You might also like
- Voter's ID, Senior Citizen's ID, Driver's License, Passport, Etc.)Document2 pagesVoter's ID, Senior Citizen's ID, Driver's License, Passport, Etc.)AUBREAYNo ratings yet
- TDSB Permission FomrDocument2 pagesTDSB Permission Fomrapi-245241322No ratings yet
- Cloisters Permission Slip 2017Document5 pagesCloisters Permission Slip 2017Casey SchmollNo ratings yet
- SH Summer Events 2012Document2 pagesSH Summer Events 2012NMCStuMinNo ratings yet
- Ncov Advisory Slip - StudentsDocument3 pagesNcov Advisory Slip - StudentsShannon AgarradoNo ratings yet
- NSTP Students WaiverDocument3 pagesNSTP Students WaiverEdwina DelsocorroNo ratings yet
- Updated Travel Request FormDocument1 pageUpdated Travel Request FormAnnie ReifsnyderNo ratings yet
- Parental Consent - 1day Tour PDFDocument1 pageParental Consent - 1day Tour PDFMaricar AytonaNo ratings yet
- Consent Form and Payment Letter FOBISIA Orchestra and Choral Festival Indonesia May 2024Document4 pagesConsent Form and Payment Letter FOBISIA Orchestra and Choral Festival Indonesia May 2024sage.ebony.meadowNo ratings yet
- Costa Rica Koinonia Application PacketDocument5 pagesCosta Rica Koinonia Application PacketWHO OfficeNo ratings yet
- Institute Cervantes Summer 2011 CampsDocument6 pagesInstitute Cervantes Summer 2011 CampsCarissa NicholsNo ratings yet
- Ministry Trip Application 10Document2 pagesMinistry Trip Application 10erichaysehkoNo ratings yet
- TOLC 2016-2017 Enrollment Form PDFDocument3 pagesTOLC 2016-2017 Enrollment Form PDFAnonymous C11nDANo ratings yet
- San Diego YLC Application 2010Document2 pagesSan Diego YLC Application 2010sandiegoylcNo ratings yet
- Migration and Declaration FormsDocument5 pagesMigration and Declaration Formsdeepheat_008No ratings yet
- Travel and Trip Risk Acknowledgement Liability Waiver FormDocument4 pagesTravel and Trip Risk Acknowledgement Liability Waiver Formapi-357423998No ratings yet
- Field TripDocument1 pageField Tripapi-231128403No ratings yet
- SASE ReviewDocument3 pagesSASE ReviewPrincess Alyanah marie OlongNo ratings yet
- Osu AffidavitDocument2 pagesOsu AffidavitFahad AhmedNo ratings yet
- 2012 An GP Risk FormsDocument5 pages2012 An GP Risk FormsRittick GuptaNo ratings yet
- Field Trip Permission Slip FillableDocument1 pageField Trip Permission Slip Fillabletvtcf286v9No ratings yet
- Science Field Trip Permission SlipDocument3 pagesScience Field Trip Permission Slipkboele100% (2)
- IYA BronzeDocument2 pagesIYA BronzeNISTSecOfficeNo ratings yet
- Permission FormDocument2 pagesPermission Formapi-352576584No ratings yet
- 2014 15 y Bas Registration Form Clark PleasantDocument4 pages2014 15 y Bas Registration Form Clark Pleasantapi-231914240No ratings yet
- Affidavit of Parental Consent For InternationalDocument2 pagesAffidavit of Parental Consent For Internationalrxpturous100% (1)
- Zawadi Africa Educational Fund Application Form KenyaDocument8 pagesZawadi Africa Educational Fund Application Form Kenyabriellexena06No ratings yet
- 022 Ole-Life Adventures Participant AgreementDocument12 pages022 Ole-Life Adventures Participant AgreementJoseJuan Temoltzin BNo ratings yet
- Retreat Packet 2014 FINALDocument9 pagesRetreat Packet 2014 FINALconvent3821No ratings yet
- Field Day Permission SlipDocument4 pagesField Day Permission SlipCasey SchmollNo ratings yet
- 2020-2021 International Student Financial Certificate: Undergraduate StudentsDocument2 pages2020-2021 International Student Financial Certificate: Undergraduate StudentshellypurwantoNo ratings yet
- Field Trip PolicyDocument2 pagesField Trip Policyknock medinaNo ratings yet
- DH ParentalReleaseDocument2 pagesDH ParentalReleasetrellon_devteamNo ratings yet
- Statement of Financial SupportDocument2 pagesStatement of Financial SupportRasel AhmedNo ratings yet
- Abq Trip AnnouncementDocument2 pagesAbq Trip Announcementapi-561040045No ratings yet
- 2013 Spring Summer BrochureDocument8 pages2013 Spring Summer Brochurejvirchow17No ratings yet
- Permission Form SnowtubingDocument1 pagePermission Form Snowtubingapi-194561932No ratings yet
- 2013 Spring Summe BrochureDocument8 pages2013 Spring Summe Brochurejvirchow17No ratings yet
- Letter of Undertaking and Waiver (High School) : Family Name, First Name, M.I Nationality City/Address Student NameDocument1 pageLetter of Undertaking and Waiver (High School) : Family Name, First Name, M.I Nationality City/Address Student NameClaudius AlexiusNo ratings yet
- AVI Application FormDocument3 pagesAVI Application FormAding PanganuronNo ratings yet
- Annex BDocument3 pagesAnnex BKevin AlicoNo ratings yet
- USA HomeStayTotal Immersion 2018Document3 pagesUSA HomeStayTotal Immersion 2018Javier SolanoNo ratings yet
- Parents IndustrialDocument2 pagesParents IndustrialBethmi JayawardenaNo ratings yet
- WorkDocument1 pageWorkmk radioNo ratings yet
- InternationalFinancialCertificationForm (FIF)Document2 pagesInternationalFinancialCertificationForm (FIF)Humaid JunedNo ratings yet
- Transfer in InstructionsDocument3 pagesTransfer in InstructionsShashank NateshNo ratings yet
- 2013 Ams NYC Trip June 7-9Document9 pages2013 Ams NYC Trip June 7-9pdalleva0% (1)
- Parental Consent 1Document1 pageParental Consent 1Zippy OcampoNo ratings yet
- OMSA Brisbane Guide 2019 PDFDocument26 pagesOMSA Brisbane Guide 2019 PDFMax A. ChengNo ratings yet
- 2014-15 Aftercare Application Revised 7-30-2014Document11 pages2014-15 Aftercare Application Revised 7-30-2014api-261535186No ratings yet
- Passport Application of Their Minor ChildDocument2 pagesPassport Application of Their Minor ChildMissouri General ContractingNo ratings yet
- 2012 Summer Conditioning BrocherureDocument2 pages2012 Summer Conditioning Brocherureapi-31215843No ratings yet
- E 13 Participant Information Authorization SmallDocument2 pagesE 13 Participant Information Authorization SmallouttherepoetrycampNo ratings yet
- Little Coopers FormDocument2 pagesLittle Coopers Formftimum1No ratings yet
- Korea International School: Field Trip Parent/Guardian Permission FormDocument1 pageKorea International School: Field Trip Parent/Guardian Permission FormJay JangNo ratings yet
- 2023 - 24year 12 ResidentialDocument3 pages2023 - 24year 12 Residentialshiva2302No ratings yet
- Prom Parents Consent FormDocument2 pagesProm Parents Consent FormJoyce AmanteNo ratings yet
- Usa Vpa f02. WaiverDocument1 pageUsa Vpa f02. WaivercmpaguntalanNo ratings yet
- Some Topics in Immigration, Refugees and Exchange Programs ApplicationsFrom EverandSome Topics in Immigration, Refugees and Exchange Programs ApplicationsRating: 5 out of 5 stars5/5 (1)
- Boq Floor Tiling WorksDocument1 pageBoq Floor Tiling WorksISAAC KIPSEREM0% (2)
- Nasoalveolar Moulding Seminar at MalakkaraDocument54 pagesNasoalveolar Moulding Seminar at MalakkaraAshwin100% (1)
- Multiple Choice Questions: Topic Covered Are As FollowsDocument3 pagesMultiple Choice Questions: Topic Covered Are As FollowsBikash SahuNo ratings yet
- 2019 PSRANM Conference Program FinalDocument24 pages2019 PSRANM Conference Program FinalKimmie JordanNo ratings yet
- ALPS 2327 Chemistry Assignment Paper PDFDocument11 pagesALPS 2327 Chemistry Assignment Paper PDFAyushNo ratings yet
- Know Your Customer BrochureDocument4 pagesKnow Your Customer BrochureTEL COMENo ratings yet
- The Production of ParacetamolDocument4 pagesThe Production of ParacetamolBryan Tan100% (2)
- Worksheet. 5. Sexual Reproduction in PlantDocument4 pagesWorksheet. 5. Sexual Reproduction in PlantLeonita SwandjajaNo ratings yet
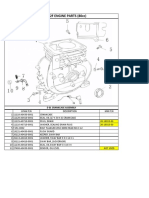
- Lifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblyDocument13 pagesLifan 152F Engine Parts (80Cc) : E 01 Crankcase AssemblySean MurrayNo ratings yet
- Digital Portable 4.0/8.0 KW Dragon LW System Digital Portable 4.0/8.0 KW Dragon LW SystemDocument8 pagesDigital Portable 4.0/8.0 KW Dragon LW System Digital Portable 4.0/8.0 KW Dragon LW Systemteacher_17No ratings yet
- NURS FPX 6410 Assessment 2 Executive Summary To AdministrationDocument7 pagesNURS FPX 6410 Assessment 2 Executive Summary To Administrationzadem5266No ratings yet
- Escape From The Western Diet Summary RevisedDocument3 pagesEscape From The Western Diet Summary Revisedapi-385530863100% (1)
- Benefits of SwimmingDocument3 pagesBenefits of Swimmingaybi pearlNo ratings yet
- Eisenmenger SyndromeDocument6 pagesEisenmenger SyndromeWarkah SanjayaNo ratings yet
- SyllabusDocument2 pagesSyllabusPrakash KumarNo ratings yet
- Comparative Study For Determination of Atracurium Besilate in Presence of Its Toxic Degradant (Laudanosine) by Reversed Phase HPLC and by TLC DensitometryDocument11 pagesComparative Study For Determination of Atracurium Besilate in Presence of Its Toxic Degradant (Laudanosine) by Reversed Phase HPLC and by TLC DensitometrySabrina JonesNo ratings yet
- New Approaches To Cryopreservation of Cells, Tissues, and OrgansDocument19 pagesNew Approaches To Cryopreservation of Cells, Tissues, and OrgansLaura CursaruNo ratings yet
- Octavia Tour BrochureDocument9 pagesOctavia Tour BrochureOvidiuIONo ratings yet
- What Is Nursing?: What Exactly Do Nurses Do?Document3 pagesWhat Is Nursing?: What Exactly Do Nurses Do?mabel yapuraNo ratings yet
- Operations Manual: Conical Burr Coffee GrinderDocument15 pagesOperations Manual: Conical Burr Coffee Grindercherrera73No ratings yet
- Dr. Ashraf Sayeed: Department of OphthalmologyDocument49 pagesDr. Ashraf Sayeed: Department of Ophthalmologysaiful haque100% (1)
- Aaron Magana's Resume, Business AnalystDocument3 pagesAaron Magana's Resume, Business AnalystEmiNo ratings yet
- Huanyang Inverter Instruction (Eng) .300dpi.67pages - OcrDocument70 pagesHuanyang Inverter Instruction (Eng) .300dpi.67pages - Ocrkyuwan kimNo ratings yet
- Investigative Report: Current Trends and Issues in ABM StrandDocument3 pagesInvestigative Report: Current Trends and Issues in ABM StrandVenjo NarcisoNo ratings yet
- MocktestestDocument15 pagesMocktestestAhmed Rasheed AliNo ratings yet
- Week 1Document14 pagesWeek 1kohalehNo ratings yet
- My Project PresentationDocument12 pagesMy Project Presentationkarunasand15No ratings yet
- WPPIL No. 43 of 2014 Uttrakhand High Court Orders For Animals - Abhishek KadyanDocument57 pagesWPPIL No. 43 of 2014 Uttrakhand High Court Orders For Animals - Abhishek KadyanNaresh KadyanNo ratings yet
- Self Esteem and AdjustmentDocument22 pagesSelf Esteem and AdjustmentJan IrishNo ratings yet