagesUniversity of The Cordillera1kasjdkasNo ratings yet
- The Thing For Sunday Pneumonia FlavouredDocument3 pagesThe Thing For Sunday Pneumonia FlavouredkasjdkasNo ratings yet
- The Clinical Teacher - 2020 - Horner - Outpatient Learning Perspectives at A UK HospitalDocument8 pagesThe Clinical Teacher - 2020 - Horner - Outpatient Learning Perspectives at A UK HospitalkasjdkasNo ratings yet
- Letter of ExplanationDocument1 pageLetter of ExplanationkasjdkasNo ratings yet
- NCM 102 M5&6 StudentDocument4 pagesNCM 102 M5&6 StudentkasjdkasNo ratings yet
- Report BroadcastingDocument5 pagesReport BroadcastingkasjdkasNo ratings yet
- Death PenaltyDocument14 pagesDeath PenaltykasjdkasNo ratings yet
- Journal TemplateDocument2 pagesJournal TemplatekasjdkasNo ratings yet
- Plasmodium FalciparumDocument4 pagesPlasmodium FalciparumkasjdkasNo ratings yet
- Teaching-Plan-Health-Education-Plan-Diabetes Mellitus TYPE IIDocument3 pagesTeaching-Plan-Health-Education-Plan-Diabetes Mellitus TYPE IIkasjdkasNo ratings yet
- Apgar and Other NB Care Procedure MarianDocument88 pagesApgar and Other NB Care Procedure MariankasjdkasNo ratings yet
- Bbbm4103 Bank Management - May Semester 2020Document25 pagesBbbm4103 Bank Management - May Semester 2020VithiaNo ratings yet
- Bike PolicyDocument2 pagesBike PolicyJagjeet SinghNo ratings yet
- Contract of Employment (Business Development Manager) : Know All Men by These PresentsDocument3 pagesContract of Employment (Business Development Manager) : Know All Men by These PresentsDexalcantara scsj2020No ratings yet
- DataDocument6 pagesDataNitish BhardwajNo ratings yet
- Hallegatte2020 Article FromPovertyToDisasterAndBackARDocument25 pagesHallegatte2020 Article FromPovertyToDisasterAndBackARKalshan DulanjaNo ratings yet
- What Is An Advance Payment?Document2 pagesWhat Is An Advance Payment?Niño Rey LopezNo ratings yet
- A Study in Financial Performance Analysis of Selected Mutual Funds in IndiaDocument8 pagesA Study in Financial Performance Analysis of Selected Mutual Funds in IndiaSurya SNo ratings yet
- 5834 GETCO 17 47 19 Tender-No.05 - OnlineDocument43 pages5834 GETCO 17 47 19 Tender-No.05 - OnlineJignesh V. KhimsuriyaNo ratings yet
- Mercantile Law Past Papers PDFDocument60 pagesMercantile Law Past Papers PDFMuhammad YahyaNo ratings yet
- Benefit Illustration For HDFC Life Sanchay Par AdvantageDocument3 pagesBenefit Illustration For HDFC Life Sanchay Par Advantagekesk32No ratings yet
- Business Finance - 12 - Third - Week 5Document11 pagesBusiness Finance - 12 - Third - Week 5AngelicaHermoParasNo ratings yet
- Annual Report 2017-18Document100 pagesAnnual Report 2017-18komaltagraNo ratings yet
- Sukanya Samriddhi Yojana Calculator - SSY Calculator OnlineDocument12 pagesSukanya Samriddhi Yojana Calculator - SSY Calculator OnlineAjmeerNo ratings yet
- Mou Mitchelle Chiedza MavenganoDocument6 pagesMou Mitchelle Chiedza Mavenganomavenganomitchell2No ratings yet
- TAX 1.docx KeyDocument94 pagesTAX 1.docx Keymario1962No ratings yet
- MTQ2 Deductions From Gross IncomeDocument4 pagesMTQ2 Deductions From Gross IncomeEISEN BELWIGANNo ratings yet
- Real Na To Noynoy Aquino's Distribution in Every SectorDocument9 pagesReal Na To Noynoy Aquino's Distribution in Every SectorAnna Mae RiveraNo ratings yet
- Standing Instruction Form Through IndusInd Bank Account-2Document1 pageStanding Instruction Form Through IndusInd Bank Account-2SonuNo ratings yet
- Lab Companies ActDocument50 pagesLab Companies ActAarchi AgrawalNo ratings yet
- 2022 Cecp Summit Summary Report: In-Person!Document6 pages2022 Cecp Summit Summary Report: In-Person!borjaNo ratings yet
- Bajaj Allianz Guarantee Assure: A Non-Linked Endowment PlanDocument9 pagesBajaj Allianz Guarantee Assure: A Non-Linked Endowment PlanBhaskarNo ratings yet
- Business Law - MMS - Session 8Document10 pagesBusiness Law - MMS - Session 8varyushNo ratings yet
- Aviation: Chapter 1 - The Airline Industry Chapter 2 - Accounting and Auditing in An Airline EnvironmentDocument15 pagesAviation: Chapter 1 - The Airline Industry Chapter 2 - Accounting and Auditing in An Airline EnvironmentJessa Gay Cartagena TorresNo ratings yet
- Om PrakashDocument2 pagesOm Prakashanshi100% (1)
- Motor Insurance - Two Wheeler Liability Only: Certificate of Insurance Cum Policy ScheduleDocument3 pagesMotor Insurance - Two Wheeler Liability Only: Certificate of Insurance Cum Policy ScheduleRakesh VermaNo ratings yet
- Fy 2023 Budget in BriefDocument174 pagesFy 2023 Budget in BriefTim BrownNo ratings yet
- Checkbook Register SampleDocument8 pagesCheckbook Register SampleKuntal ShahNo ratings yet
- Insurance ContractsDocument1 pageInsurance ContractsRicababeNo ratings yet
- BEDocument14 pagesBENguyễn Phương UyênNo ratings yet