You might also like
- BIOCHEM - 2S08 - Fluids and Electrolytes - SEC F 2021Document7 pagesBIOCHEM - 2S08 - Fluids and Electrolytes - SEC F 2021Ronak UpadhyayNo ratings yet
- Fluids: ElectrolytesDocument56 pagesFluids: ElectrolytesZee Zang100% (1)
- Water-pH-Electrolytes EDITED!!! PDFDocument109 pagesWater-pH-Electrolytes EDITED!!! PDFKate Lynne CamonayanNo ratings yet
- BODY Weight 100%: Balance/Imbalances & TherapyDocument11 pagesBODY Weight 100%: Balance/Imbalances & TherapyVictoria Castillo TamayoNo ratings yet
- Lec 4Document32 pagesLec 4bosco kiuriaNo ratings yet
- Kompartemen Cairan TubuhDocument27 pagesKompartemen Cairan Tubuhdalang leriNo ratings yet
- Dasar - Dasar Terapi: Cairan Dan ElektrolitDocument60 pagesDasar - Dasar Terapi: Cairan Dan ElektrolitdedeNo ratings yet
- Fluid and Electrolytes (PDF File) : A. Body FluidsDocument5 pagesFluid and Electrolytes (PDF File) : A. Body FluidsLegendX100% (3)
- Fisiologi Cairan MikDocument18 pagesFisiologi Cairan MikRezky Prilya WidyastutiNo ratings yet
- Terapi Cairain Dan ElektrolitDocument39 pagesTerapi Cairain Dan ElektrolityulyaNo ratings yet
- Management Terapi CairanDocument60 pagesManagement Terapi CairanHayat Hamzah DawiNo ratings yet
- FluidelectrolytebalanceDocument87 pagesFluidelectrolytebalancePavi MuruganathanNo ratings yet
- Body FluidDocument10 pagesBody FluidNwaoha Chibuzor AnthonyNo ratings yet
- Fisiologi Sel Dan Cairan Tubuh: M.Ihwan KusumaDocument20 pagesFisiologi Sel Dan Cairan Tubuh: M.Ihwan KusumaHenny AprianiNo ratings yet
- Unit 1-B5Document28 pagesUnit 1-B5Jan Marsha Marie DomiquelNo ratings yet
- Water and LifeDocument46 pagesWater and Lifelethigialinhlop11a4No ratings yet
- FluidDocument31 pagesFluidZainab BasimNo ratings yet
- Fluids Electrolytes - Acid-Base BalanceDocument11 pagesFluids Electrolytes - Acid-Base BalanceJhosita Flora Laroco100% (1)
- Body Fluids Hbc202-Lecture Notes-1Document9 pagesBody Fluids Hbc202-Lecture Notes-1Shreya AnandNo ratings yet
- Management Terapi CairanDocument60 pagesManagement Terapi Cairanpeter singalNo ratings yet
- Micronutrients: Water & ElectrolytesDocument2 pagesMicronutrients: Water & ElectrolytesRANDY ERNEST GESTOSANINo ratings yet
- Intravenous Fluids: Composition & UsesDocument41 pagesIntravenous Fluids: Composition & UsesFathima BanuzNo ratings yet
- Electrolytes Water Balance PH Balance Trace MetalsDocument21 pagesElectrolytes Water Balance PH Balance Trace MetalsJohn Kevin Carl SaligumbaNo ratings yet
- Body FluidsDocument44 pagesBody FluidsTriza JeremiahNo ratings yet
- Fluid and Electrolytes BalanceDocument29 pagesFluid and Electrolytes BalanceHachi Nini Shop IINo ratings yet
- Water and Sodium 2024 PDFDocument61 pagesWater and Sodium 2024 PDFMpho MosehlaNo ratings yet
- Lecture7 PDFDocument36 pagesLecture7 PDFDr. Amrendra JhaNo ratings yet
- Lecture 5 Fluid and ElectrolyteDocument23 pagesLecture 5 Fluid and ElectrolyteBanzaiNo ratings yet
- NCM112 MS 1 Week 1Document11 pagesNCM112 MS 1 Week 1Lerry Claire LimosNo ratings yet
- F&E For Elderly - ModuleDocument163 pagesF&E For Elderly - ModuleArihk NiladaNo ratings yet
- Blood Physiology IIDocument63 pagesBlood Physiology IIelmaNo ratings yet
- Female Reproductive System DrugsDocument11 pagesFemale Reproductive System DrugsBEN-SHARIEF ASULANo ratings yet
- Fluid & Electrolyte BalanceDocument4 pagesFluid & Electrolyte BalanceVia Kristel ZapantaNo ratings yet
- Body Fluid: Presented BY DR (MRS) Okorie PDocument56 pagesBody Fluid: Presented BY DR (MRS) Okorie PKELECHI ELEJENo ratings yet
- Fluids & ElectrolytesDocument18 pagesFluids & ElectrolytesBiway RegalaNo ratings yet
- Molecules Fantastic PDFDocument26 pagesMolecules Fantastic PDFBasma MalashNo ratings yet
- Renal Physio #1 - Fluid and Electrolyte Notes (Dr. Nobleza)Document3 pagesRenal Physio #1 - Fluid and Electrolyte Notes (Dr. Nobleza)Hannah Grace Protasio LumongsodNo ratings yet
- Terapi Cairan Pada AnakDocument48 pagesTerapi Cairan Pada AnakAstri Novia RizqiNo ratings yet
- Body Fluid CompartmenBDSDocument17 pagesBody Fluid CompartmenBDSHimani JhaNo ratings yet
- Water and ElectrolytesDocument16 pagesWater and Electrolytesedunation024No ratings yet
- Body Fluid Compartment SlidesDocument18 pagesBody Fluid Compartment SlidesAkanbi FavourNo ratings yet
- Fluid and Electrolyte MGT in SurgeryDocument40 pagesFluid and Electrolyte MGT in SurgeryJohn AgamahNo ratings yet
- Intracellular Fluid (ICF) Compartment Extracellular Fluid (ECF) CompartmentDocument7 pagesIntracellular Fluid (ICF) Compartment Extracellular Fluid (ECF) CompartmentBianca Louise Chan LimNo ratings yet
- PHARMACOLOGYDocument19 pagesPHARMACOLOGYKiela Therese LabroNo ratings yet
- Fe ConceptDocument177 pagesFe ConceptIvan MaximusNo ratings yet
- 3.14 Chapter 3 Water and Electrolytes Balance and ImblanceDocument140 pages3.14 Chapter 3 Water and Electrolytes Balance and ImblanceShourav SarkarNo ratings yet
- Lec. 3 - Fluid and ElectrolyteDocument16 pagesLec. 3 - Fluid and Electrolyteمجيب سلطانNo ratings yet
- Fluids & Electrolytes: Nio Cruzada Noveno, RN, MAN, MSNDocument66 pagesFluids & Electrolytes: Nio Cruzada Noveno, RN, MAN, MSNapi-19824701No ratings yet
- Fluid and ElectrolytesDocument21 pagesFluid and ElectrolytesMeryl RamosNo ratings yet
- TutorialDocument29 pagesTutorialVilza maharaniNo ratings yet
- Fluids and Electrolytes: 2. Interstitial SpaceDocument13 pagesFluids and Electrolytes: 2. Interstitial Spacehahahahaaaaaaa100% (1)
- Boiler Feed Water ConditioningDocument88 pagesBoiler Feed Water ConditioningGNo ratings yet
- Fluid ElectrolytesDocument39 pagesFluid ElectrolytesLaila alturaifiNo ratings yet
- 2.1 2.2 Metabolism+and+Water 2021 Science 10 IBDocument20 pages2.1 2.2 Metabolism+and+Water 2021 Science 10 IBNexExplosiveNo ratings yet
- DR - Sabah Noori 1Document26 pagesDR - Sabah Noori 1Mighty AbodyNo ratings yet
- Blood and Body Fluids-Nurs-EbaaDocument56 pagesBlood and Body Fluids-Nurs-EbaaEbaa Moh'd ZayadnehNo ratings yet
- Biological Molecules AS Bio 2022Document20 pagesBiological Molecules AS Bio 2022MrTechnomasterNo ratings yet
- Gangguan Keseimbangan Cairan Dan ElektrolitDocument45 pagesGangguan Keseimbangan Cairan Dan Elektrolitmulyo utomoNo ratings yet
- 1 Basic Chemicals in CellDocument13 pages1 Basic Chemicals in CellabbiechongNo ratings yet
- Gyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesDocument8 pagesGyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesVon HippoNo ratings yet
- Diagnostic Performance of International Ovarian Tumor Analysis IotaDocument7 pagesDiagnostic Performance of International Ovarian Tumor Analysis IotaVon HippoNo ratings yet
- Joint and Connective Tissue Disorders: QuestionsDocument11 pagesJoint and Connective Tissue Disorders: QuestionsVon HippoNo ratings yet
- Psychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersDocument11 pagesPsychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersVon HippoNo ratings yet
- Psychiatric 3: Suicide (DR Rosales) June 8, 2011Document4 pagesPsychiatric 3: Suicide (DR Rosales) June 8, 2011Von HippoNo ratings yet
- Urinary Tract Infection (Book) : NephrologyDocument4 pagesUrinary Tract Infection (Book) : NephrologyVon HippoNo ratings yet
- KissPrep-Anatomy Physiology PDFDocument1 pageKissPrep-Anatomy Physiology PDFVon HippoNo ratings yet
- PEDIA2 2.01b Fluids Electrolytes Summary TablesDocument4 pagesPEDIA2 2.01b Fluids Electrolytes Summary TablesVon HippoNo ratings yet
- Psychopharmacology-Mood StabilizerDocument5 pagesPsychopharmacology-Mood StabilizerVon Hippo100% (1)
- Adult Emergency PDFDocument2 pagesAdult Emergency PDFVon HippoNo ratings yet
- Recalls: 2nd Shifting ExamDocument13 pagesRecalls: 2nd Shifting ExamVon HippoNo ratings yet
- Child PsychiatryDocument6 pagesChild PsychiatryVon HippoNo ratings yet
- Psychiatric EmergencyDocument3 pagesPsychiatric EmergencyVon HippoNo ratings yet
- CLINPATH Finals ReviewerDocument28 pagesCLINPATH Finals ReviewerVon HippoNo ratings yet
- Brainstem Lesions Trans 2019 PDFDocument8 pagesBrainstem Lesions Trans 2019 PDFVon HippoNo ratings yet
- Abdominal: Al HerniaDocument3 pagesAbdominal: Al HerniaVon Hippo100% (1)
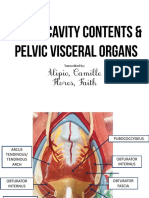
- Alipio, Camille Flores, Faith: Transcribed byDocument7 pagesAlipio, Camille Flores, Faith: Transcribed byVon HippoNo ratings yet
- Motor System: Three Types of Movement Generated by Motor SystemDocument10 pagesMotor System: Three Types of Movement Generated by Motor SystemVon Hippo100% (1)
- Book: - RecordingDocument8 pagesBook: - RecordingVon HippoNo ratings yet
- 1) Any Medical Student or GraduateDocument27 pages1) Any Medical Student or GraduateVon HippoNo ratings yet
- Renal Cell CarcinomaDocument3 pagesRenal Cell CarcinomaVon HippoNo ratings yet
- Compilation of Platings in MicrobiologyDocument6 pagesCompilation of Platings in MicrobiologyVon HippoNo ratings yet
- Internal Medicine - Nephrology: Topic: Cystic Kidney Diseases Lecturer: Dra. Myrna NgoDocument3 pagesInternal Medicine - Nephrology: Topic: Cystic Kidney Diseases Lecturer: Dra. Myrna NgoVon HippoNo ratings yet
- Biochem: Gene Expression Part 2: Recap of Transcription (Part 1 of Lecture)Document14 pagesBiochem: Gene Expression Part 2: Recap of Transcription (Part 1 of Lecture)Von HippoNo ratings yet
- Clinical Scenario: CPT Case 9 Neonatal SepsisDocument15 pagesClinical Scenario: CPT Case 9 Neonatal SepsisVon HippoNo ratings yet
- NEPHRO - Renal Stones PDFDocument3 pagesNEPHRO - Renal Stones PDFVon HippoNo ratings yet
- 2013 Compiled para Exams and Shiftings PDFDocument27 pages2013 Compiled para Exams and Shiftings PDFVon HippoNo ratings yet
- You Are The Reason PDFDocument1 pageYou Are The Reason PDFLachlan CourtNo ratings yet
- Picc Lite ManualDocument366 pagesPicc Lite Manualtanny_03No ratings yet
- Micro TeachingDocument3 pagesMicro Teachingapi-273530753No ratings yet
- Symptoms: Generalized Anxiety Disorder (GAD)Document3 pagesSymptoms: Generalized Anxiety Disorder (GAD)Nur WahyudiantoNo ratings yet
- Java Magazine JanuaryFebruary 2013Document93 pagesJava Magazine JanuaryFebruary 2013rubensaNo ratings yet
- TOURISM AND HOSPITALITY ORGANIZATIONS Di Pa TapooosDocument97 pagesTOURISM AND HOSPITALITY ORGANIZATIONS Di Pa TapooosDianne EvangelistaNo ratings yet
- 978-1119504306 Financial Accounting - 4thDocument4 pages978-1119504306 Financial Accounting - 4thtaupaypayNo ratings yet
- Economics and Agricultural EconomicsDocument28 pagesEconomics and Agricultural EconomicsM Hossain AliNo ratings yet
- Astm D1895 17Document4 pagesAstm D1895 17Sonia Goncalves100% (1)
- Task 1: MonologueDocument4 pagesTask 1: MonologueLaura Cánovas CabanesNo ratings yet
- Pharmaniaga Paracetamol Tablet: What Is in This LeafletDocument2 pagesPharmaniaga Paracetamol Tablet: What Is in This LeafletWei HangNo ratings yet
- User Manual For Inquisit's Attentional Network TaskDocument5 pagesUser Manual For Inquisit's Attentional Network TaskPiyush ParimooNo ratings yet
- Educ 3 Prelim Act.1 AlidonDocument2 pagesEduc 3 Prelim Act.1 AlidonJonash AlidonNo ratings yet
- The Leaders of The NationDocument3 pagesThe Leaders of The NationMark Dave RodriguezNo ratings yet
- лк CUDA - 1 PDCnDocument31 pagesлк CUDA - 1 PDCnОлеся БарковськаNo ratings yet
- Fort - Fts - The Teacher and ¿Mommy Zarry AdaptaciónDocument90 pagesFort - Fts - The Teacher and ¿Mommy Zarry AdaptaciónEvelin PalenciaNo ratings yet
- Kumar-2011-In Vitro Plant Propagation A ReviewDocument13 pagesKumar-2011-In Vitro Plant Propagation A ReviewJuanmanuelNo ratings yet
- Literatures of The World: Readings For Week 4 in LIT 121Document11 pagesLiteratures of The World: Readings For Week 4 in LIT 121April AcompaniadoNo ratings yet
- The Eaglet - Vol. 31, No. 3 - September 2019Document8 pagesThe Eaglet - Vol. 31, No. 3 - September 2019Rebecca LovettNo ratings yet
- Iii. The Impact of Information Technology: Successful Communication - Key Points To RememberDocument7 pagesIii. The Impact of Information Technology: Successful Communication - Key Points To Remembermariami bubuNo ratings yet
- Damodaram Sanjivayya National Law University VisakhapatnamDocument6 pagesDamodaram Sanjivayya National Law University VisakhapatnamSuvedhya ReddyNo ratings yet
- MGT 601-Smes Management MCQ For Final Term Preparation: ProductionDocument80 pagesMGT 601-Smes Management MCQ For Final Term Preparation: ProductionSajidmehsudNo ratings yet
- FCAPSDocument5 pagesFCAPSPablo ParreñoNo ratings yet
- Repair and Field Service BrochureDocument4 pagesRepair and Field Service Brochurecorsini999No ratings yet
- Meditation For AddictionDocument2 pagesMeditation For AddictionharryNo ratings yet
- Basics of An Model United Competition, Aippm, All India Political Parties' Meet, Mun Hrishkesh JaiswalDocument7 pagesBasics of An Model United Competition, Aippm, All India Political Parties' Meet, Mun Hrishkesh JaiswalHRISHIKESH PRAKASH JAISWAL100% (1)
- CS 124/LINGUIST 180 From Languages To Information: Conversational AgentsDocument58 pagesCS 124/LINGUIST 180 From Languages To Information: Conversational AgentsamanNo ratings yet
- Iluminadores y DipolosDocument9 pagesIluminadores y DipolosRamonNo ratings yet
- Wastewater Treatment: Sudha Goel, Ph.D. Department of Civil Engineering, IIT KharagpurDocument33 pagesWastewater Treatment: Sudha Goel, Ph.D. Department of Civil Engineering, IIT KharagpurSubhajit BagNo ratings yet
- The Rise of Political Fact CheckingDocument17 pagesThe Rise of Political Fact CheckingGlennKesslerWPNo ratings yet