You might also like
- Dissociative Spectrum Disorders in The Primary Care Setting: One Personal Copy May Be PrintedDocument5 pagesDissociative Spectrum Disorders in The Primary Care Setting: One Personal Copy May Be PrintedprematellieNo ratings yet
- Borderline Personality Disorder: Dialectical Behavior Therapy Workbook, Complete DBT Guide to Recovering from Borderline Personality DisorderFrom EverandBorderline Personality Disorder: Dialectical Behavior Therapy Workbook, Complete DBT Guide to Recovering from Borderline Personality DisorderNo ratings yet
- Psychiatry For Medical Students and ResidentsDocument80 pagesPsychiatry For Medical Students and ResidentsNabeel Kouka, MD, DO, MBA, MPH100% (4)
- Psychiatry Image BankDocument117 pagesPsychiatry Image BankSameeksha DasNo ratings yet
- Occupational Therapy Initial EvaluationDocument10 pagesOccupational Therapy Initial EvaluationNerissa BanguiNo ratings yet
- Psychopharmacology-Mood StabilizerDocument5 pagesPsychopharmacology-Mood StabilizerVon Hippo100% (1)
- EmotionalDocument7 pagesEmotionalapi-367611011No ratings yet
- Complex Trauma in Children PDFDocument9 pagesComplex Trauma in Children PDFMargaret MelviNo ratings yet
- Ob Gyne PDFDocument27 pagesOb Gyne PDFVon HippoNo ratings yet
- Psychiatry EoY History SampleDocument11 pagesPsychiatry EoY History SampleNicholasNo ratings yet
- 3 - Clinical Assessment, Diagnosis, and Research MethodsDocument12 pages3 - Clinical Assessment, Diagnosis, and Research Methodsapi-3855346100% (1)
- Mental Status Examination Psychiatric Nursing Assessment SpeechDocument2 pagesMental Status Examination Psychiatric Nursing Assessment SpeechElaine Louise O. Foronda100% (1)
- Purboyo Solek-Autism and Attention Deficit Hyperactivity Disorder (ADHD) FiDocument38 pagesPurboyo Solek-Autism and Attention Deficit Hyperactivity Disorder (ADHD) FiSupri Adi100% (2)
- Joint and Connective Tissue Disorders: QuestionsDocument11 pagesJoint and Connective Tissue Disorders: QuestionsVon HippoNo ratings yet
- Assessment of Mental RetardationDocument56 pagesAssessment of Mental Retardationdrkadiyala2No ratings yet
- PSYCHIATRIC DISORDERS OF CHILDHOOD (Autosaved)Document43 pagesPSYCHIATRIC DISORDERS OF CHILDHOOD (Autosaved)Amy Lalringhluani Chhakchhuak100% (1)
- #1-NCM 109 - TransesDocument10 pages#1-NCM 109 - TransesJaimie BanaagNo ratings yet
- Pre-Final Ncm116 - Disorders in Childhood and AdolescenceDocument6 pagesPre-Final Ncm116 - Disorders in Childhood and AdolescenceMyat LluvidoNo ratings yet
- Psych Nursing LectureDocument449 pagesPsych Nursing LectureButch DumdumNo ratings yet
- Reconstructive Surgery: Wei, F., Mardini, S. 2017. Flaps and Reconstructive Surgery 2 Edition. PG 1-3Document7 pagesReconstructive Surgery: Wei, F., Mardini, S. 2017. Flaps and Reconstructive Surgery 2 Edition. PG 1-3ninroseNo ratings yet
- NCP StrokeDocument7 pagesNCP StrokeMonica Gagarin Cortez100% (1)
- Brainstem Lesions Trans 2019 PDFDocument8 pagesBrainstem Lesions Trans 2019 PDFVon HippoNo ratings yet
- Mental RetardationDocument49 pagesMental RetardationRENJULAL100% (4)
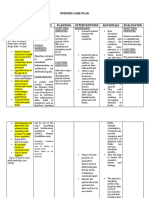
- Nursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationDocument8 pagesNursing Care Plan Diarrhea Assessment Diagnosis Planning Interventions Rationale EvaluationKrahNo ratings yet
- Effectiveness of TECAR Therapy and Therapeutic Exercise in The Treatment of Musculoskeletal Conditions A Review ArticleDocument4 pagesEffectiveness of TECAR Therapy and Therapeutic Exercise in The Treatment of Musculoskeletal Conditions A Review ArticleInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Cues/ Data Cues/ Data: Family Nursing Problem Family Nursing ProblemDocument14 pagesCues/ Data Cues/ Data: Family Nursing Problem Family Nursing ProblemAriane Rose Saria CedronNo ratings yet
- SARS PathophysioDocument2 pagesSARS PathophysioLouise BravoNo ratings yet
- Child and Adolescent Behavioral Health: A Resource for Advanced Practice Psychiatric and Primary Care Practitioners in NursingFrom EverandChild and Adolescent Behavioral Health: A Resource for Advanced Practice Psychiatric and Primary Care Practitioners in NursingEdilma L. YearwoodNo ratings yet
- SERETIDEDocument3 pagesSERETIDETempoNo ratings yet
- Matrix of ExceptionalitiesDocument2 pagesMatrix of ExceptionalitiesEhya AbetriaNo ratings yet
- Mental Retardation Lesson PlanDocument10 pagesMental Retardation Lesson Plansp2056251No ratings yet
- Mental Retardation: Costes - Doqueza - Mendiola - Oco - TapasDocument28 pagesMental Retardation: Costes - Doqueza - Mendiola - Oco - TapasEula Angelica OcoNo ratings yet
- Mental Retardation and Learning DisordersDocument4 pagesMental Retardation and Learning Disorderssarguss14100% (1)
- A Rare Case of Early Onset Bipolar Affective Disorder During LockdownDocument1 pageA Rare Case of Early Onset Bipolar Affective Disorder During LockdownRupinder GillNo ratings yet
- Chronic Schizophrenia: Medical Colleges of Northern PhilippinesDocument24 pagesChronic Schizophrenia: Medical Colleges of Northern Philippinesmark OrpillaNo ratings yet
- CMH 1Document25 pagesCMH 1Mirgank TirkhaNo ratings yet
- A Rare Case of Early-Onset Bipolar Affective Disorder During LockdownDocument1 pageA Rare Case of Early-Onset Bipolar Affective Disorder During LockdownRupinder GillNo ratings yet
- Assessment 4 (BE)Document9 pagesAssessment 4 (BE)Aryan Judith DoloresNo ratings yet
- Health Assessment LecDocument4 pagesHealth Assessment LecKyla RamonesNo ratings yet
- Ha Lab Sas 21 Magbanua Glory Mae Paciol BSN1 A18 PDFDocument7 pagesHa Lab Sas 21 Magbanua Glory Mae Paciol BSN1 A18 PDFCallie ParkNo ratings yet
- CSB 341Document48 pagesCSB 341TessNo ratings yet
- Personality Development and Intellectual DisabilityDocument5 pagesPersonality Development and Intellectual DisabilityRuxiFuxiNo ratings yet
- Behavioral DisorderDocument2 pagesBehavioral DisorderJeffrey FostanesNo ratings yet
- Lecture 8 NotesDocument3 pagesLecture 8 NotesAafreen AhmedNo ratings yet
- TGBP Session 3 Intellectual Disability CNSP PDFDocument100 pagesTGBP Session 3 Intellectual Disability CNSP PDFjlpabalan.tasiNo ratings yet
- Psychiatric NursingDocument5 pagesPsychiatric NursingcelestineNo ratings yet
- P - SMA Negeri 2 Kudus - Petrus Lintang Sutami Krisdianto Dan Rusdita Nabila Putri - Makalah - Nas2020-DikonversiDocument4 pagesP - SMA Negeri 2 Kudus - Petrus Lintang Sutami Krisdianto Dan Rusdita Nabila Putri - Makalah - Nas2020-Dikonversiayo ambiss 22No ratings yet
- FizaaaaaDocument34 pagesFizaaaaajiyanshi yadavNo ratings yet
- Early Onset SchizophreniaDocument3 pagesEarly Onset SchizophreniaDoc Prince CaballeroNo ratings yet
- Introduction To Mental Health Care of People With Intellectual DisabilityDocument65 pagesIntroduction To Mental Health Care of People With Intellectual DisabilityFrancois CreweNo ratings yet
- Intellectualy Challenged: Sports, Social, and Recreational ActivitiesDocument2 pagesIntellectualy Challenged: Sports, Social, and Recreational ActivitiesLashawna BridgewaterNo ratings yet
- AP PsychologyDocument5 pagesAP PsychologyJiwon ShinNo ratings yet
- Behavioral Health Care PlanDocument9 pagesBehavioral Health Care Planapi-520634647No ratings yet
- Study Feature Paper 1 Paper 2 Paper 3Document8 pagesStudy Feature Paper 1 Paper 2 Paper 3api-287714993No ratings yet
- Psychosocial, Behavioral, and Medical Outcomes in Children WithDocument9 pagesPsychosocial, Behavioral, and Medical Outcomes in Children WithvicraadhityaNo ratings yet
- Behavioral Health Care PlanDocument10 pagesBehavioral Health Care Planapi-520664738No ratings yet
- Potang Ina ReviewerDocument23 pagesPotang Ina ReviewerBrix RamiterreNo ratings yet
- AbPsy DevPsy Tanginang Buhay ToDocument49 pagesAbPsy DevPsy Tanginang Buhay ToBrix RamiterreNo ratings yet
- Research - Plan - Proposal SudhaDocument28 pagesResearch - Plan - Proposal SudhaEisha ShahnawazNo ratings yet
- Attention-Deficit/Hyperactivity Disorder: Thomas J. Spencer, MDDocument3 pagesAttention-Deficit/Hyperactivity Disorder: Thomas J. Spencer, MDJesica AlvarezNo ratings yet
- What Is Mental Health?: "Caring For Your Mental Health Amidst The Challenges and Change"Document23 pagesWhat Is Mental Health?: "Caring For Your Mental Health Amidst The Challenges and Change"amelito m. lingaNo ratings yet
- Cpe 103 Module 4 Typology of Learners Trisomy21 FinalDocument34 pagesCpe 103 Module 4 Typology of Learners Trisomy21 FinalAnamilah ManingcaraNo ratings yet
- Reconceptualizing Mental Heathcare Facilities: Role Architecture Plays in Improving One'S SanityDocument14 pagesReconceptualizing Mental Heathcare Facilities: Role Architecture Plays in Improving One'S SanityDEEPNo ratings yet
- Lidwien Kok, Anne Van Der Waa, Helen Klip and Wouter StaalDocument16 pagesLidwien Kok, Anne Van Der Waa, Helen Klip and Wouter StaalJulian Caro MorenoNo ratings yet
- Health Talk Mental RetardationDocument10 pagesHealth Talk Mental RetardationSanjeevNo ratings yet
- Trevarthen, C., & Aitken, K. J IntersubjetividadDocument46 pagesTrevarthen, C., & Aitken, K. J IntersubjetividadMariluzNo ratings yet
- Community HealthDocument5 pagesCommunity HealthMiguel C. DolotNo ratings yet
- Abnormal Psychology (Last Discussion)Document18 pagesAbnormal Psychology (Last Discussion)FLORLYN VERALNo ratings yet
- Psychology 3E: Saundra K. Ciccarelli, J. Noland WhiteDocument40 pagesPsychology 3E: Saundra K. Ciccarelli, J. Noland WhiteJansen WongNo ratings yet
- Genes, Memes, Culture, and Mental Illness: Toward an Integrative ModelFrom EverandGenes, Memes, Culture, and Mental Illness: Toward an Integrative ModelRating: 4 out of 5 stars4/5 (1)
- Leptospirosis Policy StatementsDocument6 pagesLeptospirosis Policy StatementsKay RuzNo ratings yet
- Adnexal Mass in Pregnancy UpToDate PDFDocument21 pagesAdnexal Mass in Pregnancy UpToDate PDFVon HippoNo ratings yet
- KissPrep-Anatomy Physiology PDFDocument1 pageKissPrep-Anatomy Physiology PDFVon HippoNo ratings yet
- Urinary Tract Infection (Book) : NephrologyDocument4 pagesUrinary Tract Infection (Book) : NephrologyVon HippoNo ratings yet
- Diagnostic Performance of International Ovarian Tumor Analysis IotaDocument7 pagesDiagnostic Performance of International Ovarian Tumor Analysis IotaVon HippoNo ratings yet
- Gyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesDocument8 pagesGyne 2.6 - Benign and Malignant Tumors of The Ovaries and Fallopian TubesVon HippoNo ratings yet
- Suicide, Psychiatric Emergency, Substance Abuse PDFDocument14 pagesSuicide, Psychiatric Emergency, Substance Abuse PDFVon HippoNo ratings yet
- Psychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersDocument11 pagesPsychiatric 3: Substance Abuse (DR Rosales) : Substance Use Related DisordersVon HippoNo ratings yet
- Psychiatric 3: Suicide (DR Rosales) June 8, 2011Document4 pagesPsychiatric 3: Suicide (DR Rosales) June 8, 2011Von HippoNo ratings yet
- Recalls: 2nd Shifting ExamDocument13 pagesRecalls: 2nd Shifting ExamVon HippoNo ratings yet
- Psychiatric 3: Suicide (DR Rosales) June 8, 2011Document4 pagesPsychiatric 3: Suicide (DR Rosales) June 8, 2011Von HippoNo ratings yet
- Adult Emergency PDFDocument2 pagesAdult Emergency PDFVon HippoNo ratings yet
- Psychiatric EmergencyDocument3 pagesPsychiatric EmergencyVon HippoNo ratings yet
- PEDIA2 2.01b Fluids Electrolytes Summary TablesDocument4 pagesPEDIA2 2.01b Fluids Electrolytes Summary TablesVon HippoNo ratings yet
- Abdominal: Al HerniaDocument3 pagesAbdominal: Al HerniaVon Hippo100% (1)
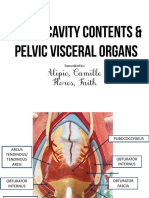
- Alipio, Camille Flores, Faith: Transcribed byDocument7 pagesAlipio, Camille Flores, Faith: Transcribed byVon HippoNo ratings yet
- Motor System: Three Types of Movement Generated by Motor SystemDocument10 pagesMotor System: Three Types of Movement Generated by Motor SystemVon Hippo100% (1)
- CLINPATH Finals ReviewerDocument28 pagesCLINPATH Finals ReviewerVon HippoNo ratings yet
- 1) Any Medical Student or GraduateDocument27 pages1) Any Medical Student or GraduateVon HippoNo ratings yet
- Vitamins B ComplexDocument4 pagesVitamins B ComplexVon HippoNo ratings yet
- Gold 2019 Pocket Guide Final WmsDocument49 pagesGold 2019 Pocket Guide Final WmsFrensi Ayu PrimantariNo ratings yet
- Book: - RecordingDocument8 pagesBook: - RecordingVon HippoNo ratings yet
- Fluid and Electrolytes YMDocument8 pagesFluid and Electrolytes YMVon HippoNo ratings yet
- Patho B Prelims RBCDocument12 pagesPatho B Prelims RBCVon HippoNo ratings yet
- Clinical Scenario: CPT Case 9 Neonatal SepsisDocument15 pagesClinical Scenario: CPT Case 9 Neonatal SepsisVon HippoNo ratings yet
- Medical-Surgical Nursing Care: Caring For Clients With Diabetes MellitusDocument90 pagesMedical-Surgical Nursing Care: Caring For Clients With Diabetes MellitusJonalynCollodChewacheoNo ratings yet
- 2.tukak PeptikDocument42 pages2.tukak PeptikEfvi VhyLiaNo ratings yet
- Sensory Practice TestDocument19 pagesSensory Practice TestJennelyn GinturoNo ratings yet
- What Are Bacteria - Streptococcus FaecalisDocument3 pagesWhat Are Bacteria - Streptococcus FaecalisAnkan PalNo ratings yet
- Clinical Practicum Worksheet: Nursing Care PlanDocument4 pagesClinical Practicum Worksheet: Nursing Care PlanOrlea Francisco-SisioNo ratings yet
- Information Sheet 4.1-4: 1. Occupational Health and Safety IndicatorsDocument3 pagesInformation Sheet 4.1-4: 1. Occupational Health and Safety Indicatorsmark ian joverNo ratings yet
- Nosocomial Infections: Causes, Controls, Preventions and Future ChallengesDocument11 pagesNosocomial Infections: Causes, Controls, Preventions and Future ChallengesAy GlassesNo ratings yet
- Amniotic Fluid and Placenta AbnormalitiesDocument60 pagesAmniotic Fluid and Placenta AbnormalitiesMicah Lou CalambaNo ratings yet
- Errata of QbankDocument29 pagesErrata of QbankSaba WaheedNo ratings yet
- Evaluation and Treatment of Hypertensive Emergencies in AdultsDocument13 pagesEvaluation and Treatment of Hypertensive Emergencies in Adultsjavier ariasNo ratings yet
- Renal Board ReviewDocument27 pagesRenal Board ReviewyumminNo ratings yet
- OsteoarthritisDocument11 pagesOsteoarthritisadddNo ratings yet
- Klasifikasi Penyebab KomaDocument19 pagesKlasifikasi Penyebab KomaNoni JacksonNo ratings yet
- First Conditional: "If You Fall, I Will Be There." - The FloorDocument3 pagesFirst Conditional: "If You Fall, I Will Be There." - The FloorgastonNo ratings yet
- Arizona Communicable Disease FlipchartDocument98 pagesArizona Communicable Disease Flipchartapi-308905421No ratings yet
- Inherited Metabolic Disorders Are Genetic Conditions That Result in Metabolism ProblemsDocument10 pagesInherited Metabolic Disorders Are Genetic Conditions That Result in Metabolism ProblemsLance CornistaNo ratings yet
- Test Yourself: MCQ and Extended MatchingDocument2 pagesTest Yourself: MCQ and Extended MatchingPhil ChanNo ratings yet
- DAFTAR PUSTAKA Referat Ca MammaeDocument5 pagesDAFTAR PUSTAKA Referat Ca MammaeAulia JanerNo ratings yet
- Medical Certificate (To Be Issued by A Registered Medical Practitioner) General ExpectationsDocument1 pageMedical Certificate (To Be Issued by A Registered Medical Practitioner) General ExpectationsShubham KhandelwalNo ratings yet
- Graha Roga'sDocument10 pagesGraha Roga'srohinibrajole123No ratings yet
- Untitled Document 22Document5 pagesUntitled Document 22api-609568172No ratings yet