You might also like
- Prevalencia y factores de riesgo del cáncer de vejiga TCCDocument12 pagesPrevalencia y factores de riesgo del cáncer de vejiga TCCpaomarcarreNo ratings yet
- Tumores de Vejiga TCCDocument12 pagesTumores de Vejiga TCCpaomarcarreNo ratings yet
- Renal CarcinomaDocument3 pagesRenal Carcinomalb25No ratings yet
- Common Pediatric Malignancies: Wilms Tumor and NeuroblastomaDocument34 pagesCommon Pediatric Malignancies: Wilms Tumor and NeuroblastomanazymalfikryNo ratings yet
- Tumor UG - Edit 1Document74 pagesTumor UG - Edit 1Krisna Adhitya WilantaraNo ratings yet
- Carcinoma of Renal Pelvis and UreterDocument27 pagesCarcinoma of Renal Pelvis and UreterIsaac MwangiNo ratings yet
- Renal Tumors RCC Renal Cells Carcinoma Renal Adenocarcinoma HypernephromaDocument5 pagesRenal Tumors RCC Renal Cells Carcinoma Renal Adenocarcinoma HypernephromaMohamed Al-zichrawyNo ratings yet
- MR 28 Agustus-1Document7 pagesMR 28 Agustus-1BramaNo ratings yet
- TJW Bladder CancerDocument35 pagesTJW Bladder CancerShariq ShaNo ratings yet
- Urology L 11 RCCDocument19 pagesUrology L 11 RCCAhmad AlrekabyNo ratings yet
- Testicular TumorsDocument6 pagesTesticular Tumorsyoussef.aziz2020No ratings yet
- Glimelius 2013Document8 pagesGlimelius 2013Sofia SimpertigueNo ratings yet
- Renal Parenchymal Tumor ClassificationDocument45 pagesRenal Parenchymal Tumor ClassificationDaniel100% (1)
- 4 Lung MalignanciesDocument2 pages4 Lung MalignanciesLeah DeeNo ratings yet
- Capitanio 2016Document13 pagesCapitanio 2016Posgrado CirugiaNo ratings yet
- ThyroidDocument43 pagesThyroidchowhan04No ratings yet
- Thyroid CancerDocument38 pagesThyroid CancerNinikNo ratings yet
- Cancer de Riñon Rodrigues SheDocument13 pagesCancer de Riñon Rodrigues SheFeRna NdoNo ratings yet
- Kanker Urologi: Budi D Machsoos Div. Hematologi Onkologi Medik Dept. Ilmu Penyakit Dalam FKUB - RSSA MalangDocument32 pagesKanker Urologi: Budi D Machsoos Div. Hematologi Onkologi Medik Dept. Ilmu Penyakit Dalam FKUB - RSSA MalangRakhmiNo ratings yet
- Nodulo TiroideoDocument6 pagesNodulo TiroideoKammiloPalaciosNo ratings yet
- Malignant Liver Tumours OxfordDocument7 pagesMalignant Liver Tumours OxfordJose Tomás MooreNo ratings yet
- Anaesthesia For NephrectomyDocument4 pagesAnaesthesia For Nephrectomy43gasdemNo ratings yet
- Barrett Esophagus Esophageal Cancer: - Grade Dysphagia: Reassessed Within 6 Months (ExcludeDocument2 pagesBarrett Esophagus Esophageal Cancer: - Grade Dysphagia: Reassessed Within 6 Months (ExcludetristineNo ratings yet
- Pielonefritis Kronis: Tujuan PraktikumDocument12 pagesPielonefritis Kronis: Tujuan PraktikumFp Cyninthia KennedyNo ratings yet
- Pancreatitis Aguda - Surgery 2019Document9 pagesPancreatitis Aguda - Surgery 2019Rodrigo MartinezNo ratings yet
- Guide to evaluating hematuria in adultsDocument9 pagesGuide to evaluating hematuria in adultsTheddyon BhenlieNo ratings yet
- Hematuria in AdultsDocument9 pagesHematuria in AdultsTheddyon BhenlieNo ratings yet
- Update On Nasopharyngeal Carcinoma: Ó Humana 2007Document6 pagesUpdate On Nasopharyngeal Carcinoma: Ó Humana 2007Zakia AjaNo ratings yet
- Lo Week 5-1Document13 pagesLo Week 5-1Martien Silviandy SetiawanNo ratings yet
- Venous Thromboembolism in MalignancyDocument3 pagesVenous Thromboembolism in MalignancyAzmi FarhadiNo ratings yet
- Cervical CancerDocument22 pagesCervical CancerfrankNo ratings yet
- 3rd Stage Liver Diseases (2) - HMUDocument31 pages3rd Stage Liver Diseases (2) - HMUjwan ahmedNo ratings yet
- Topic: Reporters: LN1, LN2, LN3 - Date of ReportDocument4 pagesTopic: Reporters: LN1, LN2, LN3 - Date of ReportDesa RefuerzoNo ratings yet
- Oncology Nursing Oncology What Is Cancer? International IncidenceDocument10 pagesOncology Nursing Oncology What Is Cancer? International IncidenceNeweeJoonYowNo ratings yet
- 3.pathology Emrcs2016Document99 pages3.pathology Emrcs2016Farah FarahNo ratings yet
- Urogenital TumorDocument71 pagesUrogenital TumorJanet UngNo ratings yet
- Oncology Nursing CareDocument10 pagesOncology Nursing CareNeweeJoonYow100% (1)
- Childhood Malignancies PP - Copy 2Document46 pagesChildhood Malignancies PP - Copy 2ugonna nwokeNo ratings yet
- Managing Thyroid NodulesDocument58 pagesManaging Thyroid NodulesBrandon ToyNo ratings yet
- Sarcomas of Soft Tissue: Brian A. Van TineDocument50 pagesSarcomas of Soft Tissue: Brian A. Van TineMed MedNo ratings yet
- CholangiocarcinomaDocument7 pagesCholangiocarcinomailovedaneNo ratings yet
- Renal Cell CarcinomaDocument15 pagesRenal Cell Carcinomadger11No ratings yet
- 74 Year Old Woman With Fatigue, Anorexia, and AbdoDocument6 pages74 Year Old Woman With Fatigue, Anorexia, and AbdoRamiro Arraya MierNo ratings yet
- Retro Peritoneal TumorDocument37 pagesRetro Peritoneal TumorHafizur RashidNo ratings yet
- Malignant Renal MassDocument42 pagesMalignant Renal MassZigmund Bryan CortezaNo ratings yet
- Common Childhood Malignancies Radiology Rev CourseDocument35 pagesCommon Childhood Malignancies Radiology Rev CourseIdris Balasa IdrisNo ratings yet
- 6 Giant Cell Arteritis Dan PolireumalgiaDocument8 pages6 Giant Cell Arteritis Dan PolireumalgiaRifqiNo ratings yet
- Management of The Thyroid NoduleDocument8 pagesManagement of The Thyroid NoduleJose Tomás MooreNo ratings yet
- Proceedings From The 2010 Annual Meeting of The American College of Physicians, Wisconsin ChapterDocument15 pagesProceedings From The 2010 Annual Meeting of The American College of Physicians, Wisconsin ChapterHarold FernandezNo ratings yet
- Acute PancreatitisDocument8 pagesAcute PancreatitisSanjaya SenevirathneNo ratings yet
- A Patient With Neck Swelling Moving With SwallowingDocument40 pagesA Patient With Neck Swelling Moving With SwallowingzaminazzNo ratings yet
- GenitoUrinary CancerDocument5 pagesGenitoUrinary CancerRaman KumarNo ratings yet
- Initial Diagnosis and Staging of Pancreatic Cancer Including Main DifferentialsDocument33 pagesInitial Diagnosis and Staging of Pancreatic Cancer Including Main DifferentialsClaudia YalanNo ratings yet
- Genitourinary Cancer GuideDocument31 pagesGenitourinary Cancer GuidefeonajaparNo ratings yet
- DR 180114164748Document43 pagesDR 180114164748Hasnain ToheedNo ratings yet
- Curs 6Document92 pagesCurs 6Adina RomanNo ratings yet
- Review Article: Cancers of The Appendix: Review of The LiteraturesDocument7 pagesReview Article: Cancers of The Appendix: Review of The LiteraturesMaman AhmadNo ratings yet
- Neuroendocrine Tumors: Surgical Evaluation and ManagementFrom EverandNeuroendocrine Tumors: Surgical Evaluation and ManagementJordan M. CloydNo ratings yet
- Urinary Tract Infection (Book) : NephrologyDocument4 pagesUrinary Tract Infection (Book) : NephrologyVon HippoNo ratings yet
- Diagnostic Accuracy of IOTA for Ovarian MassesDocument7 pagesDiagnostic Accuracy of IOTA for Ovarian MassesVon HippoNo ratings yet
- Leptospirosis Policy StatementsDocument6 pagesLeptospirosis Policy StatementsKay RuzNo ratings yet
- Joint and Connective Tissue Disorders: QuestionsDocument11 pagesJoint and Connective Tissue Disorders: QuestionsVon HippoNo ratings yet
- Adnexal Mass in Pregnancy UpToDate PDFDocument21 pagesAdnexal Mass in Pregnancy UpToDate PDFVon HippoNo ratings yet
- KissPrep-Anatomy Physiology PDFDocument1 pageKissPrep-Anatomy Physiology PDFVon HippoNo ratings yet
- Psychiatric 3: Suicide (DR Rosales) June 8, 2011Document4 pagesPsychiatric 3: Suicide (DR Rosales) June 8, 2011Von HippoNo ratings yet
- Suicide, Psychiatric Emergency, Substance Abuse PDFDocument14 pagesSuicide, Psychiatric Emergency, Substance Abuse PDFVon HippoNo ratings yet
- Gyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesDocument8 pagesGyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesVon HippoNo ratings yet
- Psychiatric 3: Suicide (DR Rosales) June 8, 2011Document4 pagesPsychiatric 3: Suicide (DR Rosales) June 8, 2011Von HippoNo ratings yet
- Psychiatric EmergencyDocument3 pagesPsychiatric EmergencyVon HippoNo ratings yet
- Psychopharmacology-Mood StabilizerDocument5 pagesPsychopharmacology-Mood StabilizerVon Hippo100% (1)
- PEDIA2 2.01b Fluids Electrolytes Summary TablesDocument4 pagesPEDIA2 2.01b Fluids Electrolytes Summary TablesVon HippoNo ratings yet
- Psychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersDocument11 pagesPsychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersVon HippoNo ratings yet
- Adult Emergency PDFDocument2 pagesAdult Emergency PDFVon HippoNo ratings yet
- Recalls: 2nd Shifting ExamDocument13 pagesRecalls: 2nd Shifting ExamVon HippoNo ratings yet
- Patho B Prelims RBCDocument12 pagesPatho B Prelims RBCVon HippoNo ratings yet
- Child PsychiatryDocument6 pagesChild PsychiatryVon HippoNo ratings yet
- Motor System: Three Types of Movement Generated by Motor SystemDocument10 pagesMotor System: Three Types of Movement Generated by Motor SystemVon Hippo100% (1)
- Practice of Medicine GuidelinesDocument27 pagesPractice of Medicine GuidelinesVon HippoNo ratings yet
- CLINPATH Finals ReviewerDocument28 pagesCLINPATH Finals ReviewerVon HippoNo ratings yet
- Brainstem Lesions Trans 2019 PDFDocument8 pagesBrainstem Lesions Trans 2019 PDFVon HippoNo ratings yet
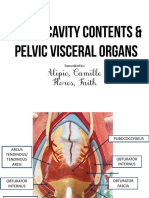
- Alipio, Camille Flores, Faith: Transcribed byDocument7 pagesAlipio, Camille Flores, Faith: Transcribed byVon HippoNo ratings yet
- Ob Gyne PDFDocument27 pagesOb Gyne PDFVon HippoNo ratings yet
- Clinical Scenario: CPT Case 9 Neonatal SepsisDocument15 pagesClinical Scenario: CPT Case 9 Neonatal SepsisVon HippoNo ratings yet
- Vitamins B ComplexDocument4 pagesVitamins B ComplexVon HippoNo ratings yet
- EHS Classification for Incisional Hernia Location and SizeDocument3 pagesEHS Classification for Incisional Hernia Location and SizeVon Hippo100% (1)
- Gold 2019 Pocket Guide Final WmsDocument49 pagesGold 2019 Pocket Guide Final WmsFrensi Ayu PrimantariNo ratings yet
- Fluid and Electrolytes YMDocument8 pagesFluid and Electrolytes YMVon HippoNo ratings yet
- Book: - RecordingDocument8 pagesBook: - RecordingVon HippoNo ratings yet
- Role of Plasmodium Falciparum in The Development Endemic Burkitt 'S Lymphoma (EBL)Document20 pagesRole of Plasmodium Falciparum in The Development Endemic Burkitt 'S Lymphoma (EBL)Aswad ShahzaibNo ratings yet
- COVID-19 Reflection - Pengosro, YzahDocument5 pagesCOVID-19 Reflection - Pengosro, Yzahyzah graceNo ratings yet
- IPM for Okra PestsDocument21 pagesIPM for Okra PestsParry Grewal100% (1)
- Pelvic Inflammatory DiseaseDocument20 pagesPelvic Inflammatory DiseaseDeniela Jamaicy Herbert100% (1)
- Standard Treatment GuidelinesDocument468 pagesStandard Treatment GuidelinesHarshit ChempallilNo ratings yet
- Bone TumorsDocument29 pagesBone TumorsmatameaNo ratings yet
- Patient Monitoring 1Document32 pagesPatient Monitoring 1janvenuNo ratings yet
- Anemia in PregnancyDocument5 pagesAnemia in PregnancySandra GabasNo ratings yet
- Nutrients and Their Functions in Maintaining HealthDocument6 pagesNutrients and Their Functions in Maintaining Healthuma crespoNo ratings yet
- Floracopeia Essential Oil EbookDocument61 pagesFloracopeia Essential Oil EbookOana Algasovschi100% (1)
- Nursing Student Resume GuideDocument16 pagesNursing Student Resume GuideBrainan Aquino100% (2)
- Cardiac PacingDocument9 pagesCardiac PacingmatzoneNo ratings yet
- PPE Course EssentialsDocument25 pagesPPE Course EssentialsUsman DastgirNo ratings yet
- Consent TattooDocument1 pageConsent TattooPetris ArielNo ratings yet
- OASIS - Notification System TRIHDDocument7 pagesOASIS - Notification System TRIHDBimmer ClaessenNo ratings yet
- Fort Bend County Clinical Health TB Annual Progress RPT CY 2016Document16 pagesFort Bend County Clinical Health TB Annual Progress RPT CY 2016BreitbartTexasNo ratings yet
- Sumy KrokDocument0 pagesSumy KrokfaithfavourNo ratings yet
- Journal Club-Stage 4 NB - Presented by TANVIRDocument15 pagesJournal Club-Stage 4 NB - Presented by TANVIRTanvir AhammedNo ratings yet
- Eruption & Shedding MCQDocument22 pagesEruption & Shedding MCQAmr KhattabNo ratings yet
- Antiinflammatory and Antimicrobial Activity of Hexane Extract of Seed of Psoralea Corylifolia LinnDocument9 pagesAntiinflammatory and Antimicrobial Activity of Hexane Extract of Seed of Psoralea Corylifolia Linnvani srcmNo ratings yet
- Mangoes (Mangifera Indica) : By: Jordan RossDocument14 pagesMangoes (Mangifera Indica) : By: Jordan Rossjordanar1005No ratings yet
- Nephrostomy Tubes ToolkitDocument18 pagesNephrostomy Tubes Toolkitmegawati.rscmNo ratings yet
- Definition of Biomedical Model of HealthDocument4 pagesDefinition of Biomedical Model of Healthتالیہ مرادNo ratings yet
- Microbiome Investigation Notebook, Pages 39-45Document7 pagesMicrobiome Investigation Notebook, Pages 39-45Rick WuNo ratings yet
- How To Write ThesisDocument22 pagesHow To Write ThesisKenneth LewisNo ratings yet
- ASmaDocument48 pagesASmaKelvin LaibidaNo ratings yet
- GCE A Level Biology ExamDocument6 pagesGCE A Level Biology ExamjoannetzyNo ratings yet
- PSORIASISDocument9 pagesPSORIASISDianne BernardoNo ratings yet
- Ujian Semester Gasal Kelas Xi IpaDocument38 pagesUjian Semester Gasal Kelas Xi IpaRichard sutantoNo ratings yet
- Quadriceps Muscle Mechanics and Knee Osteoarthritis A 2022 UpdateDocument21 pagesQuadriceps Muscle Mechanics and Knee Osteoarthritis A 2022 UpdateAthenaeum Scientific PublishersNo ratings yet