You might also like
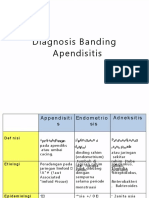
- PDF Diagnosis Banding AppDocument5 pagesPDF Diagnosis Banding AppPutri Maya AgustriaNo ratings yet
- Thyroid Cancer Diagnosis and ManagementDocument45 pagesThyroid Cancer Diagnosis and Managementapi-3704562100% (1)
- Lung Ca Case StudyDocument3 pagesLung Ca Case StudyJoseNo ratings yet
- 3.1.5.3 Patologi Anatomi Sistem Urogenital Dan PayudaraDocument70 pages3.1.5.3 Patologi Anatomi Sistem Urogenital Dan PayudaraaiysahmirzaNo ratings yet
- Malignant Diseases of The OvaryDocument64 pagesMalignant Diseases of The OvaryGÖKSU SAYGILINo ratings yet
- OvarDocument52 pagesOvarAndrei BuruianăNo ratings yet
- Pande Komang Gerry Paramesta: Decision Making in Bowel Obstruction: A Review byDocument32 pagesPande Komang Gerry Paramesta: Decision Making in Bowel Obstruction: A Review byanon_550250832100% (1)
- Ovarian CADocument62 pagesOvarian CAeza floresNo ratings yet
- Gyn Onc Case: Mircea CocaDocument6 pagesGyn Onc Case: Mircea CocacmirceaNo ratings yet
- Surgical Posting - Testicular TumoursDocument16 pagesSurgical Posting - Testicular TumoursDiyana ZatyNo ratings yet
- Peyraud 2020Document12 pagesPeyraud 2020Paulo de TarcioNo ratings yet
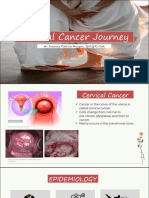
- Cervical CancerDocument50 pagesCervical CancerMohmmadRjab SederNo ratings yet
- Benign Liver Tumours EASL CPGDocument34 pagesBenign Liver Tumours EASL CPGhoneyworksNo ratings yet
- Cellular AberrationDocument6 pagesCellular AberrationALYSSANo ratings yet
- Renal CancerDocument13 pagesRenal CancerMahesh RathnayakeNo ratings yet
- Abdominal & GU TraumaDocument81 pagesAbdominal & GU TraumaAshraf HusseinNo ratings yet
- Cancer Pathophysiology Nursing NotesDocument8 pagesCancer Pathophysiology Nursing Notesgrad_nurse_2015100% (2)
- Case Presentation 1Document4 pagesCase Presentation 1api-448765847No ratings yet
- Ewing's Sarcoma: by DR - Harshavardhan ChandaneDocument49 pagesEwing's Sarcoma: by DR - Harshavardhan Chandaneharsh.chandaneNo ratings yet
- Materi DR SuzanDocument26 pagesMateri DR SuzanputrihealthirezaNo ratings yet
- GenitoUrinary CancerDocument5 pagesGenitoUrinary CancerRaman KumarNo ratings yet
- CANCERDocument45 pagesCANCEREj RamosNo ratings yet
- (Surg2) 5.4 Urology Part 3Document23 pages(Surg2) 5.4 Urology Part 3AlloiBialbaNo ratings yet
- PDF Cancer Introduction Control Amp ScreeningDocument33 pagesPDF Cancer Introduction Control Amp ScreeningFlorencia GuerraNo ratings yet
- With Examples, What Are The Properties of An Ideal Tumour Marker?Document43 pagesWith Examples, What Are The Properties of An Ideal Tumour Marker?Wan HafizNo ratings yet
- Thyroid CancerDocument38 pagesThyroid CancerNinikNo ratings yet
- ESMO Relapsed Ovarian CaDocument9 pagesESMO Relapsed Ovarian CasusdoctorNo ratings yet
- Ovarian CA 450918 SHDocument52 pagesOvarian CA 450918 SH180045No ratings yet
- Squamous Cell CarcinomaDocument53 pagesSquamous Cell CarcinomaWacky BlankNo ratings yet
- CancerDocument51 pagesCancerapi-385676067% (3)
- Oncology Lec1Document42 pagesOncology Lec1Kunal BhamareNo ratings yet
- Approach To Thyroid MalignancyDocument9 pagesApproach To Thyroid MalignancyHuda Al-AnabrNo ratings yet
- Testes and ScrotumDocument31 pagesTestes and ScrotumSarah Sy-SantosNo ratings yet
- A2 Prostate Ca - AinDocument4 pagesA2 Prostate Ca - AinNur Liyana Ahmad ZakiNo ratings yet
- Case Study Stomach CancerDocument2 pagesCase Study Stomach CancerJoseNo ratings yet
- (GYNE) Neoplastic Diseases of The Ovary-Dr. Dueñas (Parbs)Document10 pages(GYNE) Neoplastic Diseases of The Ovary-Dr. Dueñas (Parbs)adrian kristopher dela cruzNo ratings yet
- Oncology Toribio Augene SecFDocument9 pagesOncology Toribio Augene SecFAugene ToribioNo ratings yet
- Cervical CaDocument43 pagesCervical Caraul sinatoNo ratings yet
- Treatment of Parotid CancersDocument15 pagesTreatment of Parotid CancersSudhir NairNo ratings yet
- Squamous Cell CarcinomaDocument53 pagesSquamous Cell CarcinomaWacky BlankNo ratings yet
- Cervical CancerDocument36 pagesCervical CancerPro fatherNo ratings yet
- Renal Cell CarcinomaDocument3 pagesRenal Cell CarcinomaVon HippoNo ratings yet
- Thyroid CancerDocument38 pagesThyroid CancersarahNo ratings yet
- Pancreas CancerDocument66 pagesPancreas CancerPaulo Henrique Haß FilhoNo ratings yet
- EAU Pocket On Primary Urethral Carcinoma 2022Document9 pagesEAU Pocket On Primary Urethral Carcinoma 2022AlbalushiNo ratings yet
- Esophageal CADocument56 pagesEsophageal CAEdwin OkonNo ratings yet
- Module Cellular AberrationDocument43 pagesModule Cellular AberrationJojo JustoNo ratings yet
- NbmeDocument5 pagesNbmeRahul ShuklaNo ratings yet
- The Genetics of CancerDocument36 pagesThe Genetics of CancerRAFIEYANNo ratings yet
- Approach To Endometrial BiopsyDocument62 pagesApproach To Endometrial BiopsySumiya JssalbNo ratings yet
- Texf Eu 2011 00600366 2Document8 pagesTexf Eu 2011 00600366 2JS57No ratings yet
- Vulva CancerDocument2 pagesVulva CancerLim Hui ZhuanNo ratings yet
- Germ Cell TumoursDocument32 pagesGerm Cell Tumoursapi-3705046No ratings yet
- Oncology 1Document60 pagesOncology 1LUISENRIQUENo ratings yet
- Tumors of TestisDocument25 pagesTumors of TestisYazeed AsrawiNo ratings yet
- Endometrial Cancer OGRM 2019Document8 pagesEndometrial Cancer OGRM 2019MiraNo ratings yet
- Surgical OncologyDocument10 pagesSurgical Oncologysofea zamriNo ratings yet
- Rectal Cancer With Synchronous Tonsillar Metastasis: A Case Report and Literature ReviewDocument3 pagesRectal Cancer With Synchronous Tonsillar Metastasis: A Case Report and Literature ReviewKresna ArdinugrahaNo ratings yet
- 3 - NCM112Document6 pages3 - NCM112Edthel IniegoNo ratings yet
- OC SasaDocument32 pagesOC SasamupkoNo ratings yet
- 100 Games IntructionDocument15 pages100 Games IntructionmupkoNo ratings yet
- Word Napredne TehnikeDocument71 pagesWord Napredne TehnikedjelleNo ratings yet
- Praxis Monitoring Report For MarchDocument4 pagesPraxis Monitoring Report For MarchmupkoNo ratings yet
- Praxis Protection Monitoring Report July 2019 PDFDocument7 pagesPraxis Protection Monitoring Report July 2019 PDFmupkoNo ratings yet
- Petmax Catalogue April 2019 Zs2Document1 pagePetmax Catalogue April 2019 Zs2mupkoNo ratings yet
- Bladder Cancer 1Document31 pagesBladder Cancer 1Anas HamadNo ratings yet
- A Good Thesis Statement For A Cancer Research PaperDocument6 pagesA Good Thesis Statement For A Cancer Research PaperNeedSomeoneWriteMyPaperCanada100% (1)
- 21st Century DiseasesDocument8 pages21st Century DiseasesPapanaga ArinaNo ratings yet
- The Crete Declaration On Oral Cancer Prevention 2005 - A Commitment To ActionDocument1 pageThe Crete Declaration On Oral Cancer Prevention 2005 - A Commitment To ActionMario LanzaNo ratings yet
- Bassez 2021Document40 pagesBassez 2021Juan PachecoNo ratings yet
- CT and MRI of Abdomen and PelvicDocument1,691 pagesCT and MRI of Abdomen and PelvicĐức Khang NguyễnNo ratings yet
- WEEK 4 - MEDSURG - Cellular AberrationDocument10 pagesWEEK 4 - MEDSURG - Cellular AberrationLeslie CruzNo ratings yet
- The Pathological Diagnosis of Epithelial Ovarian Cancer in The NetherlandsDocument4 pagesThe Pathological Diagnosis of Epithelial Ovarian Cancer in The Netherlandssmdj1975No ratings yet
- Incision in Breast Oncoplastic SurgeryDocument26 pagesIncision in Breast Oncoplastic Surgeryccmcshh surgeryNo ratings yet
- Activation of KRAS Promotes The MesenchymalDocument9 pagesActivation of KRAS Promotes The MesenchymalDayan Andrea Carrión EstradaNo ratings yet
- Aldape 2015Document20 pagesAldape 2015BG BBNo ratings yet
- Anticancer Pharmacology: D. Lyrawati, Apt. MS., PHDDocument52 pagesAnticancer Pharmacology: D. Lyrawati, Apt. MS., PHDSiti Jannatul HusnahNo ratings yet
- Glioma Difuso de La Linea MediaDocument9 pagesGlioma Difuso de La Linea MediaJOHN LOPERANo ratings yet
- Warthins Tumorof Parotid GlandDocument5 pagesWarthins Tumorof Parotid GlandWahyuni NaharuddinNo ratings yet
- Soft Tissue Biopsy Needles - BR - ENDocument20 pagesSoft Tissue Biopsy Needles - BR - ENAgung WibowoNo ratings yet
- Kyle Clanton Brings Colorectal Cancer Awareness To The Catwalk Modeling Blue ShoesDocument3 pagesKyle Clanton Brings Colorectal Cancer Awareness To The Catwalk Modeling Blue ShoesPR.comNo ratings yet
- New Zealand Listener - February 25 2023Document98 pagesNew Zealand Listener - February 25 2023juan carlosNo ratings yet
- Relative ClauseDocument4 pagesRelative ClauseZu Zu KhinNo ratings yet
- Bfco193 Radiotherapy Dose Fractionation Third-edition-head-And-neck 0Document6 pagesBfco193 Radiotherapy Dose Fractionation Third-edition-head-And-neck 0Khumaira SantaNo ratings yet
- Herceptin® Trastuzumab: Albane Brunel, Claire D'avout, Domitille Fernet, Nadia TalebDocument112 pagesHerceptin® Trastuzumab: Albane Brunel, Claire D'avout, Domitille Fernet, Nadia TalebBima AnestyaNo ratings yet
- Paras ProtocolDocument14 pagesParas Protocolparas yadavNo ratings yet
- Macomb County Resource Guide From McLaren HealthDocument13 pagesMacomb County Resource Guide From McLaren HealthWXYZ-TV Channel 7 DetroitNo ratings yet
- PowerPoint - Hereditary Breast and Ovarian CancerDocument43 pagesPowerPoint - Hereditary Breast and Ovarian CancerkeeNo ratings yet
- Bevacizumab-Capecitabina - CA Mama IV ReviewDocument10 pagesBevacizumab-Capecitabina - CA Mama IV ReviewRocio SolervicensNo ratings yet
- Feature Extraction From Dermoscopy Images For An Effective Diagnosis of Melanoma Skin CancerDocument4 pagesFeature Extraction From Dermoscopy Images For An Effective Diagnosis of Melanoma Skin CancerSnehaNo ratings yet
- Epidemiology and Factors Related To The Survival of Metastatic Kidney Cancers: Retrospective Study at The Mohamed VI Center For The Cancer Treatment in Casablanca, MoroccoDocument5 pagesEpidemiology and Factors Related To The Survival of Metastatic Kidney Cancers: Retrospective Study at The Mohamed VI Center For The Cancer Treatment in Casablanca, MoroccoInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- CancerMapleBaking 2Document2 pagesCancerMapleBaking 2Aliona JelescuNo ratings yet
- Oncology Cheat Sheets - 1Document5 pagesOncology Cheat Sheets - 1abdallahmaurice94No ratings yet
- Notes, 1/e: Surgical Incisions, Needle and Suture MaterialsDocument7 pagesNotes, 1/e: Surgical Incisions, Needle and Suture MaterialsvkNo ratings yet
- CARCINOGENESIS CRC Prof RiwantoDocument48 pagesCARCINOGENESIS CRC Prof Riwantoand3sgr3atNo ratings yet