You might also like
- BriefingDocument BPAC Topic1A ConsiderationsForIronManagementDocument19 pagesBriefingDocument BPAC Topic1A ConsiderationsForIronManagementGilbertmichyNo ratings yet
- Anemia Besi Di Pasien HFDocument14 pagesAnemia Besi Di Pasien HFAdipNo ratings yet
- BM and Iron ProfileDocument5 pagesBM and Iron ProfileShila SahaNo ratings yet
- Using The Hemoglobin Content of Reticulocytes (RET-He) To Evaluate Anemia in Patients With CancerDocument7 pagesUsing The Hemoglobin Content of Reticulocytes (RET-He) To Evaluate Anemia in Patients With CancerMekar PalupiNo ratings yet
- Frequent Blood Donations Alter Susceptibility of Red Blood Cells To Storage and Stress Induced HemolysisDocument12 pagesFrequent Blood Donations Alter Susceptibility of Red Blood Cells To Storage and Stress Induced HemolysisYuendri IrawantoNo ratings yet
- Inappropriate Expression of Hepcidin by Liver CongestionDocument10 pagesInappropriate Expression of Hepcidin by Liver CongestionEduardo Henrique de Sousa SalvinoNo ratings yet
- Joo Sten 2017Document7 pagesJoo Sten 2017langit rizki yuditamaNo ratings yet
- NIH Public Access: Restless Legs Syndrome, Pica, and Iron Status in Blood DonorsDocument15 pagesNIH Public Access: Restless Legs Syndrome, Pica, and Iron Status in Blood DonorsmuiNo ratings yet
- Pi Is 1548559519301144Document20 pagesPi Is 1548559519301144hemer hadyn calderon alvites0% (1)
- Main Article - BM PancytopeniaDocument10 pagesMain Article - BM PancytopeniaAbdur Rachman Ba'abdullahNo ratings yet
- Anem 2Document6 pagesAnem 2vamiqrasoolNo ratings yet
- Pone 0167987 PDFDocument12 pagesPone 0167987 PDFErick AlvarezNo ratings yet
- Ni Hms 590004Document24 pagesNi Hms 590004Muhammad SaqriNo ratings yet
- Besarab 2010Document13 pagesBesarab 2010josephNo ratings yet
- Camaschella 2017Document9 pagesCamaschella 2017Walter Jhon Delgadillo Arone0% (1)
- Ehac 569Document14 pagesEhac 569Binod KumarNo ratings yet
- Credibility of The Measurement of Serum Ferritin and Transferrin Receptor As Indicators of Iron Deficiency Anemia in Hemodialysis PatientsDocument5 pagesCredibility of The Measurement of Serum Ferritin and Transferrin Receptor As Indicators of Iron Deficiency Anemia in Hemodialysis PatientsTanveerNo ratings yet
- Paternostro 2020Document9 pagesPaternostro 2020my accountNo ratings yet
- A Review of Iron Overload in Beta-Thalassemia Major, and A Discussion On Alternative Potent Iron Chelation TargetsDocument9 pagesA Review of Iron Overload in Beta-Thalassemia Major, and A Discussion On Alternative Potent Iron Chelation TargetsFalisha Belvia KairinNo ratings yet
- HHS Public Access: The Role of Iron Repletion in Adult Iron Deficiency Anemia and Other DiseasesDocument18 pagesHHS Public Access: The Role of Iron Repletion in Adult Iron Deficiency Anemia and Other DiseasesKingPasta88 premiereDesignVIDEONo ratings yet
- Assessment of Iron Deficiency Anemia Among Patients Attending Kigali University Teaching HospitalDocument5 pagesAssessment of Iron Deficiency Anemia Among Patients Attending Kigali University Teaching HospitalAzzam SaqrNo ratings yet
- Iron Deficiency Anemia in Chronic Liver Disease: Etiopathogenesis, Diagnosis and TreatmentDocument9 pagesIron Deficiency Anemia in Chronic Liver Disease: Etiopathogenesis, Diagnosis and TreatmentOcha24 TupamahuNo ratings yet
- Serum Ferritin As An Indicator of Iron Status: What Do We Need To Know?Document6 pagesSerum Ferritin As An Indicator of Iron Status: What Do We Need To Know?udjkwNo ratings yet
- Burden 2018Document2 pagesBurden 2018yohann GonsalvesNo ratings yet
- Serum Transferrin Receptor and Transferrin Receptor-Ferritin Index Identify Healthy Subjects With Subclinical Iron DeficitsDocument6 pagesSerum Transferrin Receptor and Transferrin Receptor-Ferritin Index Identify Healthy Subjects With Subclinical Iron DeficitsekoNo ratings yet
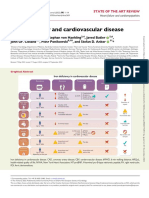
- Iron Deficiency and Cardiovascular DiseaseDocument14 pagesIron Deficiency and Cardiovascular DiseasemiguelalmenarezNo ratings yet
- Reticulocyte hemoglobin content testDocument4 pagesReticulocyte hemoglobin content testLoudry ElfaNo ratings yet
- Iron Deficiency Anemia in Chronic Kidney Disease: ReviewDocument7 pagesIron Deficiency Anemia in Chronic Kidney Disease: ReviewSundas Ejaz100% (1)
- Iron Deficiency in Heart Failure: An OverviewDocument11 pagesIron Deficiency in Heart Failure: An OverviewFelipe SennNo ratings yet
- Reticulocyte Hemoglobin Equivalent As A Potential Marker PDFDocument10 pagesReticulocyte Hemoglobin Equivalent As A Potential Marker PDFFrancoNo ratings yet
- Iron de Ficiency: An Emerging Therapeutic Target in Heart FailureDocument8 pagesIron de Ficiency: An Emerging Therapeutic Target in Heart FailureNastitie Cinintya NurzihanNo ratings yet
- NIH Public Access: Author ManuscriptDocument22 pagesNIH Public Access: Author ManuscriptLolaNo ratings yet
- Page 2010Document8 pagesPage 2010Anonymous 6dMqKOvNo ratings yet
- Iron Deficiency and Blood Donation.Document12 pagesIron Deficiency and Blood Donation.HECTOR ESTRELLA TOPETENo ratings yet
- Iron Overload in Beta Thalassemia PDFDocument5 pagesIron Overload in Beta Thalassemia PDFyesikaNo ratings yet
- Relation of Iron Status To Prognosis After Acute Coronary SyndromeDocument9 pagesRelation of Iron Status To Prognosis After Acute Coronary SyndromeselvianaNo ratings yet
- Anemia of Chronic DiseaseDocument2 pagesAnemia of Chronic DiseasejuanabNo ratings yet
- Deficiencia de HierroDocument12 pagesDeficiencia de HierrofulanotaNo ratings yet
- Iron Deficiency Risk in Chronic Heart FailureDocument1 pageIron Deficiency Risk in Chronic Heart FailureAri WoroNo ratings yet
- Alt Ast - Serum FerritinDocument10 pagesAlt Ast - Serum FerritinMino TaeNo ratings yet
- Subclinical Iron Deficiency in Non-Anemic Individuals: A Retrospective Analysis of Korean Health ExamineesDocument1 pageSubclinical Iron Deficiency in Non-Anemic Individuals: A Retrospective Analysis of Korean Health ExamineesHafizzanovian HanNo ratings yet
- Anemia of Chronic DiseaseDocument5 pagesAnemia of Chronic DiseaseGufront MustofaNo ratings yet
- Molecular Mechanisms of Hepcidin Regulation - Implications For The Anemia of CKDDocument16 pagesMolecular Mechanisms of Hepcidin Regulation - Implications For The Anemia of CKDGading AuroraNo ratings yet
- 2021 Iron Replacement Therapy in Heart Failure A Literature ReviewDocument11 pages2021 Iron Replacement Therapy in Heart Failure A Literature ReviewSiswanto H. AzwarNo ratings yet
- Paediatrica Indonesiana: Fajar Subroto, MD Bulan Ginting Munthe, MD Najib Advani, MD Agus Firmansyah, MD, PHDDocument4 pagesPaediatrica Indonesiana: Fajar Subroto, MD Bulan Ginting Munthe, MD Najib Advani, MD Agus Firmansyah, MD, PHDmuhamadmukhlisNo ratings yet
- Intravenous Iron and Maintenance Hemodialysis: CorrespondenceDocument3 pagesIntravenous Iron and Maintenance Hemodialysis: CorrespondenceSamanthaNo ratings yet
- Jclinpath00120 0042Document3 pagesJclinpath00120 0042Anderson LondoñoNo ratings yet
- 8 PDFDocument8 pages8 PDFSofia FurtadoNo ratings yet
- Validation Biochemistry MeasurementDocument35 pagesValidation Biochemistry Measurementhudan aziziNo ratings yet
- Nephrol. Dial. Transplant. 2005 Klutstein Vii7 Vii10Document4 pagesNephrol. Dial. Transplant. 2005 Klutstein Vii7 Vii10Indah PratiwiNo ratings yet
- The Coexistence of Polycythemia Vera and Iron Deficiency AnemiaDocument3 pagesThe Coexistence of Polycythemia Vera and Iron Deficiency AnemiaasclepiuspdfsNo ratings yet
- Diagnostic Importance of Hepcidin, Soluble TransferrinDocument4 pagesDiagnostic Importance of Hepcidin, Soluble TransferrinushaNo ratings yet
- What Are Some Current Issues and Controversies About IronDocument2 pagesWhat Are Some Current Issues and Controversies About IronDinda SaviraNo ratings yet
- 10 12982jams 2023 058Document7 pages10 12982jams 2023 058ahmedradwan2005No ratings yet
- Soluble Transferrin Receptors and Reticulocyte Hemoglobin Concentration in The Assessment in Iron Deficiency in Hemodialysis PatientsDocument9 pagesSoluble Transferrin Receptors and Reticulocyte Hemoglobin Concentration in The Assessment in Iron Deficiency in Hemodialysis PatientsMuhammad HafidNo ratings yet
- Erythrocyte Indices As Differential Diagnostic Biomarkers of Iron Deficiency Anemia and ThalassemiaDocument6 pagesErythrocyte Indices As Differential Diagnostic Biomarkers of Iron Deficiency Anemia and ThalassemiadesaklaksmiNo ratings yet
- ArticlesDocument6 pagesArticlesbedahfkumiNo ratings yet
- Management of Iron de Ficiency: Shuoyan Ning and Michelle P. ZellerDocument8 pagesManagement of Iron de Ficiency: Shuoyan Ning and Michelle P. ZellerGeorgina Aguilar GallardoNo ratings yet
- Iron Deficiency Anemia Diagnosis and Treatment InsightsDocument6 pagesIron Deficiency Anemia Diagnosis and Treatment InsightschameleonNo ratings yet
- Iron SupplementationDocument10 pagesIron SupplementationAnonymous 6dMqKOvNo ratings yet
- Page 2010Document8 pagesPage 2010Anonymous 6dMqKOvNo ratings yet
- Halo Assalamualaykum Terimakasih WassalamualaykumDocument1 pageHalo Assalamualaykum Terimakasih WassalamualaykumAnonymous 6dMqKOvNo ratings yet
- Serum Ferritin in Plateletpheresis and Whole Blood Donors 2016Document5 pagesSerum Ferritin in Plateletpheresis and Whole Blood Donors 2016azizk83No ratings yet
- Poster IcmhsDocument1 pagePoster IcmhsAnonymous 6dMqKOvNo ratings yet
- ATEC-AUTISM Spectrum Disorder ChecklistDocument1 pageATEC-AUTISM Spectrum Disorder ChecklistAnonymous jH2v0B100% (1)
- Anonim 2011Document1 pageAnonim 2011Anonymous 6dMqKOvNo ratings yet
- About 1 in 88 Children Has Been Identified With An Autism Spectrum DisorderDocument1 pageAbout 1 in 88 Children Has Been Identified With An Autism Spectrum DisorderAnonymous 6dMqKOvNo ratings yet
- Jadwal Uji Proposal KTI, Mhs 2011Document7 pagesJadwal Uji Proposal KTI, Mhs 2011Anonymous 6dMqKOvNo ratings yet
- Difficulty Falling Asleep or Insomnia Is One of Health Problems in ElderlyDocument1 pageDifficulty Falling Asleep or Insomnia Is One of Health Problems in ElderlyAnonymous 6dMqKOvNo ratings yet
- Hubungan Antara ObesitasDocument1 pageHubungan Antara ObesitasAnonymous 6dMqKOvNo ratings yet
- A Prospective Study of The Emergence of Early Behavioral Signs of AutismDocument4 pagesA Prospective Study of The Emergence of Early Behavioral Signs of AutismAnonymous 6dMqKOvNo ratings yet
- Waktu PelaksanaanDocument2 pagesWaktu PelaksanaanAnonymous 6dMqKOvNo ratings yet
- Smoking's Impact on Musculoskeletal Pain and Bone DensityDocument17 pagesSmoking's Impact on Musculoskeletal Pain and Bone DensityAnonymous 6dMqKOvNo ratings yet
- A4 paper text format for IJECE submissionsDocument1 pageA4 paper text format for IJECE submissionsAnonymous 6dMqKOvNo ratings yet
- BeGH TemplatesDocument8 pagesBeGH TemplatesBhie BhieNo ratings yet
- Chapter 013Document36 pagesChapter 013Aria LeNo ratings yet
- ElisaDocument5 pagesElisaDennis ValdezNo ratings yet
- Contoh SoapDocument11 pagesContoh SoapIlham riandaNo ratings yet
- Historical SupplyDocument5 pagesHistorical Supplylara torricoNo ratings yet
- Implantology and The Severely Resorbed Edentulous MandibleDocument9 pagesImplantology and The Severely Resorbed Edentulous MandibleAfiz ZullahNo ratings yet
- 239 910 1 PB PDFDocument133 pages239 910 1 PB PDFEres TriasaNo ratings yet
- Introduction to Public Health NursingDocument37 pagesIntroduction to Public Health NursingKailash NagarNo ratings yet
- OB Quiz 1: Nishath Sarwath's 10-question OB nursing examDocument5 pagesOB Quiz 1: Nishath Sarwath's 10-question OB nursing examNishath SarwathNo ratings yet
- Abnormal Labor. BBBB WWPPTXDocument53 pagesAbnormal Labor. BBBB WWPPTXHamss Ahmed100% (2)
- Chinese Auricular Acupuncture 2nd EditionDocument57 pagesChinese Auricular Acupuncture 2nd Editiongordon.gibson456100% (37)
- Free Modern Neuromuscular Techniques PDFDocument6 pagesFree Modern Neuromuscular Techniques PDFStiven FloresNo ratings yet
- (10920684 - Neurosurgical Focus) Hitler's ParkinsonismDocument5 pages(10920684 - Neurosurgical Focus) Hitler's ParkinsonismStuti MardiaNo ratings yet
- Emrcp CNS 38-62Document22 pagesEmrcp CNS 38-62dryusufsNo ratings yet
- Pleno Skenario A TB Dewasa-1Document58 pagesPleno Skenario A TB Dewasa-1ninja sanjeninNo ratings yet
- Urea Cycle DefectsDocument12 pagesUrea Cycle DefectsAleksandra RadonjićNo ratings yet
- ECG Report: An Overview of ElectrocardiographyDocument5 pagesECG Report: An Overview of Electrocardiographyالحارث فخري فياض احمدNo ratings yet
- Stanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013Document3 pagesStanford Hospital & Clinics Antimicrobial Dosing Reference Guide 2013SANCHOSKYNo ratings yet
- In-Press Article: Outcomes Following Severe Distal Tibial, Ankle, And/or Mid/Hindfoot TraumaDocument10 pagesIn-Press Article: Outcomes Following Severe Distal Tibial, Ankle, And/or Mid/Hindfoot TraumaDeng PanNo ratings yet
- Omphalocele and GastroschisisDocument12 pagesOmphalocele and Gastroschisisluisisea100% (1)
- Unit 8Document34 pagesUnit 8Deta Meila PutriNo ratings yet
- Stop The Bleed Booklet FinalDocument16 pagesStop The Bleed Booklet FinalUrsula MalauNo ratings yet
- Gordon's 11 Functional Health PatternDocument2 pagesGordon's 11 Functional Health PatternWendell AcuñaNo ratings yet
- General Stress Level of SHS ABM Students in Their Specialized SubjectDocument4 pagesGeneral Stress Level of SHS ABM Students in Their Specialized SubjectThons Nacu LisingNo ratings yet
- HS 2212 Wa U5Document4 pagesHS 2212 Wa U5bnvjNo ratings yet
- Lesson 1 - Matching HeadingDocument17 pagesLesson 1 - Matching HeadingHà ĐàoNo ratings yet
- Sample Infection Control Risk AssessmentDocument2 pagesSample Infection Control Risk AssessmentMj Celuler100% (1)
- ScriptDocument3 pagesScriptVictoria Dinio FernandoNo ratings yet
- Name of Drug Mechanism of Action Indication Contraindication Side Effects Adverse Effects Nursing Consideration IndicationDocument2 pagesName of Drug Mechanism of Action Indication Contraindication Side Effects Adverse Effects Nursing Consideration IndicationBrian BaggayanNo ratings yet
- Diseases of Oral Cavity, Salivary Glands and Jaws (K00-K14) : Search (Advanced Search)Document13 pagesDiseases of Oral Cavity, Salivary Glands and Jaws (K00-K14) : Search (Advanced Search)Ria MarthantiNo ratings yet