You might also like
- Developing Occupation Kits in A Hand Therapy Student Experiential Learning ClinicDocument10 pagesDeveloping Occupation Kits in A Hand Therapy Student Experiential Learning ClinicFranz CalumpitNo ratings yet
- Occupational Therapy and Physiotherapy Benefit The Acute Patient Pathway: A Mixed-Methods StudyDocument12 pagesOccupational Therapy and Physiotherapy Benefit The Acute Patient Pathway: A Mixed-Methods StudyIlvita MayasariNo ratings yet
- Ransby 2020Document10 pagesRansby 2020Franz CalumpitNo ratings yet
- AMPS and Hand FunctionDocument10 pagesAMPS and Hand FunctionJosh Hin ChoiNo ratings yet
- Acceptance and Commitment Therapy in Cancer: Review of Applications and FindingsDocument27 pagesAcceptance and Commitment Therapy in Cancer: Review of Applications and FindingsJuan Alberto GonzálezNo ratings yet
- Work Transitions After Serious Hand Injury: Current Occupational Therapy Practice in A Middle-Income CountryDocument14 pagesWork Transitions After Serious Hand Injury: Current Occupational Therapy Practice in A Middle-Income CountryNataliaNo ratings yet
- Occup Environ Med 2003Document16 pagesOccup Environ Med 2003BM2062119PDPP Pang Kuok WeiNo ratings yet
- تنزيلDocument9 pagesتنزيلrazanyahya440No ratings yet
- A Multicenter Study Into Burnout, Perceived Stress, Job Satisfaction, Coping Strategies and General Health Among Emergency Department Nursing StaffDocument16 pagesA Multicenter Study Into Burnout, Perceived Stress, Job Satisfaction, Coping Strategies and General Health Among Emergency Department Nursing Staffmaria blanca cuencaNo ratings yet
- Literature Review Occupational TherapyDocument5 pagesLiterature Review Occupational Therapyafdtorpqk100% (1)
- Kebutuhan Pasien Paliative Tool Menurut PNPCDocument13 pagesKebutuhan Pasien Paliative Tool Menurut PNPCErika putri widianingtyasNo ratings yet
- Physical Therapy Informed by Acceptance and Commitment Therapy - 2020 - The JoDocument11 pagesPhysical Therapy Informed by Acceptance and Commitment Therapy - 2020 - The JoPriscila CarvalhoNo ratings yet
- 1 s2.0 S2452301116301225 MainDocument10 pages1 s2.0 S2452301116301225 MainNia AnggreniNo ratings yet
- Research Paper Occupational TherapyDocument8 pagesResearch Paper Occupational Therapygz8reqdc100% (1)
- 10.1177 17589983231209678Document11 pages10.1177 17589983231209678NataliaNo ratings yet
- Patient Functional Independence and Occupational Therapist Time-Use in Inpatient Services: Patient Demographic and Clinical CorrelatesDocument10 pagesPatient Functional Independence and Occupational Therapist Time-Use in Inpatient Services: Patient Demographic and Clinical CorrelatesNataliaNo ratings yet
- Participatory Action ResearchDocument9 pagesParticipatory Action ResearchGilbert BaltazarNo ratings yet
- Self-Care 3 Months After Attending Chronic Obstructive Pulmonary Disease Patient Education: A Qualitative Descriptive AnalysisDocument7 pagesSelf-Care 3 Months After Attending Chronic Obstructive Pulmonary Disease Patient Education: A Qualitative Descriptive AnalysisBachtiar M TaUfikNo ratings yet
- Anamnesis 2014Document5 pagesAnamnesis 2014Daniel Araya RochaNo ratings yet
- Artigo SimulaçãoDocument7 pagesArtigo SimulaçãoAntónio PereiraNo ratings yet
- Success or Failure of Chronic Pain Rehabilitation: The Importance of Good Interaction - A Qualitative Study Under Patients and ProfessionalsDocument8 pagesSuccess or Failure of Chronic Pain Rehabilitation: The Importance of Good Interaction - A Qualitative Study Under Patients and ProfessionalsJay JalaliNo ratings yet
- International Emergency Nursing: SciencedirectDocument7 pagesInternational Emergency Nursing: SciencedirectKavin Zank JuniorNo ratings yet
- IdentidadDocument12 pagesIdentidadEdgarsito AyalaNo ratings yet
- Research Papers On Clinical PharmacyDocument6 pagesResearch Papers On Clinical Pharmacyaflbrtdar100% (1)
- Comunidad Salud MentlDocument4 pagesComunidad Salud MentlRafael MezaNo ratings yet
- Aquatic Therapy For Occupational Therapy Education and PracticeDocument123 pagesAquatic Therapy For Occupational Therapy Education and PracticeAURORA BADIALINo ratings yet
- Barriers, Facilitators, and ProposalsDocument11 pagesBarriers, Facilitators, and ProposalsAisha MagarangNo ratings yet
- Samikshya .EditedDocument8 pagesSamikshya .EditedSaru NiraulaNo ratings yet
- Wimolrat IPE HYPERTENSION CARE IN THAILANDDocument68 pagesWimolrat IPE HYPERTENSION CARE IN THAILANDAgeng Patuh PranataNo ratings yet
- Study of Expectations and Satisfaction of General Practi - Tioners (GPS) in Relation To A Physical and Rehabilitation Medicine CenterDocument1 pageStudy of Expectations and Satisfaction of General Practi - Tioners (GPS) in Relation To A Physical and Rehabilitation Medicine CentercarolciveNo ratings yet
- Critical ValuesDocument10 pagesCritical ValuesJorgeNo ratings yet
- An Occupational, Internet-Based Intervention To Prevent Chronicity in Subacute Lower Back Pain: A Randomized Controlled TrialDocument7 pagesAn Occupational, Internet-Based Intervention To Prevent Chronicity in Subacute Lower Back Pain: A Randomized Controlled TrialVictor Hugo Mejìa EscalanteNo ratings yet
- AmputeeDocument7 pagesAmputeeneurodivertoNo ratings yet
- Research Article The Perception of Allied Health Professionals On Occupational TherapyDocument8 pagesResearch Article The Perception of Allied Health Professionals On Occupational TherapyNataliaNo ratings yet
- Cost Consequences StudyDocument4 pagesCost Consequences StudySankita SandalNo ratings yet
- Internationally Indexed Journal Internationally Indexed Journal Internationally Indexed Journal Internationally Indexed JournalDocument8 pagesInternationally Indexed Journal Internationally Indexed Journal Internationally Indexed Journal Internationally Indexed JournalGopi KrishnanNo ratings yet
- Coach, Don't Just TeachDocument17 pagesCoach, Don't Just TeachFabiano HenriqueNo ratings yet
- A New Tool For Assessment of Professional Skills of Occupational Therapy StudentsDocument14 pagesA New Tool For Assessment of Professional Skills of Occupational Therapy Studentsantonio de diaNo ratings yet
- Compliance With Hand Therapy Programs - Therapist and Patients PerceptionsDocument10 pagesCompliance With Hand Therapy Programs - Therapist and Patients PerceptionssammyrasaNo ratings yet
- JMedLife 09 363Document6 pagesJMedLife 09 363Al FatihNo ratings yet
- SR QdashDocument18 pagesSR QdashFrancis MacatangayNo ratings yet
- International Journal of Medical Sciences 2011 8 (5) :397-401 Research Paper Communication Skills Training For Emergency NursesDocument10 pagesInternational Journal of Medical Sciences 2011 8 (5) :397-401 Research Paper Communication Skills Training For Emergency Nursesanon_543702124No ratings yet
- Stroke Article 1Document10 pagesStroke Article 1api-292843843No ratings yet
- Assessment of Stress Coping and PresenteDocument10 pagesAssessment of Stress Coping and PresenteMadalina SoldanNo ratings yet
- Studyprotocol Open AccessDocument11 pagesStudyprotocol Open AccessDIMITRANo ratings yet
- Nurse Education Today: Ana M. Grilo, Margarida C. Santos, Joana S. Rita, Ana I. GomesDocument5 pagesNurse Education Today: Ana M. Grilo, Margarida C. Santos, Joana S. Rita, Ana I. GomesShiee Nevhie ParaDinata WapersNo ratings yet
- 1 Paper EmergencyDepartmentPatientProcessFlowDocument6 pages1 Paper EmergencyDepartmentPatientProcessFlowandika fahruroziNo ratings yet
- Evaluation of The Job Satisfaction of The Nursing Staff of The National Hospital of Donka: Case of The Trainee DoctorsDocument6 pagesEvaluation of The Job Satisfaction of The Nursing Staff of The National Hospital of Donka: Case of The Trainee DoctorsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Clinical Reasoning: Linking Theory To Practice and Practice To TheoryDocument14 pagesClinical Reasoning: Linking Theory To Practice and Practice To Theorylumac1087831No ratings yet
- 05 RandallJ-et-al Effect-of-CST JAMA 2013Document11 pages05 RandallJ-et-al Effect-of-CST JAMA 2013Mirabela CretuNo ratings yet
- Literature Review Occupational Therapy and Primary Health CareDocument6 pagesLiterature Review Occupational Therapy and Primary Health Carec5r08vf7No ratings yet
- Experiencing Patient Experience SurveyDocument10 pagesExperiencing Patient Experience Surveyrisa setiaNo ratings yet
- Occupational Therapy 3D PrintingDocument12 pagesOccupational Therapy 3D PrintingRainNo ratings yet
- Effective Healthcare Worker-Patient Communication in Hong Kong Accident and Emergency DepartmentsDocument15 pagesEffective Healthcare Worker-Patient Communication in Hong Kong Accident and Emergency Departmentssel selNo ratings yet
- Developing Delirium Best Practice: A Systematic Review of Education Interventions For Healthcare Professionals Working in Inpatient SettingsDocument32 pagesDeveloping Delirium Best Practice: A Systematic Review of Education Interventions For Healthcare Professionals Working in Inpatient Settingslinxiaofei2019No ratings yet
- How Much Does The Dallas Pain Questionnaire Score Have To Improve To Indicate That Patients With Chronic Low Back Pain Feel Better or Well?Document6 pagesHow Much Does The Dallas Pain Questionnaire Score Have To Improve To Indicate That Patients With Chronic Low Back Pain Feel Better or Well?mitchNo ratings yet
- Interprofessional Collaboration in Primary Health CareDocument12 pagesInterprofessional Collaboration in Primary Health Caremira maryanilaifaNo ratings yet
- 1 Paper EmergencyDepartmentPatientProcessFlowDocument6 pages1 Paper EmergencyDepartmentPatientProcessFlowYey PahmateeNo ratings yet
- Hand Surgery Patient Satisfaction After SurgeryDocument20 pagesHand Surgery Patient Satisfaction After SurgeryManuel SanchezNo ratings yet
- Fast Facts: Dermatological Nursing: A practical guide on career pathwaysFrom EverandFast Facts: Dermatological Nursing: A practical guide on career pathwaysNo ratings yet
- Medication Errors PaperDocument6 pagesMedication Errors Paperapi-487459879No ratings yet
- DHCS Handbook EnglishDocument33 pagesDHCS Handbook EnglishprabhaNo ratings yet
- Werner CH 4Document99 pagesWerner CH 4Osama NasimNo ratings yet
- Lecture3 PDFDocument3 pagesLecture3 PDFKumar RajeshNo ratings yet
- ØÁ L Nu T Uz È: Federal Negarit GazetaDocument17 pagesØÁ L Nu T Uz È: Federal Negarit GazetaHabtamu TadesseNo ratings yet
- Indian Income Tax Return Acknowledgement 2021-22: Assessment YearDocument1 pageIndian Income Tax Return Acknowledgement 2021-22: Assessment YearPrateek GuptaNo ratings yet
- 1028 - Temporal LobeDocument19 pages1028 - Temporal LobeEdward LinNo ratings yet
- Gray Hat Hacking The Ethical Hackers Handbook Sixth Edition Daniel Regalado Full ChapterDocument51 pagesGray Hat Hacking The Ethical Hackers Handbook Sixth Edition Daniel Regalado Full Chaptereugene.poremski145100% (5)
- Science Direct Photoluminescence From Colloidal Silver NanoparticlesDocument6 pagesScience Direct Photoluminescence From Colloidal Silver NanoparticlesYu Shu HearnNo ratings yet
- 1VDD006144 GB SafeRing - Plus - Air - April 2016Document74 pages1VDD006144 GB SafeRing - Plus - Air - April 2016Gary FortuinNo ratings yet
- UntitledDocument37 pagesUntitledDevanathan ChinnasamyNo ratings yet
- ASR-3000 Service ManualDocument26 pagesASR-3000 Service ManualYoussry Elsayed MohamedNo ratings yet
- BV Rules PtE Ch3 Sec2 AUT-CCSDocument2 pagesBV Rules PtE Ch3 Sec2 AUT-CCSJon LopezNo ratings yet
- I. Demographic Profile: Treatments/MedicationDocument4 pagesI. Demographic Profile: Treatments/MedicationGrace MellaineNo ratings yet
- AC Rectifier Bulk Capacitor Selection With Analysis+SPICE (Walker) PDFDocument5 pagesAC Rectifier Bulk Capacitor Selection With Analysis+SPICE (Walker) PDFjazbo8No ratings yet
- TL280LE (R) : Internet and LTE/HSPA Dual-Path Alarm CommunicatorDocument60 pagesTL280LE (R) : Internet and LTE/HSPA Dual-Path Alarm Communicatorcchung147554No ratings yet
- Severe Acute Malnutrition: Facility-Based Management of Children WithDocument176 pagesSevere Acute Malnutrition: Facility-Based Management of Children WithNikitha RafeekNo ratings yet
- Pulmonary SurgeryDocument18 pagesPulmonary SurgeryShy PatelNo ratings yet
- Molusco ContagiosoDocument12 pagesMolusco ContagiosoEduardo Medeiros Tabosa PinheiroNo ratings yet
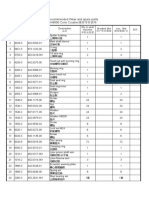
- Recommended Wear and spare parts H8800 Cone Crusher推荐零件清单Document3 pagesRecommended Wear and spare parts H8800 Cone Crusher推荐零件清单Lmf DanielNo ratings yet
- Mounting Solutions: Multi-Parameter Patient MonitorDocument2 pagesMounting Solutions: Multi-Parameter Patient Monitor杨敏杰No ratings yet
- Types of Tissue - Nervous TissueDocument3 pagesTypes of Tissue - Nervous TissueFaye AquinoNo ratings yet
- BECG Assignment 5th SeptDocument4 pagesBECG Assignment 5th Septpragya dhancholiaNo ratings yet
- 0906 0909 Lab Accreditation I II (Class Notes) (Vanessa 2022)Document82 pages0906 0909 Lab Accreditation I II (Class Notes) (Vanessa 2022)Vienne Yuen Wing YanNo ratings yet
- Separation Agreement Template 04Document5 pagesSeparation Agreement Template 04rob De MayoNo ratings yet
- CytoskeletonDocument4 pagesCytoskeletonharshika tembhurneNo ratings yet
- The Solubility of DrugsDocument38 pagesThe Solubility of Drugsmoney in the bankNo ratings yet
- 8 Oraciones - Cook - InglesDocument2 pages8 Oraciones - Cook - InglesÓliver MontenegroNo ratings yet
- STC Man Power Supply ServicesDocument12 pagesSTC Man Power Supply ServicesSTC OmanNo ratings yet
- Hirschman 1982 Hedonic Consumption Emerging Concepts Methods and Propositio PDFDocument11 pagesHirschman 1982 Hedonic Consumption Emerging Concepts Methods and Propositio PDFMichael Alexandre Ramos BravoNo ratings yet