You might also like
- Semi-Detailed Lesson PlanDocument13 pagesSemi-Detailed Lesson PlanElma Ortega Camion100% (1)
- WDSC Intro Sigil Magic PDFDocument30 pagesWDSC Intro Sigil Magic PDFzC6MuNiWNo ratings yet
- Biology Research PaperDocument5 pagesBiology Research Paperapi-240098584No ratings yet
- Food Toxicology FSPT 2 YR. Food Toxicology FSPT 2 YR.: ND NDDocument57 pagesFood Toxicology FSPT 2 YR. Food Toxicology FSPT 2 YR.: ND NDzekariyas kuneNo ratings yet
- 3 PharmacokineticsDocument36 pages3 PharmacokineticsTanvir FahimNo ratings yet
- Biotransformation of Toxins, DrugsDocument5 pagesBiotransformation of Toxins, Drugsirfan khanNo ratings yet
- SAAM-6636-001: Industrial Toxicology - Winter 2019 Class 4: Mechanisms of Toxicology Chapter 3 - Casarett and Doull'SDocument16 pagesSAAM-6636-001: Industrial Toxicology - Winter 2019 Class 4: Mechanisms of Toxicology Chapter 3 - Casarett and Doull'Skriz0812No ratings yet
- Toxicokinetics: To It in The Body". Four Processes Are Involved in ToxicokineticsDocument13 pagesToxicokinetics: To It in The Body". Four Processes Are Involved in ToxicokineticsSayed AlamNo ratings yet
- UNIT 2 - Week (4-5) : Mechanisms of Toxicity & Toxicokinetics Intended Learning Outcomes (ILO)Document8 pagesUNIT 2 - Week (4-5) : Mechanisms of Toxicity & Toxicokinetics Intended Learning Outcomes (ILO)Hannah Jean Lapenid LemorenasNo ratings yet
- Kuliah FarmakologiDocument74 pagesKuliah FarmakologiHanifNo ratings yet
- Drug Absorption MechanismDocument20 pagesDrug Absorption MechanismhabibieNo ratings yet
- Lecture No. 4 (PHARMACOKINETICS - Mechanism of Drug Transport Processes)Document9 pagesLecture No. 4 (PHARMACOKINETICS - Mechanism of Drug Transport Processes)tejasbhukal567No ratings yet
- Toxicokinetics: Toxicokinetics Is Essentially The Study of "How ADocument22 pagesToxicokinetics: Toxicokinetics Is Essentially The Study of "How ARajabMumbeeNo ratings yet
- Significance of ToxicokineticDocument6 pagesSignificance of Toxicokineticlucy2 kasongiNo ratings yet
- PHARMACOKINETICSDocument55 pagesPHARMACOKINETICSnezifzenu2023No ratings yet
- Mechanisms of ToxicityDocument60 pagesMechanisms of ToxicityKhara TeanoTanNo ratings yet
- Ulangkaji Exam MDM DDocument10 pagesUlangkaji Exam MDM DAsyraf RefdinNo ratings yet
- Pharmacokinetics (Absorption)Document5 pagesPharmacokinetics (Absorption)okoroesther123No ratings yet
- GGDocument24 pagesGGManan BhatiaNo ratings yet
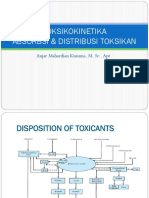
- Disposition of ToxicantsDocument102 pagesDisposition of ToxicantsApoorvi JainNo ratings yet
- DR - Datten Bangun, MSC, SPFK Departemen Framakologi & Terapeutik Fakultas Kedokteran Universitas HKBP Nommensen MedanDocument53 pagesDR - Datten Bangun, MSC, SPFK Departemen Framakologi & Terapeutik Fakultas Kedokteran Universitas HKBP Nommensen MedanSartika NapitupuluNo ratings yet
- Disposition of Toxic Compounds and Its Metabolic Reaction: 03/10/22 Toksikologi Lab. Biokimia Nutrisi 1Document56 pagesDisposition of Toxic Compounds and Its Metabolic Reaction: 03/10/22 Toksikologi Lab. Biokimia Nutrisi 1Franco CibroNo ratings yet
- Ico Kin Etic S& Ico Dyn Am Ics: Professor Dr. Najat A. HasanDocument34 pagesIco Kin Etic S& Ico Dyn Am Ics: Professor Dr. Najat A. HasanMelkamu AyeNo ratings yet
- Pharmacokinetics - DrdhritiDocument83 pagesPharmacokinetics - Drdhritidbrahma100% (1)
- Drug Metabolism ADME PrincipalDocument38 pagesDrug Metabolism ADME PrincipalA. Kumar Soni100% (1)
- Chapter III Pharmacokinetics: Durge Raj GhalanDocument64 pagesChapter III Pharmacokinetics: Durge Raj GhalanDurge Raj Ghalan100% (3)
- Thomas L. Pazdernik, Laszlo Kerecsen-Rapid Review Pharmacology, 3rd Edition-Mosby (2010)Document784 pagesThomas L. Pazdernik, Laszlo Kerecsen-Rapid Review Pharmacology, 3rd Edition-Mosby (2010)dtech2No ratings yet
- PharmacokineticsDocument83 pagesPharmacokineticsdv94gw9zd8No ratings yet
- BCH421. Biotransformation of XenobioticsDocument8 pagesBCH421. Biotransformation of XenobioticsidriscognitoleadsNo ratings yet
- General PharmacologyDocument76 pagesGeneral PharmacologyMiyuru HasarangaNo ratings yet
- Uc PDFDocument6 pagesUc PDFPenNo ratings yet
- Day 7-8 ToxicityDocument100 pagesDay 7-8 ToxicityAlfredoNo ratings yet
- Toksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptDocument51 pagesToksikokinetika Absorbsi & Distribusi Toksikan: Anjar Mahardian Kusuma, M. SC., AptRossy OchieNo ratings yet
- Toxicokinetics: "What The Body Does To The Toxic Material"Document44 pagesToxicokinetics: "What The Body Does To The Toxic Material"Muhammad Shahid BilalNo ratings yet
- Pharmacology 1Document53 pagesPharmacology 1Dawn WRein LegaspiNo ratings yet
- Toxicant Processing in VivoDocument38 pagesToxicant Processing in VivoSilvyNo ratings yet
- ADME Processes - Drug AbsorptionDocument27 pagesADME Processes - Drug AbsorptionDiógenes GramachoNo ratings yet
- BIOPHARMACEUTICSDocument169 pagesBIOPHARMACEUTICSFitria Shizuoka Jiyeon100% (5)
- Pharmaceutical Chemistry I (Phcm571) Lecture 3, Drug Metabolism IDocument42 pagesPharmaceutical Chemistry I (Phcm571) Lecture 3, Drug Metabolism IMirette AshrafNo ratings yet
- Document 2Document9 pagesDocument 2zoha fatimaNo ratings yet
- Biopharmaceutics AbsorptionDocument49 pagesBiopharmaceutics AbsorptionSaul Antonio Montoya SerranoNo ratings yet
- 1a Midterms CompiledDocument105 pages1a Midterms CompiledmasorNo ratings yet
- Module 1 Intro PcolDocument21 pagesModule 1 Intro PcolCygme Neile TacusalmeNo ratings yet
- ASSIGMENT of Environmental Toxicology 12Document8 pagesASSIGMENT of Environmental Toxicology 12naeem attaNo ratings yet
- Absorption of Drug - BiopharmDocument10 pagesAbsorption of Drug - BiopharmTanu nathnaiNo ratings yet
- Resumen FarmacoDocument9 pagesResumen FarmacoMagali DelvalleNo ratings yet
- Notes From Drug MetabolismDocument3 pagesNotes From Drug MetabolismDaniil LyalkoNo ratings yet
- L P - 2 Pharmacokinetics Final-3Document20 pagesL P - 2 Pharmacokinetics Final-3Zakria Al-HadadNo ratings yet
- Drug AbsorptionDocument30 pagesDrug AbsorptionShiva KantNo ratings yet
- Toxicokinetics & ToxicodynamicsDocument31 pagesToxicokinetics & ToxicodynamicscrissNo ratings yet
- XenobioticsDocument2 pagesXenobioticsKarthik SNo ratings yet
- 7 JBS3812Document10 pages7 JBS3812penjurisubhashNo ratings yet
- Pharmacokinetics and Pharmacodynamics - LecturioDocument30 pagesPharmacokinetics and Pharmacodynamics - LecturioAndrea de GuzmanNo ratings yet
- Toxicokinetics & ToxicodynamicsDocument31 pagesToxicokinetics & ToxicodynamicsWahyudin AhmadNo ratings yet
- Topic 5BDocument70 pagesTopic 5BMohd RafiqNo ratings yet
- Chapter 5 DDS Clarion LCDocument15 pagesChapter 5 DDS Clarion LCclyde clarionNo ratings yet
- Pharmacokinetics ProcessDocument11 pagesPharmacokinetics ProcesstitusNo ratings yet
- The Ladmer SystemDocument12 pagesThe Ladmer Systemkriss WongNo ratings yet
- Drug BiotransformationDocument17 pagesDrug Biotransformation4mvqwc9h7kNo ratings yet
- SLP 4Document4 pagesSLP 4RUDOLF YUSON BM20110052No ratings yet
- Xenobiotic MetabolismDocument5 pagesXenobiotic MetabolismErezina Odomero OyegwaNo ratings yet
- A-level Biology Revision: Cheeky Revision ShortcutsFrom EverandA-level Biology Revision: Cheeky Revision ShortcutsRating: 5 out of 5 stars5/5 (5)
- Thyroid DisordersDocument67 pagesThyroid DisordersMA 09No ratings yet
- Seham L7-SchizopherniaDocument62 pagesSeham L7-SchizopherniaMA 09No ratings yet
- Activity IDocument1 pageActivity IMA 09No ratings yet
- Gout and HyperuricemiaDocument41 pagesGout and HyperuricemiaMA 09No ratings yet
- AmlodipineDocument9 pagesAmlodipineMA 09No ratings yet
- Generalized Tonic-Clonic Seizures CaseDocument7 pagesGeneralized Tonic-Clonic Seizures CaseMA 09No ratings yet
- Hypoglycemia (SeminarDocument38 pagesHypoglycemia (SeminarDawitNo ratings yet
- Alingatong Plants?Document3 pagesAlingatong Plants?nancy urrizaNo ratings yet
- D.pharm Syllabus PDFDocument24 pagesD.pharm Syllabus PDFpankaj dagurNo ratings yet
- Radiology Masterclass - Chest Tutorials - Chest Anatomy - Trachea and Main Bronchi-1Document2 pagesRadiology Masterclass - Chest Tutorials - Chest Anatomy - Trachea and Main Bronchi-1kbNo ratings yet
- 2nd Periodical ExamDocument4 pages2nd Periodical ExamLourie Jean Tupaz TelinNo ratings yet
- ProbDocument5 pagesProbMa Christina Miravalles SergioNo ratings yet
- Ins Analysis Bio ActivityDocument11 pagesIns Analysis Bio Activitykosmotrotter7137No ratings yet
- Master Techniques in Orthopaedic Surgery Soft Tissue SurgeryDocument944 pagesMaster Techniques in Orthopaedic Surgery Soft Tissue SurgeryAbotaleb Mohd100% (15)
- Ferrous SulfateDocument3 pagesFerrous Sulfatechinchin ramosNo ratings yet
- Heart Rate ExperimentDocument2 pagesHeart Rate Experimentapi-437098595No ratings yet
- PBL GM 2Document41 pagesPBL GM 2SleepyHead ˋωˊNo ratings yet
- Lecture Notes-Growth Kinetics - Growth PhasesDocument24 pagesLecture Notes-Growth Kinetics - Growth Phasesbioenviron100% (1)
- Neural Signal Processing: ELEC 548 - Fall 2015 Tuesday/Thursday 09:25AM - 10:40AM BRC 284Document31 pagesNeural Signal Processing: ELEC 548 - Fall 2015 Tuesday/Thursday 09:25AM - 10:40AM BRC 284marcaumggNo ratings yet
- NEJM 2014 Fundamentals of Lung AuscultationDocument7 pagesNEJM 2014 Fundamentals of Lung AuscultationFelipe CeaNo ratings yet
- Blood PressureDocument4 pagesBlood PressureWincy SalazarNo ratings yet
- Patient Worksheet - Postpartum 1-PatientDocument1 pagePatient Worksheet - Postpartum 1-PatientJerry G100% (1)
- Workout CalendarDocument2 pagesWorkout CalendarKatie Bonick-ColbreseNo ratings yet
- Nutrition Part Fat-Soluble Vitamin Deficiency: UMFA2053 General Pathology (JAN) Lan Yen MinDocument68 pagesNutrition Part Fat-Soluble Vitamin Deficiency: UMFA2053 General Pathology (JAN) Lan Yen MinAliLeeNo ratings yet
- BIO-207 (1) Homeostasis Lecture NotesDocument10 pagesBIO-207 (1) Homeostasis Lecture NotesJNo ratings yet
- Prana Shama Yoga Training ManualDocument48 pagesPrana Shama Yoga Training Manualvincraig100% (5)
- Principles of Human Physiology 6th Edition Stanfield Test BankDocument35 pagesPrinciples of Human Physiology 6th Edition Stanfield Test Bankpithlessriverp4d6No ratings yet
- Histology - Male Reproductive SystemDocument46 pagesHistology - Male Reproductive SystemKim AcostaNo ratings yet
- UG022524 International GCSE in Human Biology 4HB0 For PrintDocument42 pagesUG022524 International GCSE in Human Biology 4HB0 For PrintHosni ShowikeNo ratings yet
- Kantor Cabang: BANJARMASIN - 1701 FKTP: Kertak Hanyar - 17040601Document72 pagesKantor Cabang: BANJARMASIN - 1701 FKTP: Kertak Hanyar - 17040601Ic-tika Siee ChuabbieNo ratings yet
- Lab 4: Finger Reaction Time To Visual, Auditory and Combined StimulusDocument7 pagesLab 4: Finger Reaction Time To Visual, Auditory and Combined Stimulusapi-318013724No ratings yet
- Sleep Disorders - EnglishDocument42 pagesSleep Disorders - EnglishLevitaSavitry100% (1)
- EndocrineDocument55 pagesEndocrineKolapo SanusiNo ratings yet