You might also like
- Laboratory Quality/Management: A Workbook with an Eye on AccreditationFrom EverandLaboratory Quality/Management: A Workbook with an Eye on AccreditationRating: 5 out of 5 stars5/5 (1)
- Laboratory Management SOP SampleDocument14 pagesLaboratory Management SOP Samplealiana100% (4)
- Quality Control ChecklistDocument3 pagesQuality Control Checklistsheila marie canibasNo ratings yet
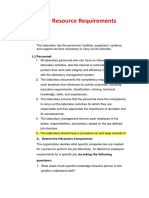
- Chapter 6: Resource Requirements: 1.2 PersonnelDocument17 pagesChapter 6: Resource Requirements: 1.2 PersonnelReama QumsanNo ratings yet
- Quality Manual: Table of Contents: GeneralDocument7 pagesQuality Manual: Table of Contents: Generalmankin901No ratings yet
- ISO 17025 ManualDocument7 pagesISO 17025 Manualvinodkvatsa100% (1)
- Joint Acreditacion de LaboratoriosDocument10 pagesJoint Acreditacion de LaboratoriosRobert Caballero BardalesNo ratings yet
- JOINT COMMISSION INTERNATIONAL ACCREDITATION STANDARDS FOR Clinical LaboratoriesDocument15 pagesJOINT COMMISSION INTERNATIONAL ACCREDITATION STANDARDS FOR Clinical LaboratoriesZulfikar Husni Faruq100% (1)
- SWIFS FBU Quality Manual Program DNA and Serology v1.3 (03.12.2009) 15 PagesDocument15 pagesSWIFS FBU Quality Manual Program DNA and Serology v1.3 (03.12.2009) 15 Pagesjac_blakeNo ratings yet
- Fundamental Points On Glp.Document5 pagesFundamental Points On Glp.Emidinho Emidinho100% (2)
- ORA-LAB.5.2 Personnel Training (v02)Document11 pagesORA-LAB.5.2 Personnel Training (v02)marwa100% (4)
- US Environmental Protection Agency Office of Pesticide ProgramsDocument10 pagesUS Environmental Protection Agency Office of Pesticide ProgramsJeji HirboraNo ratings yet
- WHO AFRO Checklist Assessment Guidelines Jan 2012Document40 pagesWHO AFRO Checklist Assessment Guidelines Jan 2012Rosemary ShirimaNo ratings yet
- Good Laboratory Practice SOPPD102 02Document11 pagesGood Laboratory Practice SOPPD102 02jsembiringNo ratings yet
- Policy and Procedures For Hiring, PromotionsDocument2 pagesPolicy and Procedures For Hiring, PromotionsRazel Ann ElagioNo ratings yet
- 007 2017 Laboratory Evaluation Checklist Laboratory Quality Assurance ProgramDocument10 pages007 2017 Laboratory Evaluation Checklist Laboratory Quality Assurance Programalaa arafaNo ratings yet
- ORA-LAB.4.3 Document Control and Management (v02)Document9 pagesORA-LAB.4.3 Document Control and Management (v02)rajesh sharmaNo ratings yet
- Sample Quality ManualDocument11 pagesSample Quality ManualwalitedisonNo ratings yet
- GFLPDocument40 pagesGFLPayu kristiyaningrumNo ratings yet
- Measurement Traceability PDFDocument7 pagesMeasurement Traceability PDFPrashansa ShresthaNo ratings yet
- ORA-LAB.4.15 Management Review (v02)Document6 pagesORA-LAB.4.15 Management Review (v02)Agus JatmikoNo ratings yet
- Sample Quality Manual For LaboratoriesDocument10 pagesSample Quality Manual For LaboratoriesPhArMaCyGrAdUaTeS50% (2)
- 12 11 2021 10 39 10 F-0217A-DocumentReviewandPre-AssessmentISO17025Rev00Document14 pages12 11 2021 10 39 10 F-0217A-DocumentReviewandPre-AssessmentISO17025Rev00muhammad kamranNo ratings yet
- Blood Banking - System RequirementsDocument24 pagesBlood Banking - System RequirementsJira Jinn ChuaNo ratings yet
- GD-07-QMS - Quality Management System in Testing LaboratoryDocument8 pagesGD-07-QMS - Quality Management System in Testing Laboratorycavalo2080No ratings yet
- Quality Management System Procedure: QSP 4-3-1 - Document ControlDocument5 pagesQuality Management System Procedure: QSP 4-3-1 - Document Controljeric bañaderaNo ratings yet
- Hawassa Poly Technic Collage Water Quality Laboratory Accreditation Experience Sharing ProgramDocument3 pagesHawassa Poly Technic Collage Water Quality Laboratory Accreditation Experience Sharing ProgramJeji HirboraNo ratings yet
- Good Laboratory Practices (BPOM) EngDocument61 pagesGood Laboratory Practices (BPOM) EngWidiyantoNo ratings yet
- Sop Title: Study Team Training and Study Handover SOP Version No: 01 DateDocument5 pagesSop Title: Study Team Training and Study Handover SOP Version No: 01 DateNupur SinghviNo ratings yet
- Documentation Pharmaceutical IndustryDocument102 pagesDocumentation Pharmaceutical IndustryRagulNo ratings yet
- Methods, Method Verification and ValidationDocument14 pagesMethods, Method Verification and Validationjljimenez1969100% (16)
- ORA-LAB.4.13 Record and Data Management (v02)Document11 pagesORA-LAB.4.13 Record and Data Management (v02)Vedang BhagwatNo ratings yet
- Course Outline Laboratory Management and SupervisionDocument3 pagesCourse Outline Laboratory Management and SupervisionNichole SilverioNo ratings yet
- ORA Lab Manual Vol. II Section 5.4.5 Methods-Method Verification and Validation PDFDocument32 pagesORA Lab Manual Vol. II Section 5.4.5 Methods-Method Verification and Validation PDFLaura GuarguatiNo ratings yet
- GLP Good OneDocument14 pagesGLP Good OnesanjeevbhatNo ratings yet
- GLP Guide - EnglishDocument16 pagesGLP Guide - EnglishMohamad IsmailNo ratings yet
- Site Monitoring Plan TemplateDocument5 pagesSite Monitoring Plan TemplaterajuNo ratings yet
- Msapmsup309a r1Document7 pagesMsapmsup309a r1Shamil JamalNo ratings yet
- Doc10-14 App B QSE 2 OrgDocument4 pagesDoc10-14 App B QSE 2 Orgajee doNo ratings yet
- Continuous Improvement: A Corrective and Preventive Action (CAPA) PlanDocument8 pagesContinuous Improvement: A Corrective and Preventive Action (CAPA) PlanEm NiaxNo ratings yet
- SopDocument3 pagesSopmrchilliciousNo ratings yet
- Training ProcedureDocument10 pagesTraining ProcedureMd HossainNo ratings yet
- Competency SOPDocument10 pagesCompetency SOPD Tech Dental Technologies100% (1)
- Sic - 403 Quality Laboratory ManagementDocument20 pagesSic - 403 Quality Laboratory ManagementharrisonNo ratings yet
- Doc10-14 App - Guide For Dev A Qual MGT PlanDocument72 pagesDoc10-14 App - Guide For Dev A Qual MGT PlanS ONo ratings yet
- Duo IndustrialDocument6 pagesDuo IndustrialLeinner José Motta TrujilloNo ratings yet
- Module 5 - Communication, Requisitioning and Reporting: New Era UniversityDocument55 pagesModule 5 - Communication, Requisitioning and Reporting: New Era UniversityAngela PabelloNo ratings yet
- ORA-LAB.5.9 Ensuring The Quality of Test Results (v02)Document17 pagesORA-LAB.5.9 Ensuring The Quality of Test Results (v02)ahmed alghrably100% (1)
- Audit ReportDocument3 pagesAudit Reportmanujacob33No ratings yet
- AUTC - PPM - WI 1 Document ControlDocument7 pagesAUTC - PPM - WI 1 Document ControlPeterNo ratings yet
- ISO 15189 - 2012 Management RequirementsDocument56 pagesISO 15189 - 2012 Management RequirementsAhmed AdemNo ratings yet
- Chapter 2Document14 pagesChapter 2AdityaDhanrajSinghNo ratings yet
- STE-Unit3 (AY 22-23)Document4 pagesSTE-Unit3 (AY 22-23)hamza khanNo ratings yet
- 6 VOL+II+ +5.5.1 EquipLogWI v1.3 UpdatedDocument6 pages6 VOL+II+ +5.5.1 EquipLogWI v1.3 UpdatedPowellAbogadoNo ratings yet
- Oppe Fppe ToolkitDocument71 pagesOppe Fppe ToolkitFaisal Hamdi100% (1)
- Lec 5 (GLP)Document15 pagesLec 5 (GLP)sheikh muhammad mubashirNo ratings yet
- Good Laboratory Practice (GLP) Requirements: An Overview: KeywordsDocument5 pagesGood Laboratory Practice (GLP) Requirements: An Overview: KeywordsMahmoud DomourNo ratings yet
- Role of Quality Assurance ManagerDocument13 pagesRole of Quality Assurance ManagergrtunaNo ratings yet
- Documentation in Pharmaceutical IndustryDocument101 pagesDocumentation in Pharmaceutical Industrygeet55No ratings yet
- Agilent Maritime Seminar FDA-Methods Validations Guidelines PresentationDocument19 pagesAgilent Maritime Seminar FDA-Methods Validations Guidelines PresentationSunil Murkikar (GM - PMI Quality Operations)No ratings yet
- IT SOP TemplateDocument3 pagesIT SOP TemplateMargelatu SemintarNo ratings yet
- Lex MarkDocument1 pageLex MarkMargelatu SemintarNo ratings yet
- Preturi Piese Schimb Imprimante-AficioDocument2 pagesPreturi Piese Schimb Imprimante-AficioMargelatu SemintarNo ratings yet
- NecesarDocument1 pageNecesarMargelatu SemintarNo ratings yet
- ODNS Support SLA SilverDocument2 pagesODNS Support SLA SilverMargelatu SemintarNo ratings yet
- Printer PartsDocument2 pagesPrinter PartsMargelatu SemintarNo ratings yet
- Bowser's HouseDocument1 pageBowser's HouseMargelatu SemintarNo ratings yet
- ControlDocument1 pageControlMargelatu SemintarNo ratings yet
- Bowser's Grey Airships The BeginingDocument2 pagesBowser's Grey Airships The BeginingMargelatu SemintarNo ratings yet
- KV-S3105CSERIES KV-S3085SERIES: High Speed Color ScannerDocument35 pagesKV-S3105CSERIES KV-S3085SERIES: High Speed Color ScannerMargelatu SemintarNo ratings yet
- S3105C Sup 02 f71Document9 pagesS3105C Sup 02 f71Margelatu SemintarNo ratings yet
- S3105C Sup 02 f71Document9 pagesS3105C Sup 02 f71Margelatu SemintarNo ratings yet
- Interface 02Document1 pageInterface 02Margelatu SemintarNo ratings yet
- Mother 01Document1 pageMother 01Margelatu SemintarNo ratings yet
- KV-S3105CSERIES KV-S3085SERIES: High Speed Color ScannerDocument35 pagesKV-S3105CSERIES KV-S3085SERIES: High Speed Color ScannerMargelatu SemintarNo ratings yet
- Lexmark™ X642 Troubleshooting Guide: Solving Printing ProblemsDocument6 pagesLexmark™ X642 Troubleshooting Guide: Solving Printing ProblemsohnospamNo ratings yet
- Epson TMU220Document164 pagesEpson TMU220Margelatu SemintarNo ratings yet
- Parts Change Notice: Model No. KV-S3105C / KV-S3085 SeriesDocument2 pagesParts Change Notice: Model No. KV-S3105C / KV-S3085 SeriesMargelatu SemintarNo ratings yet
- S3105C Sup 02 f71Document9 pagesS3105C Sup 02 f71Margelatu SemintarNo ratings yet
- PCN3105 Km70602124peDocument1 pagePCN3105 Km70602124peMargelatu SemintarNo ratings yet
- PCN3105 Km70602124peDocument1 pagePCN3105 Km70602124peMargelatu SemintarNo ratings yet
- Epson TMU220Document164 pagesEpson TMU220Margelatu SemintarNo ratings yet
- Panasonic KX Fl513 FullDocument266 pagesPanasonic KX Fl513 FullmalexserviceNo ratings yet
- What Is A Printer Driver?Document2 pagesWhat Is A Printer Driver?Margelatu SemintarNo ratings yet
- What Is A Printer Driver?Document2 pagesWhat Is A Printer Driver?Margelatu SemintarNo ratings yet
- Xerox C123 FuserDocument5 pagesXerox C123 FuserVadineanu RamonaNo ratings yet
- Panasonic KX Fl513 FullDocument266 pagesPanasonic KX Fl513 FullmalexserviceNo ratings yet
- PC Canon6317Document74 pagesPC Canon6317Margelatu SemintarNo ratings yet
- Xerox PE16 Service ManualDocument138 pagesXerox PE16 Service ManualMargelatu SemintarNo ratings yet
- FAIS Assignment 1 - Mariam Jabbar PDFDocument4 pagesFAIS Assignment 1 - Mariam Jabbar PDFMariamNo ratings yet
- Practical Accounting 2 Review: Installment SalesDocument22 pagesPractical Accounting 2 Review: Installment SalesJason BautistaNo ratings yet
- Problem 1 4 8Document2 pagesProblem 1 4 8gaziahmad100% (2)
- 18-JSA Dismantling of Batching PlantDocument5 pages18-JSA Dismantling of Batching Plantmohamed.elkomyNo ratings yet
- State of The Game Industry 2021Document29 pagesState of The Game Industry 2021spotNo ratings yet
- FOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherDocument2 pagesFOR Office USE Only: HDFC Life Sb/Ca/Cc/Sb-Nre/Sb-Nro/OtherAnithaNo ratings yet
- Case Study: From Munich To Mohali: QuestionsDocument3 pagesCase Study: From Munich To Mohali: Questionsshika rai100% (1)
- Ericsson Oil Gas Solution BriefDocument7 pagesEricsson Oil Gas Solution BriefTanesan WyotNo ratings yet
- CRIM2 43. Abalos-vs-People-of-the-PhilippinesDocument2 pagesCRIM2 43. Abalos-vs-People-of-the-PhilippinesKirstie Lou Sales100% (1)
- Prajwalit Dalai Dessertation 2022Document81 pagesPrajwalit Dalai Dessertation 2022Praj Walit DalaiNo ratings yet
- Kelvin Lau MWI +RRDocument18 pagesKelvin Lau MWI +RRUniversityJCNo ratings yet
- Contract of SaleDocument4 pagesContract of Salecorvinmihai591No ratings yet
- Labor Laws and Management in The Tourism EstablishmentsDocument6 pagesLabor Laws and Management in The Tourism EstablishmentsLayna AcostaNo ratings yet
- Steps in Production Planning and ControlDocument2 pagesSteps in Production Planning and ControlImran Ali67% (3)
- Engineering Management Masters Thesis TopicsDocument5 pagesEngineering Management Masters Thesis Topicsgbtrjrap100% (2)
- Contract Agreement Form InfrastructureDocument4 pagesContract Agreement Form InfrastructureAnne Lorraine DioknoNo ratings yet
- Rajesh Exports: ExportingDocument8 pagesRajesh Exports: ExportingShreepal ParekhNo ratings yet
- Catalogue: Pool Equipment / Spare PartsDocument123 pagesCatalogue: Pool Equipment / Spare PartsArmudin SukantaNo ratings yet
- English For Business EassayDocument4 pagesEnglish For Business EassayEma ZulkiffliNo ratings yet
- Fixed DepositsDocument1 pageFixed DepositsTiso Blackstar GroupNo ratings yet
- Harbour Club ReportDocument29 pagesHarbour Club ReportEnthusiastic NoobNo ratings yet
- Zero Defects:: Quality Control, Agrees, Commenting That These Programs Typically Do Not Drive The "Use ofDocument4 pagesZero Defects:: Quality Control, Agrees, Commenting That These Programs Typically Do Not Drive The "Use ofAyush SinghNo ratings yet
- Singapore Metal CaseDocument5 pagesSingapore Metal Caseshreyabatra100% (1)
- NPCP Chapter 11 PDFDocument2 pagesNPCP Chapter 11 PDFCristian OmacNo ratings yet
- How To Earn Money Blogging? (Top 10 Ways To Easily Earn $1k+ Per Month)Document34 pagesHow To Earn Money Blogging? (Top 10 Ways To Easily Earn $1k+ Per Month)Raginee Summoogum100% (1)
- Foundation OBDocument35 pagesFoundation OBSushant VermaNo ratings yet
- Chapter 12 - EditedDocument7 pagesChapter 12 - EditedAhmed walidNo ratings yet
- Solicitud Prestamo InglesDocument7 pagesSolicitud Prestamo InglesGrazyna PrzyborowskaNo ratings yet
- Computer Embracement in NigeriaDocument10 pagesComputer Embracement in NigeriaosakingsNo ratings yet
- Scope and LimitationDocument2 pagesScope and LimitationAlexander Cuenza100% (6)