You might also like
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (590)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (540)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (401)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5813)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (844)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (822)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (897)
- Massey - A Book of The Beginnings (Vol. I)Document516 pagesMassey - A Book of The Beginnings (Vol. I)Celephaïs Press / Unspeakable Press (Leng)100% (8)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (348)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1092)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Savage Battletech Rules - Revision 12Document56 pagesSavage Battletech Rules - Revision 12jasonstierle100% (8)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Vocabulary: Roman EducationDocument14 pagesVocabulary: Roman EducationBibek Chapagain100% (1)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Age of Ashes - Player's Guide PDFDocument11 pagesAge of Ashes - Player's Guide PDFBlack KnightNo ratings yet
- Z Engineer Interview PDFDocument36 pagesZ Engineer Interview PDFDFNo ratings yet
- Deductive InductiveDocument30 pagesDeductive InductiveJerome Salazar Caballero0% (1)
- Descripcion de 28 Pulsos Segun MTCDocument4 pagesDescripcion de 28 Pulsos Segun MTCJujosomaNo ratings yet
- The 28 Pulse QualitiesDocument1 pageThe 28 Pulse QualitiesJujosomaNo ratings yet
- Special PointsseparateDocument18 pagesSpecial PointsseparateJujosomaNo ratings yet
- Protocolos Auriculoterapia by Juan Jose SotoDocument3 pagesProtocolos Auriculoterapia by Juan Jose SotoJujosomaNo ratings yet
- Functions in Python MCQDocument4 pagesFunctions in Python MCQManpreet AroraNo ratings yet
- Location Facilities QuizDocument29 pagesLocation Facilities QuizDiane CabiscuelasNo ratings yet
- HTW 1 3 1nDocument241 pagesHTW 1 3 1nmingo622No ratings yet
- (Subclass) (Barbarian) Path of The DoomslayerDocument1 page(Subclass) (Barbarian) Path of The DoomslayerChiroptera419No ratings yet
- Brand Hate Thesis FFFDocument101 pagesBrand Hate Thesis FFFAmbreen ZahraNo ratings yet
- Kaloji Narayana Rao University of Health Sciences, Warangal, Telangana - 506007Document9 pagesKaloji Narayana Rao University of Health Sciences, Warangal, Telangana - 506007Sriram KasturiNo ratings yet
- TC1767 Microcontroller Manual PDFDocument1,892 pagesTC1767 Microcontroller Manual PDFpierpaolo aldrigo100% (1)
- Control Systems III Course Guide 2016Document11 pagesControl Systems III Course Guide 2016John LionelNo ratings yet
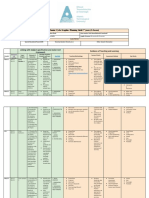
- Planning Grid Junior Cert Graphics 2nd YearsDocument5 pagesPlanning Grid Junior Cert Graphics 2nd Yearsapi-547735446No ratings yet
- The Synergy Between Neoliberalism and CommunitarianismDocument12 pagesThe Synergy Between Neoliberalism and Communitarianismsamar1973No ratings yet
- Senate 29sept 2013Document136 pagesSenate 29sept 2013RajanSharmaNo ratings yet
- Ce8701 Estimation, Costing and Valuation Engineering R17Document1 pageCe8701 Estimation, Costing and Valuation Engineering R17Gururaj SivaprakasamNo ratings yet
- 5 Marxism and EdnDocument4 pages5 Marxism and EdnIrene TeyaNo ratings yet
- Art of Indus ValleyDocument10 pagesArt of Indus ValleyThejasvi AtmadasaNo ratings yet
- On Performance AppraisalDocument40 pagesOn Performance AppraisalChander SekharNo ratings yet
- AurangzebDocument5 pagesAurangzebAdulrehman KhanNo ratings yet
- ch2 1 25Document25 pagesch2 1 25gianfranco361No ratings yet
- ÜDS-KPDS İPUÇLARI-NOTLAR - ÖnemliDocument30 pagesÜDS-KPDS İPUÇLARI-NOTLAR - ÖnemliRe KANo ratings yet
- Assignment 3-Prb 2Document12 pagesAssignment 3-Prb 2JazamNo ratings yet
- Gauge Theory: José Figueroa-O'FarrillDocument37 pagesGauge Theory: José Figueroa-O'Farrillcifarha venantNo ratings yet
- Survey Report DLPDocument4 pagesSurvey Report DLPMark Joey Arendain MuñozNo ratings yet
- Afgitmolfm PDFDocument411 pagesAfgitmolfm PDFSelleeeNo ratings yet
- Ch01 RETAIL MARKETING EnvironmentDocument10 pagesCh01 RETAIL MARKETING Environmenttb7976skNo ratings yet