You might also like
- 3rd - DIAGNOSTIC TESTDocument23 pages3rd - DIAGNOSTIC TESTsrslytrdNo ratings yet
- AmniocentesisDocument15 pagesAmniocentesisGYPSY CAT100% (1)
- Case 1 History & PEDocument3 pagesCase 1 History & PEcbac1990No ratings yet
- Grayscale USG of Placenta AccretaDocument5 pagesGrayscale USG of Placenta AccretaDara Mayang SariNo ratings yet
- Case Obsos SellyDocument24 pagesCase Obsos SellyDwi CahyaNo ratings yet
- NCM 109 SL Lesson 1Document3 pagesNCM 109 SL Lesson 1Martina Medrano100% (1)
- General ObjectivesDocument13 pagesGeneral ObjectiveskevinNo ratings yet
- Pedsinreview 2021005196Document4 pagesPedsinreview 2021005196Claudio MontiNo ratings yet
- History ObgynDocument37 pagesHistory ObgynRana WaelNo ratings yet
- Amniocentesis Cbsebiology4uDocument12 pagesAmniocentesis Cbsebiology4uSharan GopinathNo ratings yet
- Gynac SQ - Docx 1480428309093Document107 pagesGynac SQ - Docx 1480428309093VivekNo ratings yet
- Pediatric and Adolescent Gynecologic Emergencies 2022Document16 pagesPediatric and Adolescent Gynecologic Emergencies 2022Felipe MayorcaNo ratings yet
- Gyne - Torsion of Dermoid CystDocument4 pagesGyne - Torsion of Dermoid CystroshmaeNo ratings yet
- Case Report Session Preterm Rupture of Membrane (PROM) - Ketuban Pecah DiniDocument15 pagesCase Report Session Preterm Rupture of Membrane (PROM) - Ketuban Pecah DiniAnto SaragihNo ratings yet
- Acute Appendicitis in Childhood and Adulthood: MedicineDocument15 pagesAcute Appendicitis in Childhood and Adulthood: MedicineTran DuongNo ratings yet
- Amenorrhea Ovarian TumorsDocument18 pagesAmenorrhea Ovarian TumorsJeremy ShimlerNo ratings yet
- Surgery of The AppendixDocument5 pagesSurgery of The AppendixJoseph De JoyaNo ratings yet
- L 25 Prenatal Diagnosis and Genetic CounselingDocument49 pagesL 25 Prenatal Diagnosis and Genetic Counselingcactus life foreverNo ratings yet
- NCP Tumor Wilms: Ni Nyoman Udiani, S.Kep.,Ns.,M.KepDocument37 pagesNCP Tumor Wilms: Ni Nyoman Udiani, S.Kep.,Ns.,M.KepClaudia NatasyaNo ratings yet
- Cephalopelvic DisproportionDocument6 pagesCephalopelvic DisproportionBaljinder kaurNo ratings yet
- Anatomical SieveDocument4 pagesAnatomical Sieveusmle_social_retardsNo ratings yet
- Ultrasound Scanning of Fetal AnomalyDocument19 pagesUltrasound Scanning of Fetal AnomalyFA Khan0% (1)
- Managment of Abnormal Pap SmearDocument78 pagesManagment of Abnormal Pap SmearMohammad AlrefaiNo ratings yet
- 27 Testicular PainDocument2 pages27 Testicular PainazizaaharisNo ratings yet
- Grand Case Pres - Transverse Vaginal Septum..Document32 pagesGrand Case Pres - Transverse Vaginal Septum..Gio LlanosNo ratings yet
- Askep Tumor Wilms: Ni Nyoman Udiani, S.Kep - Ns.,M.KepDocument36 pagesAskep Tumor Wilms: Ni Nyoman Udiani, S.Kep - Ns.,M.KepRelysa Magdalena IssiNo ratings yet
- Kehamilan Ektopik TergangguDocument31 pagesKehamilan Ektopik TergangguAnonymous al0G68RwjJNo ratings yet
- ABORTION AND ECTOPIC PREGNANCY 2nd LecDocument9 pagesABORTION AND ECTOPIC PREGNANCY 2nd LecDominion OgochukwuNo ratings yet
- Congenital Ovarian Cyst Diagnosisand Perinatal ManagementDocument5 pagesCongenital Ovarian Cyst Diagnosisand Perinatal Managementchirurgie nou-nascutiNo ratings yet
- 378 1682 1 PBDocument6 pages378 1682 1 PBAla RollerNo ratings yet
- p141 PDFDocument7 pagesp141 PDFAde FadilNo ratings yet
- Screening TestsDocument11 pagesScreening TestsMarie Ashley CasiaNo ratings yet
- Approach To Fetal AnomaliesDocument38 pagesApproach To Fetal Anomaliesamq aloqiliNo ratings yet
- Intussusception TransDocument4 pagesIntussusception TransJames Maravillas100% (1)
- Ectopic 2Document48 pagesEctopic 2Norsri WahyuNo ratings yet
- Department of Obstetrics and Gynaecology Faculty of Medicine Sriwijaya University Dr. Moh. Hoesin General Hospital PalembangDocument8 pagesDepartment of Obstetrics and Gynaecology Faculty of Medicine Sriwijaya University Dr. Moh. Hoesin General Hospital PalembangmughanNo ratings yet
- Dolor Abdominal Agudo en El Niño: Universidad Nacional de Trujillo Facultad de MedicinaDocument15 pagesDolor Abdominal Agudo en El Niño: Universidad Nacional de Trujillo Facultad de MedicinaGuille VallejoNo ratings yet
- PIYUSH BIO 01amniocentesis-Cbsebiology4uDocument15 pagesPIYUSH BIO 01amniocentesis-Cbsebiology4uNikhil ChaudhariNo ratings yet
- Prenatal DiagnosisDocument26 pagesPrenatal DiagnosisShandy Suwanto PutraNo ratings yet
- Current Approach To The Diagnosis and Emergency Department Management of Appendicitis in ChildrenDocument6 pagesCurrent Approach To The Diagnosis and Emergency Department Management of Appendicitis in ChildrenmaithamNo ratings yet
- Gray Scale and Doppler Ultrasound in Placenta AccrDocument5 pagesGray Scale and Doppler Ultrasound in Placenta AccrRicky JunaediNo ratings yet
- Case Study On PROMDocument11 pagesCase Study On PROMPatricia Denise TiradoNo ratings yet
- Makalah Case 5 (DR - Akbar)Document81 pagesMakalah Case 5 (DR - Akbar)Malisa Fitri UmarNo ratings yet
- Biochemical Methods ObgDocument25 pagesBiochemical Methods ObgRupali AroraNo ratings yet
- OB Reviewerv2Document9 pagesOB Reviewerv2Andrassy Twinkle AlineaNo ratings yet
- High Risk Pregnancy Assessment and ManagementDocument48 pagesHigh Risk Pregnancy Assessment and ManagementWilfredo PesanteNo ratings yet
- 1 - Abdomen 1Document23 pages1 - Abdomen 1noushad aminNo ratings yet
- PiosalpinxDocument3 pagesPiosalpinxRopiNo ratings yet
- Medical ExamDocument38 pagesMedical Examchikinlam900No ratings yet
- Hernia Uterine Inguinale: An Uncommon Cause of Pelvic Pain in The Adult Female PatientDocument4 pagesHernia Uterine Inguinale: An Uncommon Cause of Pelvic Pain in The Adult Female PatientJeje MoNo ratings yet
- CrackCast Shownotes Episode 93 AppendicitisDocument10 pagesCrackCast Shownotes Episode 93 AppendicitisBharathi ManiyanNo ratings yet
- PWH - NotesDocument140 pagesPWH - NotesjNo ratings yet
- Undescended TestesDocument29 pagesUndescended TestesHillary Bushnell100% (1)
- Transvaginal Sonography Versus Hysteroscopy in Evaluation of Abnormal Uterine BleedingDocument6 pagesTransvaginal Sonography Versus Hysteroscopy in Evaluation of Abnormal Uterine BleedingKoko AgungNo ratings yet
- Abdominal PainDocument11 pagesAbdominal PainSNo ratings yet
- Office Gynecology Dr. SSM Source: PPT + Recordings: Initial Assessment - Communication Medical History and PeDocument74 pagesOffice Gynecology Dr. SSM Source: PPT + Recordings: Initial Assessment - Communication Medical History and PePrecious MedinaNo ratings yet
- 161004acuteaof Gi - MadridDocument73 pages161004acuteaof Gi - MadridMAPACHE 91No ratings yet
- 1 s2.0 S2211568411000234 MainDocument5 pages1 s2.0 S2211568411000234 MainAndres Suarez GutierrezNo ratings yet
- CMC-Preterm LaborDocument11 pagesCMC-Preterm LaborRalph AlbertoNo ratings yet
- Diagnostic Performance of International Ovarian Tumor Analysis IotaDocument7 pagesDiagnostic Performance of International Ovarian Tumor Analysis IotaVon HippoNo ratings yet
- KissPrep-Anatomy Physiology PDFDocument1 pageKissPrep-Anatomy Physiology PDFVon HippoNo ratings yet
- Urinary Tract Infection (Book) : NephrologyDocument4 pagesUrinary Tract Infection (Book) : NephrologyVon HippoNo ratings yet
- Joint and Connective Tissue Disorders: QuestionsDocument11 pagesJoint and Connective Tissue Disorders: QuestionsVon HippoNo ratings yet
- Gyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesDocument8 pagesGyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesVon HippoNo ratings yet
- Psychopharmacology-Mood StabilizerDocument5 pagesPsychopharmacology-Mood StabilizerVon Hippo100% (2)
- Psychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersDocument11 pagesPsychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersVon HippoNo ratings yet
- PEDIA2 2.01b Fluids Electrolytes Summary TablesDocument4 pagesPEDIA2 2.01b Fluids Electrolytes Summary TablesVon HippoNo ratings yet
- Adult Emergency PDFDocument2 pagesAdult Emergency PDFVon HippoNo ratings yet
- Psychiatric EmergencyDocument3 pagesPsychiatric EmergencyVon HippoNo ratings yet
- Compilation of Platings in MicrobiologyDocument6 pagesCompilation of Platings in MicrobiologyVon HippoNo ratings yet
- Psychiatric 3: Suicide (DR Rosales) June 8, 2011Document4 pagesPsychiatric 3: Suicide (DR Rosales) June 8, 2011Von HippoNo ratings yet
- Child PsychiatryDocument6 pagesChild PsychiatryVon HippoNo ratings yet
- Motor System: Three Types of Movement Generated by Motor SystemDocument10 pagesMotor System: Three Types of Movement Generated by Motor SystemVon Hippo100% (1)
- CLINPATH Finals ReviewerDocument28 pagesCLINPATH Finals ReviewerVon HippoNo ratings yet
- Brainstem Lesions Trans 2019 PDFDocument8 pagesBrainstem Lesions Trans 2019 PDFVon HippoNo ratings yet
- Abdominal: Al HerniaDocument3 pagesAbdominal: Al HerniaVon Hippo100% (1)
- Recalls: 2nd Shifting ExamDocument13 pagesRecalls: 2nd Shifting ExamVon HippoNo ratings yet
- 1) Any Medical Student or GraduateDocument27 pages1) Any Medical Student or GraduateVon HippoNo ratings yet
- Clinical Scenario: CPT Case 9 Neonatal SepsisDocument15 pagesClinical Scenario: CPT Case 9 Neonatal SepsisVon HippoNo ratings yet
- Fluid and Electrolytes YMDocument8 pagesFluid and Electrolytes YMVon HippoNo ratings yet
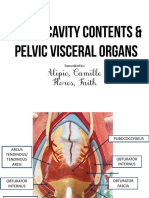
- Alipio, Camille Flores, Faith: Transcribed byDocument7 pagesAlipio, Camille Flores, Faith: Transcribed byVon HippoNo ratings yet
- NEPHRO - Renal Stones PDFDocument3 pagesNEPHRO - Renal Stones PDFVon HippoNo ratings yet
- 2013 Compiled para Exams and Shiftings PDFDocument27 pages2013 Compiled para Exams and Shiftings PDFVon HippoNo ratings yet
- Biochem: Gene Expression Part 2: Recap of Transcription (Part 1 of Lecture)Document14 pagesBiochem: Gene Expression Part 2: Recap of Transcription (Part 1 of Lecture)Von HippoNo ratings yet
- Internal Medicine - Nephrology: Topic: Cystic Kidney Diseases Lecturer: Dra. Myrna NgoDocument3 pagesInternal Medicine - Nephrology: Topic: Cystic Kidney Diseases Lecturer: Dra. Myrna NgoVon HippoNo ratings yet
- Renal Cell CarcinomaDocument3 pagesRenal Cell CarcinomaVon HippoNo ratings yet
- AppenDocument54 pagesAppenmoqtadirNo ratings yet
- Alterations in Nutrition and Gastrointestinal, Metabolism and EndocrineDocument105 pagesAlterations in Nutrition and Gastrointestinal, Metabolism and EndocrineJanmichael FeliscuzoNo ratings yet
- Acute Appendicitis Group CDocument40 pagesAcute Appendicitis Group CHeart TolenadaNo ratings yet
- Rotary Kiln: Doc. No.: 18051-041.1Document14 pagesRotary Kiln: Doc. No.: 18051-041.1mkpqNo ratings yet
- Guidelines For BTP Report PDFDocument14 pagesGuidelines For BTP Report PDFAyush GuptaNo ratings yet
- C. Schematic Tracing: Precipitating Factors: Predisposing FactorsDocument5 pagesC. Schematic Tracing: Precipitating Factors: Predisposing FactorsAngie ArancesNo ratings yet
- Home Remedies For AppendicitisDocument10 pagesHome Remedies For Appendicitispurinaresh85100% (1)
- Why I Gave Up Atheism For Christianity: Michael G. Houts, PHDDocument144 pagesWhy I Gave Up Atheism For Christianity: Michael G. Houts, PHDgrattuckerNo ratings yet
- Granulomatous Appendicitis in A 12-Year-Old Boy: Derya Yayla, Bedriye Nuray Alpman, Yasemin DolekDocument3 pagesGranulomatous Appendicitis in A 12-Year-Old Boy: Derya Yayla, Bedriye Nuray Alpman, Yasemin Dolekansar ahmedNo ratings yet
- Format For Minor Project ReportDocument6 pagesFormat For Minor Project ReportjakharamitNo ratings yet
- APPENDICITISDocument36 pagesAPPENDICITISsjamilmdfauzie100% (4)
- Assignment: Conceptual Design Specification (CDS)Document8 pagesAssignment: Conceptual Design Specification (CDS)Jonathan LeungNo ratings yet
- DR - Krishna Kumar MallickDocument52 pagesDR - Krishna Kumar MallickShiva KumaranNo ratings yet
- Acute Appendicitis and PeritonitisDocument8 pagesAcute Appendicitis and PeritonitisYosuaNo ratings yet
- Appendix and Cecum!Document13 pagesAppendix and Cecum!SilvanaPutriNo ratings yet
- Mucinous Cystadenoma of The AppendixDocument3 pagesMucinous Cystadenoma of The AppendixKriti KumariNo ratings yet
- Use of Appendices 1-9 and 1-10 of ASME Section VIII Division 1Document3 pagesUse of Appendices 1-9 and 1-10 of ASME Section VIII Division 1SachinNo ratings yet
- Project Report FormatDocument7 pagesProject Report FormatRaunaq KaliaNo ratings yet
- Reading Comprehension Task Number 1 Human Body Parts and OrgansDocument5 pagesReading Comprehension Task Number 1 Human Body Parts and OrgansAlexa VelezNo ratings yet
- AppendicitisDocument1 pageAppendicitisMary GiuntiniNo ratings yet
- The Sequence in Which The Project Report Material Should Be Arranged and Bound Should Be As FollowsDocument18 pagesThe Sequence in Which The Project Report Material Should Be Arranged and Bound Should Be As FollowsPraveen KumarNo ratings yet
- Unit Ix: Nursing Management of Patients With Gi Disorders: Topic: AppendicitisDocument16 pagesUnit Ix: Nursing Management of Patients With Gi Disorders: Topic: Appendicitisayushi rainaNo ratings yet
- AppendicitisDocument11 pagesAppendicitisbobtagubaNo ratings yet
- Digestive System: A. Def'nDocument14 pagesDigestive System: A. Def'nrahul_onlyoneNo ratings yet
- Test 7: Appendicitis Definition and FactsDocument21 pagesTest 7: Appendicitis Definition and FactsRuhi RuhiNo ratings yet
- Brmedj03162 0029 PDFDocument3 pagesBrmedj03162 0029 PDFkeyla_shineeeNo ratings yet
- Approach To Acute AbdomenDocument50 pagesApproach To Acute AbdomenAndie ArrNo ratings yet
- Case Study AppendectomyDocument40 pagesCase Study AppendectomyArmin Joseph Pepito0% (1)
- Referat AppendicitisDocument28 pagesReferat AppendicitisFerio Joelian ChandraNo ratings yet
- Identifying Child Abuse ChecklistDocument6 pagesIdentifying Child Abuse Checklistdavidhoracio100% (1)