You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (122)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (589)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5796)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Basic Economics Module 2020-2021Document108 pagesBasic Economics Module 2020-2021Lhiwell MiñaNo ratings yet
- Oliver Wyman Airline Economic Analysis 2015 2016Document68 pagesOliver Wyman Airline Economic Analysis 2015 2016DharmeshNo ratings yet
- 2000 AP Micro Test 1Document13 pages2000 AP Micro Test 1newtonokewoye75% (4)
- Structural Design Report For Glass BalustradeDocument14 pagesStructural Design Report For Glass Balustradeantonv0421No ratings yet
- LM2324 IdDocument84 pagesLM2324 IdVictor Ryan DellosaNo ratings yet
- 2023 Animo Tips Commercial LawDocument23 pages2023 Animo Tips Commercial LawVictor Ryan DellosaNo ratings yet
- Rental Agreement Shop@TempleDocument7 pagesRental Agreement Shop@TempleVirat VermaNo ratings yet
- Booking Room Conversation With AlternativeDocument2 pagesBooking Room Conversation With Alternativemang yulyNo ratings yet
- Inspection and Acceptance ReportDocument1 pageInspection and Acceptance ReportVictor Ryan DellosaNo ratings yet
- 6.a. Pre-Inspection ReportDocument1 page6.a. Pre-Inspection ReportVictor Ryan DellosaNo ratings yet
- Certification On FairWear and TearDocument1 pageCertification On FairWear and TearVictor Ryan DellosaNo ratings yet
- Request For QuotationDocument3 pagesRequest For QuotationVictor Ryan DellosaNo ratings yet
- Purchase RequestDocument1 pagePurchase RequestVictor Ryan DellosaNo ratings yet
- Purchase OrderDocument1 pagePurchase OrderVictor Ryan DellosaNo ratings yet
- PLR Loc Gov November 2020Document125 pagesPLR Loc Gov November 2020Victor Ryan DellosaNo ratings yet
- Requisition and Issuance SlipDocument1 pageRequisition and Issuance SlipVictor Ryan DellosaNo ratings yet
- PCFReg - Valencia 2Q 2022Document4 pagesPCFReg - Valencia 2Q 2022Victor Ryan DellosaNo ratings yet
- PCF Voucher - FebDocument23 pagesPCF Voucher - FebVictor Ryan DellosaNo ratings yet
- AMENDED TARGETS FPA CY2020 TEMPLATE by Rai - 1Document61 pagesAMENDED TARGETS FPA CY2020 TEMPLATE by Rai - 1Victor Ryan DellosaNo ratings yet
- PLR Election Law November 2020Document81 pagesPLR Election Law November 2020Victor Ryan DellosaNo ratings yet
- PCFReg - Valencia 3Q 2022Document6 pagesPCFReg - Valencia 3Q 2022Victor Ryan DellosaNo ratings yet
- PHILIPPINES - Intercountry AdoptionDocument9 pagesPHILIPPINES - Intercountry AdoptionVictor Ryan DellosaNo ratings yet
- Purchase Order: Bureau of Fire Protection-R7 Alicia Fire Station Poblacion, Alicia, BoholDocument2 pagesPurchase Order: Bureau of Fire Protection-R7 Alicia Fire Station Poblacion, Alicia, BoholVictor Ryan DellosaNo ratings yet
- Bids and Awards Committee Abstract of Canvass / QuotationDocument2 pagesBids and Awards Committee Abstract of Canvass / QuotationVictor Ryan DellosaNo ratings yet
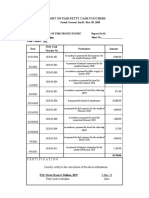
- Report On Paid Petty Cash VoucherDocument2 pagesReport On Paid Petty Cash VoucherVictor Ryan DellosaNo ratings yet
- Report On Paid Petty Cash VoucherDocument2 pagesReport On Paid Petty Cash VoucherVictor Ryan DellosaNo ratings yet
- Form A Number of Establishments (Iso 9001:2015 Quality Objective)Document8 pagesForm A Number of Establishments (Iso 9001:2015 Quality Objective)Victor Ryan DellosaNo ratings yet
- BOQ - Retaining Wall0001Document2 pagesBOQ - Retaining Wall0001Victor OmotoriogunNo ratings yet
- An Introduction To Risk and Return-History of Financial Market ReturnsDocument10 pagesAn Introduction To Risk and Return-History of Financial Market ReturnsanisaNo ratings yet
- Mock 21 HL Paper 2 EconomicsDocument9 pagesMock 21 HL Paper 2 EconomicsiafraserNo ratings yet
- Fall2022 Chapter 7 AssignmentDocument10 pagesFall2022 Chapter 7 Assignmentdo minh tuanNo ratings yet
- Econ 105 Final Exam (Summer 2020)Document7 pagesEcon 105 Final Exam (Summer 2020)Rituraaj SathyaNo ratings yet
- Tourism Economics Research: A Review and AssessmentDocument30 pagesTourism Economics Research: A Review and AssessmentNanda SyafiraNo ratings yet
- A979968895 - 24696 - 22 - 2020 - GD Topics Ca-2Document11 pagesA979968895 - 24696 - 22 - 2020 - GD Topics Ca-2Ashish kumar ThapaNo ratings yet
- Case STUDYDocument3 pagesCase STUDYrohitbatra0% (1)
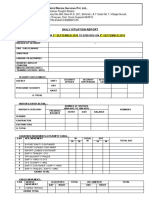
- DSR Seabird SecurityDocument2 pagesDSR Seabird SecurityShandar TamashaNo ratings yet
- Tahsin Yomralioglu Chapter 2: Land ReadjustmentDocument41 pagesTahsin Yomralioglu Chapter 2: Land ReadjustmentkapilprashantkapilNo ratings yet
- General Population Census of Cambodia 2008 Final Census Results Figures at A GlanceDocument4 pagesGeneral Population Census of Cambodia 2008 Final Census Results Figures at A Glanceanh00No ratings yet
- 3 5-SewingDocument4 pages3 5-SewingShahriarNo ratings yet
- Lucy and Melvin Share An Apartment They Spend Some ofDocument1 pageLucy and Melvin Share An Apartment They Spend Some oftrilocksp SinghNo ratings yet
- Available Cars For Sale May 15 2020Document10 pagesAvailable Cars For Sale May 15 2020dyosaNo ratings yet
- 001 Cash Cash Equi Bank Recon and PocDocument5 pages001 Cash Cash Equi Bank Recon and PocArsenio N. RojoNo ratings yet
- ID WASS CourseCalendar-Okt20 INZAGE3Document2 pagesID WASS CourseCalendar-Okt20 INZAGE3robotokabutakuNo ratings yet
- Bedroom VocabularyDocument2 pagesBedroom VocabularyAlondra Joseline Beristain ContrerasNo ratings yet
- Compromise AgreementDocument3 pagesCompromise AgreementLian Dominic GumbanNo ratings yet
- Kimiki Sales Monitoring 2023 - 8-31-2023Document184 pagesKimiki Sales Monitoring 2023 - 8-31-2023JulzNo ratings yet
- The Role of Finance in Supply Chain Management: Lars StemmlerDocument2 pagesThe Role of Finance in Supply Chain Management: Lars StemmlerHernandoNo ratings yet
- Accounting 1Document8 pagesAccounting 1Jane ebonaNo ratings yet
- Unit 6 Producer Behaviour and SupplyDocument23 pagesUnit 6 Producer Behaviour and SupplyGohar Waqas BusinessNo ratings yet
- NEEARAJ 2 STTMTDocument4 pagesNEEARAJ 2 STTMTRohit raagNo ratings yet
- I. Accounting Methods For By-Products: Exercise 3Document2 pagesI. Accounting Methods For By-Products: Exercise 3Crescent OsamuNo ratings yet