You might also like
- Gastroenterology For General SurgeonsFrom EverandGastroenterology For General SurgeonsMatthias W. WichmannNo ratings yet
- NCP Tumor Wilms: Ni Nyoman Udiani, S.Kep.,Ns.,M.KepDocument37 pagesNCP Tumor Wilms: Ni Nyoman Udiani, S.Kep.,Ns.,M.KepClaudia NatasyaNo ratings yet
- Wilms Tumor Nursing CareDocument19 pagesWilms Tumor Nursing CareReni OktaviaNo ratings yet
- Common Pediatric Malignancies: Wilms Tumor and NeuroblastomaDocument34 pagesCommon Pediatric Malignancies: Wilms Tumor and NeuroblastomanazymalfikryNo ratings yet
- Introduction To Child With Onchological DisorderDocument16 pagesIntroduction To Child With Onchological DisorderAsha jiluNo ratings yet
- Wilms Tumour: Nitha K 2 Year MSC NursingDocument40 pagesWilms Tumour: Nitha K 2 Year MSC NursingNITHA K100% (1)
- Tumor Wilms NephroblastomaDocument8 pagesTumor Wilms NephroblastomaRisal FoengNo ratings yet
- Tumor Pada AnakDocument65 pagesTumor Pada Anakdr.cintaNo ratings yet
- Wilms Tumor NelsonDocument8 pagesWilms Tumor NelsonvegaNo ratings yet
- Wilms TumorDocument6 pagesWilms TumorJennyDanielNo ratings yet
- WT by WorkuDocument24 pagesWT by Workuworku asfawNo ratings yet
- NephroblastomaDocument26 pagesNephroblastomaRahul Dhaker100% (3)
- Wilms Tumor in Children: Causes, Symptoms, Staging and TreatmentDocument3 pagesWilms Tumor in Children: Causes, Symptoms, Staging and TreatmentPrasetya Ismail PermadiNo ratings yet
- Wilms' Tumour (Nephroblastoma) : EpidemiologyDocument3 pagesWilms' Tumour (Nephroblastoma) : EpidemiologyPauleen Trisha SamparaniNo ratings yet
- Kyle Essentials of Pediatric Nursing 2nd c2013 TXTBK 1295 1297Document3 pagesKyle Essentials of Pediatric Nursing 2nd c2013 TXTBK 1295 12972003027 Orysa Ann YudhistyNo ratings yet
- Ovarian CA 450918 ShDocument52 pagesOvarian CA 450918 Sh180045No ratings yet
- Anesthetic Considerations for Pediatric Patients with Wilms' TumorDocument10 pagesAnesthetic Considerations for Pediatric Patients with Wilms' Tumorlinhohb4833No ratings yet
- Breast CancerDocument9 pagesBreast CancerLilia Tejada AlmonteNo ratings yet
- TumourDocument32 pagesTumourzainabd1964No ratings yet
- Leukemia Cells & ColorectalDocument40 pagesLeukemia Cells & ColorectalYum CNo ratings yet
- Nephroblastoma in Children (Wilm's Tumor)Document24 pagesNephroblastoma in Children (Wilm's Tumor)Yankurije TheophileNo ratings yet
- Nephroblastoma FinalDocument24 pagesNephroblastoma FinalKrissy_Singh_211No ratings yet
- Pielonefritis Kronis: Tujuan PraktikumDocument12 pagesPielonefritis Kronis: Tujuan PraktikumFp Cyninthia KennedyNo ratings yet
- Wilms TumorDocument24 pagesWilms TumorROXTA RAHULNo ratings yet
- Malignant Ovarian TumourDocument46 pagesMalignant Ovarian Tumourahmed shorshNo ratings yet
- Case Analysis DR RinaDocument30 pagesCase Analysis DR RinaCindy PrayogoNo ratings yet
- Understanding Wilms Tumor - A Guide for CliniciansDocument58 pagesUnderstanding Wilms Tumor - A Guide for CliniciansMona MorrisNo ratings yet
- Renal Tumor: Oleh: I Made Andi Saputra Pembimbing: Dr. Munawir, SP - BaDocument22 pagesRenal Tumor: Oleh: I Made Andi Saputra Pembimbing: Dr. Munawir, SP - Baimadeandi saputraNo ratings yet
- Chapter 4 Wilms Tumor and Its Management in A Surgical AspectDocument10 pagesChapter 4 Wilms Tumor and Its Management in A Surgical AspectchimbimbNo ratings yet
- Tumor IntraabdomenDocument30 pagesTumor IntraabdomenBedahanakugmNo ratings yet
- Rare Kidney Cancer in ChildrenDocument12 pagesRare Kidney Cancer in ChildrenKath CamachoNo ratings yet
- Nephroblastoma: Rahul DhakerDocument34 pagesNephroblastoma: Rahul DhakerRahul Dhaker100% (1)
- Wilms' Tumor 2014Document18 pagesWilms' Tumor 2014api-282060573No ratings yet
- OBGYN Revision NotesDocument9 pagesOBGYN Revision NotesJoanne Bowers100% (3)
- Wilm'S Tumor IDocument25 pagesWilm'S Tumor IBiancaGabatinoAbarca100% (1)
- Abdominal Tumors in ChildrenDocument25 pagesAbdominal Tumors in Children'Sebastián FerreroNo ratings yet
- Wilms' Tumor or Wilms' Tumour (SeeDocument9 pagesWilms' Tumor or Wilms' Tumour (SeeGretchen BugarinNo ratings yet
- Gastric Cancer by BalaDocument17 pagesGastric Cancer by BalaArundeep AsaithambiNo ratings yet
- Benign Lesions of The OvariesDocument12 pagesBenign Lesions of The OvariesdocjosmaNo ratings yet
- Childhood Malignancies PP - Copy 2Document46 pagesChildhood Malignancies PP - Copy 2ugonna nwokeNo ratings yet
- Renal Tumors RCC Renal Cells Carcinoma Renal Adenocarcinoma HypernephromaDocument5 pagesRenal Tumors RCC Renal Cells Carcinoma Renal Adenocarcinoma HypernephromaMohamed Al-zichrawyNo ratings yet
- Pediatrics in Review 2013 Friedman 328 30Document5 pagesPediatrics in Review 2013 Friedman 328 30Enrique CaballéNo ratings yet
- OncologyDocument66 pagesOncologyMaria Sofia Stephanie SatoriNo ratings yet
- Wils TumorDocument19 pagesWils TumorjolibeecaldonaNo ratings yet
- Assessment and Diagnosis of Abdominal Masses in Children: Resident Education Lecture SeriesDocument45 pagesAssessment and Diagnosis of Abdominal Masses in Children: Resident Education Lecture SeriesboubiyouNo ratings yet
- Cancer Cervix: BY Ahmed Magdy ElmohandesDocument34 pagesCancer Cervix: BY Ahmed Magdy ElmohandesAhmed ElmohandesNo ratings yet
- Wilms Tumor: Urology DepartmentDocument38 pagesWilms Tumor: Urology DepartmentHardiTariqHammaNo ratings yet
- Nephroblastoma (Wilm's Tumor)Document5 pagesNephroblastoma (Wilm's Tumor)dunhill26labanNo ratings yet
- Dr. E. J. Arteen F.R.C.S General & Colorectal Consultant SurgeonDocument65 pagesDr. E. J. Arteen F.R.C.S General & Colorectal Consultant SurgeonEslam R. Almassri100% (1)
- Metastatic Kidney Cancer in ChildrenDocument29 pagesMetastatic Kidney Cancer in ChildrenAnusha Verghese100% (2)
- Wilms Tumor: by Nuzul AlimiDocument14 pagesWilms Tumor: by Nuzul AlimiNu JoeNo ratings yet
- Bladder Cancer 1Document31 pagesBladder Cancer 1Anas HamadNo ratings yet
- Prune Belly SyndromeDocument39 pagesPrune Belly SyndromeHudaNo ratings yet
- Endometrial NeoplasiaDocument48 pagesEndometrial NeoplasiaBONI M.WoyessaNo ratings yet
- 6. Ovarian MalignancyDocument51 pages6. Ovarian MalignancydeepaNo ratings yet
- Benign and Malignant Lesion of Lower GIDocument45 pagesBenign and Malignant Lesion of Lower GIAhmad Alzu3beNo ratings yet
- Pancreatic Tumours: Types, Causes, Symptoms and TreatmentDocument33 pagesPancreatic Tumours: Types, Causes, Symptoms and TreatmentAdil ShabbirNo ratings yet
- PNP NCM 103Document6 pagesPNP NCM 103Mark Joseph Mabazza LappayNo ratings yet
- Hemicolectomy GuideDocument5 pagesHemicolectomy GuideMuhammad MalikNo ratings yet
- Association Between Working Memory Impairment and ActivitiesDocument6 pagesAssociation Between Working Memory Impairment and ActivitiesDaniel OrregoNo ratings yet
- O.level Human Bio Edexcel Past Papers Paper 1 2019 - 2020Document68 pagesO.level Human Bio Edexcel Past Papers Paper 1 2019 - 2020Tamer AhmedNo ratings yet
- FDAR For Urinary Tract InfectionDocument2 pagesFDAR For Urinary Tract InfectionElle Monge100% (1)
- A Clinical Decision Support Framework For Heterogeneous Data SourcesDocument10 pagesA Clinical Decision Support Framework For Heterogeneous Data SourcesdineshshaNo ratings yet
- OlanzapineDocument1 pageOlanzapineKallie ChartrandNo ratings yet
- Case StudyDocument2 pagesCase StudyClaire MachicaNo ratings yet
- OBGYN Revalida Review 2019Document74 pagesOBGYN Revalida Review 2019anonymous100% (1)
- Pankaj Naram - CuresDocument14 pagesPankaj Naram - CuresArtlife1No ratings yet
- Chest PhysiotherapyDocument4 pagesChest Physiotherapyhakky gamyNo ratings yet
- Cardiac Myocytes CultureDocument6 pagesCardiac Myocytes CultureÉmerson MoreiraNo ratings yet
- Red Blood Cell Disorders Part 1 and 2Document7 pagesRed Blood Cell Disorders Part 1 and 2babael.zuher123No ratings yet
- BurtonFreeman Reimers2011Document12 pagesBurtonFreeman Reimers2011Della FitriaNo ratings yet
- Informed Consent Form: Covid-19Document3 pagesInformed Consent Form: Covid-19Yohana DahokloryNo ratings yet
- When and Where Did The First Quarantines Take Place?Document1 pageWhen and Where Did The First Quarantines Take Place?Raghavendra SharmaNo ratings yet
- MCQ Exam Questions (Faculty Pediatrics 2019-2020) .: Choleretics and Cholekinetics / HolenzimDocument20 pagesMCQ Exam Questions (Faculty Pediatrics 2019-2020) .: Choleretics and Cholekinetics / HolenzimKumar AdityaNo ratings yet
- NCM 116 - Nursing Care of Patients With Neurologic DysfunctionDocument11 pagesNCM 116 - Nursing Care of Patients With Neurologic DysfunctionRigel Kent C. TobiasNo ratings yet
- Surgical Option For Pediatric Bilateral Vocal Cord PalsyDocument9 pagesSurgical Option For Pediatric Bilateral Vocal Cord PalsyJeremy HermantoNo ratings yet
- 19 04 2020 Mumbai PDFDocument33 pages19 04 2020 Mumbai PDFShaji VkNo ratings yet
- West Minin CaseDocument2 pagesWest Minin CaseEUNICE MANATADNo ratings yet
- PI Kidmin 200 MLDocument2 pagesPI Kidmin 200 MLFayza AdelNo ratings yet
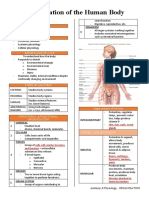
- Organization of the Human BodyDocument8 pagesOrganization of the Human BodyAly HannahNo ratings yet
- Zubiaga, R-Jeane S. - BSN 3 - For PlagscanDocument41 pagesZubiaga, R-Jeane S. - BSN 3 - For PlagscanR-Jeane ZubiagaNo ratings yet
- Detection of Cardiac Disorder Using MATLAB BasedDocument4 pagesDetection of Cardiac Disorder Using MATLAB BasedSeira LoyardNo ratings yet
- Corn Pest Surveillance Pre-Inception MeetingDocument41 pagesCorn Pest Surveillance Pre-Inception MeetingMarcJunardJoverNo ratings yet
- Introduction To Oncology and Palliative Care: Lecturer: Nadia ShamasnahDocument47 pagesIntroduction To Oncology and Palliative Care: Lecturer: Nadia ShamasnahXo Yem100% (1)
- Biochemistry Papers MSUDocument20 pagesBiochemistry Papers MSUShiv BhattNo ratings yet
- Lesson Plan Nephrotic SyndromeDocument9 pagesLesson Plan Nephrotic SyndromeEllen Angel50% (2)
- A Guide To Clinical Differential Diagnosis of Oral Mucosal LesionDocument46 pagesA Guide To Clinical Differential Diagnosis of Oral Mucosal LesionFasmiya ShariffNo ratings yet
- Kisi 2 B Ing - 230604 - 173816Document3 pagesKisi 2 B Ing - 230604 - 173816izzatul afifahNo ratings yet
- AARC Clinical Practice Guideline: Incentive SpirometryDocument10 pagesAARC Clinical Practice Guideline: Incentive SpirometrytruptimptNo ratings yet